Download presentation
Presentation is loading. Please wait.

1
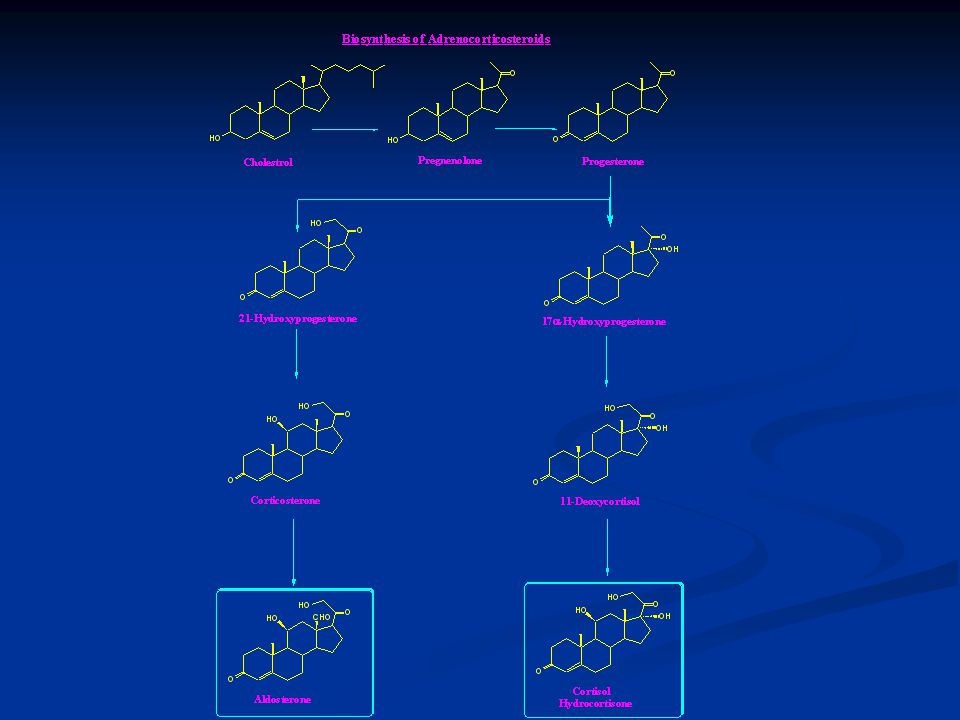
Steroidal Hormones (Adrenocorticosteroids, Adrenocorticoids, Corticosteroids, Corticoids)
Secretion: Adrenal cortex of the adrenal gland. Regulation: Stimulation: ACTH. Inhibition: Feed back Mechanism.

2
Classification of corticosteroids
They are all C21 hormones.

3
Numbering System of Steroidal ring:

5
Physiological Functions and Pharmacological Effects:
Carbohydrates and Proteins Metabolism: Stimulate glucose formation in the brain. Decrease peripheral utilization of glucose. Promote storage of glucose in the liver. Promote gluconeogenesis. Lipids Metabolism: Redistribution of body fat (Buffalo hump, Moon face). Enhance lipolyses of Triglycerides. Electrolyte and Water balance: Enhance reabsorption of sodium and water into plasma. Increase urinary excretion of potassium.
. Enhance lipolyses of Triglycerides. Electrolyte and Water balance: Enhance reabsorption of sodium and water into plasma. Increase urinary excretion of potassium.")
6
Anti-inflammatory effects:
Blood Picture: Increase hemoglobin and Red blood cells. Decrease white blood cells. Anti-inflammatory effects: Suppress inflammations regardless to their cause. Immunosuppressive Effects: Decrease immunity as a result of decrease the WBC’s. Cell Growth: Retardation of cell division and cell growth.

7
Disease States: Addison’s disease:
Rare syndrome 1/100,000 due to Hypoadrenalism. Causes: Atrophy of adrenal gland. Tuberculoses. Low level of ACTH. Symptoms: Weakness, fatigue, apathy, depression and irritability. Anemia and low blood pressure. Loss of sodium and dehydration. Hypersensitivity to Insulin. Hyper pigmentation. Nausea and vomiting.

8
Cushing’s disease: Conn’s syndrom:
Rare syndrome 2- 5/Million due to Hyperadrenalism. Causes: Tumor of the Adrenal Cortex. Tumor of the Pituitary gland. Symptoms: Alteration of fat distribution. Hypertension. Osteoporosis. Growth retardation. Decrease Immunity. Conn’s syndrom: Inability of adrenal cortex to carry out 17a-hydroxylation of pregnenolone. That leads to low level of Cortisol and high level of Aldosterone. Alkalosis. Polyuria. Edema.

9
Pharmacokinetics: Absorption: Plasma Protein binding:
Well absorbed from all sites of administration. Plasma Protein binding: 90% to albumin or globulin. Half life (t1/2): hr. Metabolism and Excretion: Excreted in urine after glycosylation with glucuronic acid.
: hr. Metabolism and Excretion: Excreted in urine after glycosylation with glucuronic acid.")
11
Adrenocorticoid Drugs
Systemic Corticosteroids: They can be administered by IV, IM injections, oral, topical or by inhalation. They can be short, intermediate or long-acting. Unlike natural corticoids they do not undergo first pass metabolism. Cortisone and Cortisone acetate: Can be given orally or by IM injection. Acetate has longer duration of action. Drug of choice in replacement therapy.

12
Prednisone and Prednisolone:
Fludrocortison: 9a-fluorocortisone. 10 times more active than cortisone as antiinflammatory. times more active as mineralocorticoids. Prednisone and Prednisolone: They are Δ1 corticoids. 3, 4 times more active than cortisone and hydrocortisone. Prepared by microbial dehydrogenation (Corynebacterium simplex) or chemically using SeO2.
 or chemically using SeO2.")
13
Triamcinolone: Dexamethasone: Betamethasone:
9a-fluoro, 16a-hydroxyprednisolone. Activity equal to prednidolone but with less mineralocorticoid activity. Dexamethasone: 9a-fluoro, 16a-methylprednisolone. 5- 7 times more active than prednidolone. Betamethasone: 9a-fluoro, 16b-methylprednisolone. Slightly more active than Dexamethasone.

14
Topical Corticosteroid:
Beclomethasone: 9a-fluoro, 16b-methylprednisolone. 9a-chloro analog of Betamethasone. Topical activity 500 times more than Betamethasone.

15
Inhaled Corticosteroids:
Beclomethasone 17, 21-dipropionate (BDP): Prodrug metabolized to more active 17-BMP. 17-BMP is 30 times more active than BDP. Topical activity 500 times more than Betamethasone. Triamcinolone Acetonide:
: Prodrug metabolized to more active 17-BMP. 17-BMP is 30 times more active than BDP. Topical activity 500 times more than Betamethasone. Triamcinolone Acetonide:")
16
Clinical uses: Hypoadrenalism. Rumatic diseases. Renal diseases.
Collagen diseases. Ocular diseases. Skin diseases. GIT inflammation. Liver diseases.

17
Diagnostic uses: Cause of Hyperadrenalism:
Non specific due to obesity or stress. Cushing’s syndrome. 2 mg Dexamethasone every 6 hr for 8 doses to diagnose the cause.

18
Side effects: Due to Prolonged use: Withdrawal Symptoms:
Fluid and electrolyte disturbances, edema and hypertension. Hyperglycemia and glucosuria. Peptic ulcer. Osteoporoses Myopathy Growth arrest Increase susceptibility to infections. Withdrawal Symptoms: Rapid withdrawal after prolonged use leads to sever hypoadrenalism.

Similar presentations









 are the triangle-shaped and orange- colored endocrine.>")



 Hormones.>")






