Download presentation
Presentation is loading. Please wait.

1
GAP-D2B An Alliance for Quality

2
GAP-D2B Goal n To achieve a door-to-balloon time of </= 90 minutes for at least 75% of non- transfer primary PCI patients with ST- segment elevation myocardial infarction in all participating hospitals performing primary PCI.

3
What is ACC doing to address this issue? n Assembled the ACC D2B Work Group and (5) subgroups comprised of physician and nurse volunteers and ACC staff n Summarized the evidence and identified the evidence-based strategies n Currently developing the tools and educational materials to support the strategies. n Collaboration with strategically-related organizations is being pursued.
 subgroups comprised of physician and nurse volunteers and ACC staff n Summarized the evidence and identified the evidence-based strategies n Currently developing the tools and educational materials to support the strategies. n Collaboration with strategically-related organizations is being pursued..")
4
Disseminating the “How”: Evidence-based Strategies 1.Pre-hospital ECG to activate the cath lab 2.ED physician activates the cath lab 3.One call activates the cath lab 4.Cath lab team ready in 20-30 minutes 5.Prompt data feedback 6.Senior management commitment 7.Team-based approach

5
Themes n Clear, explicit goal n Administrative support n Clinical champions n Data feedback n Systems approach n Collaborative teams n Culture Circulation 2006;113:1079-85

6
Lowering door-to-balloon…a how-to guide n Patients presenting to the ED with CP are rapidly triaged; an ECG is obtained and immediately shown to an ED physician. Goal: Door to ECG<5 minutes. n ED physician empowered to activate cath lab Interventionalist-does not have to wait until a cardiologist sees the patient.

7
n 24/7 staff and Interventional Cardiologist coverage. Staff expected to arrive no later than 30 minutes after being called. n ED staff trained in the expeditious preparation of the patient. Adequate but limited assessment and preparation performed. Orders standardized wherever possible (IV access, groin shave, Reopro etc.)
.")
8
n Transport to cath lab can occur even before entire cath lab staff or cardiologist is present. When 2 out of 3 are there, “ready call” is made. Cardiologist will briefly assess patient at the door if missed in ED. n Limited injections of non-infarct related arteries are taken with diagnostic catheters, before proceeding directly to the culprit vessel a with an interventional guide. LV gram and other imaging done at the end of case.

9
n Entire process is continually reviewed by a collaborative committee consisting of : ED physician, Cardiologist, Cath lab staff, Administrators, pre-hospital providers, nursing, etc. n A subcommittee reviews charts on all cases with door to device times of greater than 90 minutes, and feedback is provided to those involved. n Transfers from outside hospitals are taken directly to the cath lab, bypassing the ED and CCU.

10
Path Forward n Disseminate the ‘How’ and recruit other hospitals to develop similar programs n Focus on total door-to-balloon time n Focus on associated outcomes n Foster cooperation between PCI and non-PCI hospitals to develop regional MI systems and improve access n Public education to decrease symptom- to-door time and use of 911

11
Challenges/Limitations n Delays are common n Relationship with outcome strong n Disparity is hospital-based n Time of day/day of week important n Specialization important n Pre-hospital ECG rare

12
Relationship between door to balloon time and mortality in NRMI registry Door to balloon time (min)Mortality (%) <903.0 91 – 120 4.2 121 – 150 5.7 >1507.4 McNamara RL et al. J Am Coll Cardiol 2006; 47:2180–2186.

13
Goals National Time Goals n Door to ECG 5 minutes n Door to Cath Lab 30 minutes n Door to Cath Lab device 55 minutes Total =90 minutes Centra Health Goals n Door to ECG 5 minutes n Door to Cath Lab 30 minutes n Door to Cath Lab device 25 minutes Total =60 minutes

14
Total Door-to-Balloon Time Circulation 2005;111:761-7

15
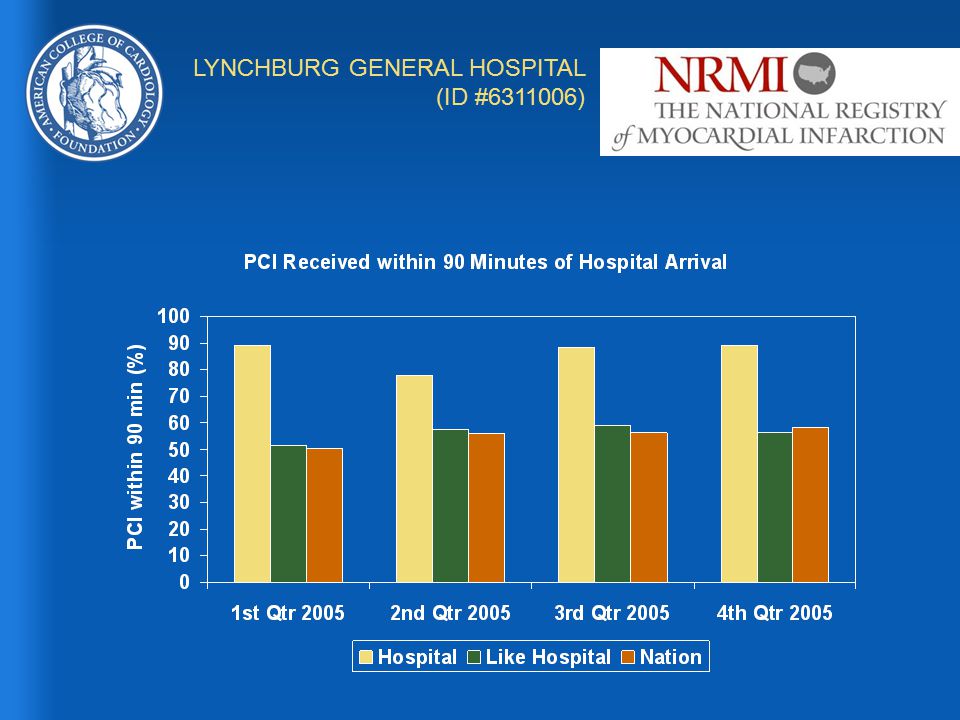
LYNCHBURG GENERAL HOSPITAL (ID #6311006)
")
18
Why pursue D2B at this point? n ACC physicians, staff and our strategic partners are working together on GAP-D2B. n ACC Governor survey indicates that D2B is one of the top areas of interest. n GAP-D2B is consistent with ACC-AHA and SCAI Guidelines. n Opportunity for the ACC BOG to exert its leadership by beginning the launch of a national quality improvement initiative. n Achieving the D2B goal will have a significant positive impact on patient outcomes and mortality.

19
How will ACC execute a solution? n Recruitment begins NOW WITH YOU! n The formal “launch” will occur in November 2006 at AHA. n Over 130 hospitals have already expressed interest in this national collaborative. n GAP-D2B website will enable participants to post data, communicate and evaluate best practices. n ACC Work Group developing tools and materials necessary to successfully reduce door-to-balloon time.

20
What is asked of hospital participants? n Commit to implementing the evidence-based strategies. n Commit to submission of your data. n Allow ACC to use hospital name in D2B promotional materials. n Help contribute to community by sharing stories, successes and obstacles. n Learn from others. n No cost to join.

21
Role of Chapter Executives n Establish a Chapter Quality Council. n Work with Governor to convene D2B team. n Coordinate Chapter level activities and communications. n Assist Governor in recruitment and follow up.

22
Role of Governors n Identify physician champions in your state n Work with physician champions to recruit your primary PCI hospitals to GAP-D2B n Contact your local QIO for collaboration potential n Contact your local MCOs for collaboration potential n Email information to jbyrd@acc.org n WE CHALLENGE EACH GOVERNOR TO RECRUIT AT LEAST 4 HOSPITALS BY NOV. 1

Similar presentations














![[Hospital Name | Presenter name and title | Date of presentation]](/19/5722524/big_thumb.jpg "[Hospital Name | Presenter name and title | Date of presentation]>")


 715-6418>")


 CVN Weekly Interventional Update December 8, 2008 Jeffrey J. Popma and Christopher.>")