Download presentation
Presentation is loading. Please wait.

1
11 WAYS TO DECREASE DOOR TO NEEDLE TIME YOU CAN DO IT FASTER Jeff Nickel, MD FACEP ED Medical Director Parkview Regional Medical Center

2
TARGET STROKE A national quality improvement initiative of the American Heart Association/American Stroke Association to improve the care of stroke patients Phase 1 - Door to IV TPA goal was median time of <60 minutes Phase 2 – 75% <60 minutes. Median time 45 minutes Every 15 minute reduction in time has been shown to improve favorable outcomes by 4% With best practices we could get this down to 30-45 minutes

3
1) EMS PRE-NOTIFICATION EMS outreach and education Be aware of local hospitals capabilities Gather all significant history Notify ED as early as possible Relay patient name and information Bring witness/family member to ED with patient Initiate antecubital IV, collect blood, check sugar, bring medications if available. Register into EMR before arrival if possible

4
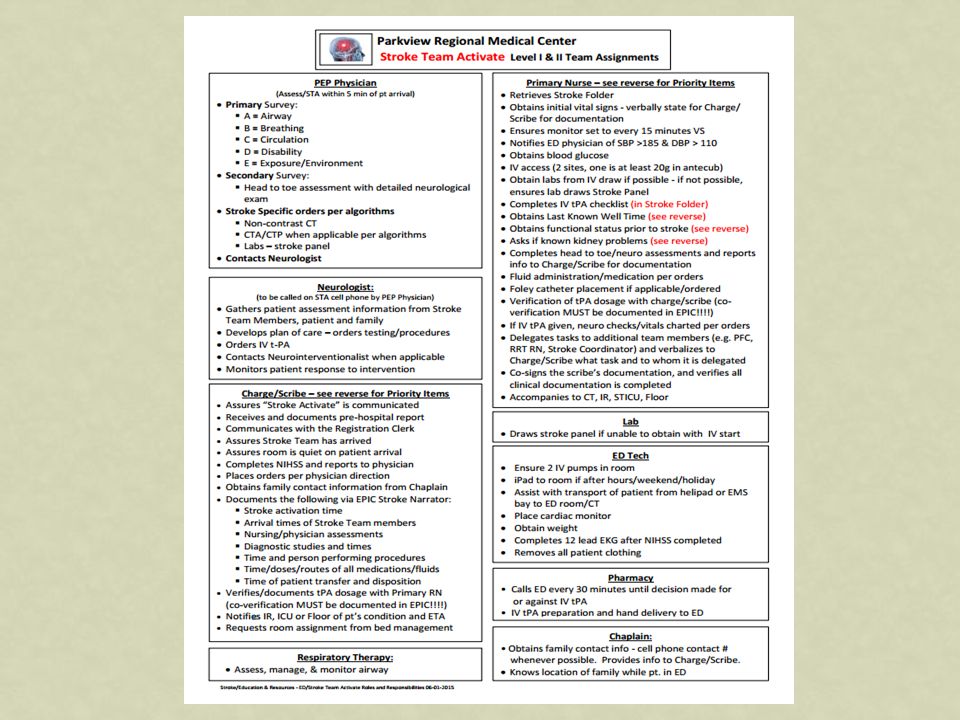
2) STROKE TOOLKIT Rapid triage protocol Stroke team member assignments Clinical decision support tool –TPA screening Checklist Specific order sets Critical pathways NIH Stroke Scale
 STROKE TOOLKIT Rapid triage protocol Stroke team member assignments Clinical decision support tool –TPA screening Checklist Specific order sets Critical pathways NIH Stroke Scale")
12
3) RAPID TRIAGE PROTOCOL AND STROKE TEAM NOTIFICATION Triage Protocols facilitate timely recognition of Stroke. Stroke team should be activated as soon as patient is identified pre-hospital or at triage Rapid neurologic evaluation should be performed ASAP in ED or on CT table NIH scale done ASAP

14
If pt. does not meet this screening criteria for neurointervention, neurologist paged by ED physician for consult as appropriate

18
4) SINGLE CALL ACTIVATION SYSTEM One call should activate the entire stroke team Includes ED staff, CT, Lab, Pharmacy, Neurologist, Radiologist, Chaplain, Stroke Team Nurses, Research Nurse, Stat Nurse, ICU Nurse, etc.
 SINGLE CALL ACTIVATION SYSTEM One call should activate the entire stroke team Includes ED staff, CT, Lab, Pharmacy, Neurologist, Radiologist, Chaplain, Stroke Team Nurses, Research Nurse, Stat Nurse, ICU Nurse, etc.")
19
5) TRANSFER DIRECTLY TO CT Eligible stroke patients, if appropriate should go directly to CT from ambulance or triage Protocols to ensure patients requiring emergency medical assessment or stabilization are not directly triaged to CT Get patient weight on gurney or CT table if possible Physician evaluation and NIH scale can be obtained in CT
 TRANSFER DIRECTLY TO CT Eligible stroke patients, if appropriate should go directly to CT from ambulance or triage Protocols to ensure patients requiring emergency medical assessment or stabilization are not directly triaged to CT Get patient weight on gurney or CT table if possible Physician evaluation and NIH scale can be obtained in CT")
20
6) RAPID INTERPRETATION OF CT Initial plain CT only. Delay advanced imaging until it is determined patient is not a TPA candidate Consider Radiologist or Neurologist in CT scanner for real time interpretation Acquisition time should be within 20 minutes of arrival and complete interpretation within 35 minutes of arrival

21
7) RAPID LABORATORY TESTING Draw blood pre-hospital or upon arrival Glucose, Glucose, Glucose Point of care testing Lab turn around time should be less than 30 minutes, prioritize INR and platelets If patient is not are risk for coagulation defect and not on anticoagulants, consider not delaying tpa while waiting on results
 RAPID LABORATORY TESTING Draw blood pre-hospital or upon arrival Glucose, Glucose, Glucose Point of care testing Lab turn around time should be less than 30 minutes, prioritize INR and platelets If patient is not are risk for coagulation defect and not on anticoagulants, consider not delaying tpa while waiting on results")
22
8) MIX TPA AHEAD OF TIME TPA stored in ED has been shown to reduce administration time If stored in pharmacy, pharmacist must be notified immediately on patient arrival and given patients weight. Mix the TPA when a potential patient is identified Manufacturer will replace unused thrombolytic free of charge

23
9) RAPID ACCESS AND ADMINISTRATION OF TPA Only one IV necessary initially, start second when possible Bolus should be given ASAP even on CT table if possible. Drip should be started immediately. One nurse can give bolus while second is preparing and priming drip. Have your TPA administration protocol in your stroke tool kit

24
10) TEAM-BASED APPROACH Team approach based on standardized stroke pathways and protocols has proven to be effective in enhancing the number of eligible patients treated and reducing time to treatment Essential for successful stroke performance improvement Huddle after every TPA eligible patient to discuss what went right and wrong, opportunities for improvement
 TEAM-BASED APPROACH Team approach based on standardized stroke pathways and protocols has proven to be effective in enhancing the number of eligible patients treated and reducing time to treatment Essential for successful stroke performance improvement Huddle after every TPA eligible patient to discuss what went right and wrong, opportunities for improvement")
26
11) PROMPT DATA FEEDBACK Accurately measure and track your door to needle times, IV TPA treatment rates and time intervals Disseminate data and outcomes on every patient on a real time basis Meet frequently to devise strategies to identify and overcome barriers, set targets and monitor progress.
 PROMPT DATA FEEDBACK Accurately measure and track your door to needle times, IV TPA treatment rates and time intervals Disseminate data and outcomes on every patient on a real time basis Meet frequently to devise strategies to identify and overcome barriers, set targets and monitor progress.")
27
FEEDBACK TOOL

28
QUESTIONS?

Similar presentations



















-Score: Probability of Mass Transfusion as Surrogate for Life Threatening Hemorrhage after Multiple Trauma The.>")





 program is provided by the American Heart Association/American Stroke Association. The GWTG->")

>")


