Download presentation
Presentation is loading. Please wait.

1
Michael G Mount, DO 5/21/2012

2
Learn the indications, placement and complications of central venous catheters Know the criteria for surgery in Carotid Stenosis and technical basics of Carotid Endarterectomy Understand Abdominal Aortic Aneurysms and the basics of management Know the potential surgical options for correction of peripheral vascular disease Understand relevant anatomy as it relates to vascular surgery

4
Indications for Central Venous Catheterization Monitoring ◦ CVP - central venous pressure, an estimate of Right heart filling pressure, ScvO2 (central venous oxygen saturations) a measure of oxygen return to the heart ◦ PA Catheter - pulmonary artery, catheter allows right ventricle pressure measurements and PAOP (pulmonary artery occlusion pressure) an estimate of left heart filling pressures Access ◦ Dialysis - or plasmapheresis requires large bore double lumen into central vein capable of very high flow ◦ Specific Medications
 a measure of oxygen return to the heart ◦ PA Catheter - pulmonary artery, catheter allows right ventricle pressure measurements and PAOP (pulmonary artery occlusion pressure) an estimate of left heart filling pressures Access ◦ Dialysis - or plasmapheresis requires large bore double lumen into central vein capable of very high flow ◦ Specific Medications")
5
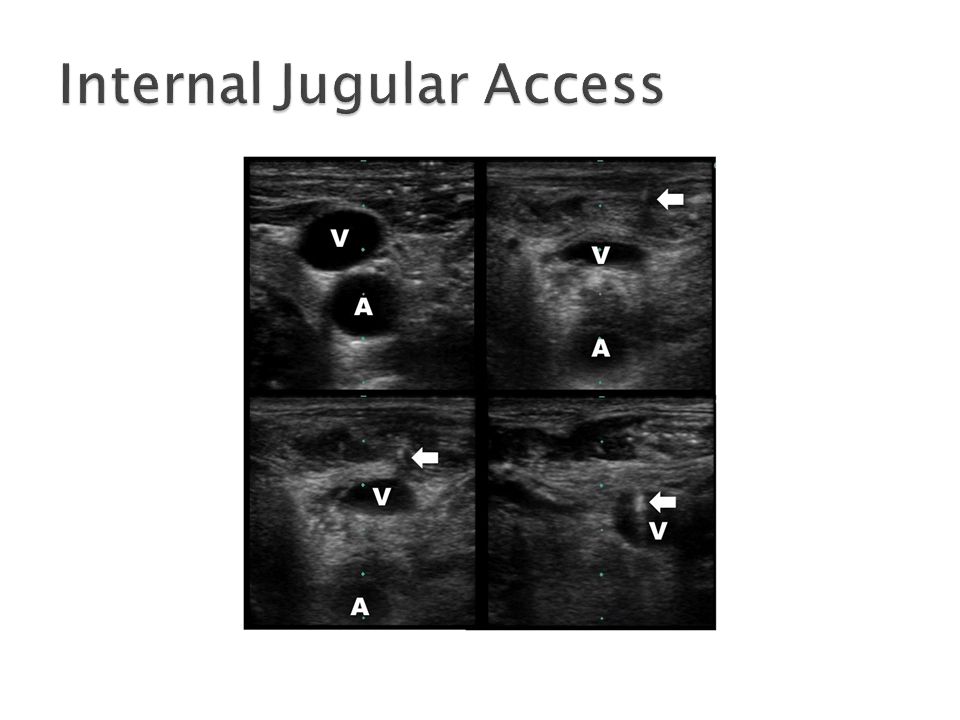
Seldinger Technique ◦ placement of a wire into a vessel followed by placement of catheters over the wire Anatomic Landmarks Ultrasound Locations ◦ Internal Jugular ◦ Subclavian ◦ Femoral

6
Deep to sternocleidomastoid Superficial and lateral to the common carotid artery Joins with subclavian vein to form brachiocephalic (inominate) on left and right
 on left and right")
7
Palpate between sternal and clavicular heads of SCM Enter 30 degrees to skin, aiming towards ipsilateral nipple

9
Landmarks; inferior and lateral to bend of clavicle, aiming towards sternal notch, just deep to clavicle, parallel to ground Higher rates of pneumothorax, lower rates of infection, most comfortable

10
Femoral vein medial and just deep to femoral artery Deep femoral vein and saphenous veins join at deep surface and anteromedial surface respectively Highest rate of infection

11
Potential complications Infection (varies with site, lowest with SC, highest with femoral) lowered by technique, catheter, dressing Pneumothorax – SC higher than IJ, lowered by ultrasound Pseudoaneurysm – sequelae of arterial puncture or inadvertent cannulation Line migration
 lowered by technique, catheter, dressing Pneumothorax – SC higher than IJ, lowered by ultrasound Pseudoaneurysm – sequelae of arterial puncture or inadvertent cannulation Line migration")
13
700,000 CVA per year in United States 75 – 85 % ischemic 20 - 60% related to carotid atherosclerosis 7-12% of patients > 65yo have evidence of atherosclerosis at the carotid bulb Male > Female Vascular Risk Factors Morbidity >> Mortality

14
Stroke TIA (transient ischemic attack) Amarousis Fugax ◦ intermittent blindness; “shade coming down over one eye”, due to transient embolic occlusion of ipsilateral ophthalmic artery Syncope Cervical Bruit
 Amarousis Fugax ◦ intermittent blindness; shade coming down over one eye , due to transient embolic occlusion of ipsilateral ophthalmic artery Syncope Cervical Bruit")
15
Ultrasound – preferred modality 70-99% stenosis; 89% sensitivity, 84% specificity 50-69% stenosis; 36% sensitivity, 91% specificity 0-49% or 100%; 83% sensitivity, 84% specificity

17
TrialIndication Perioperative CVA/Death Risk Reduction P Value NASCETSx: ≥70%5.8%16.5%/2 yr<.001 Sx: 50%-69%6.7%10.1%/5 yr<.05 ECSTSx: 70%-99%7.5%9.6%/3 yr<.01 ACASAsx: ≥60%2.3%5.9%/5 yr.004 ACSTAsx: >60%3.1%5.4%/5 yr<.0001

18
Symptomatic Patient with 70-99%stenosis ◦ CEA and Best medical therapy ◦ Surgeon with perioperative CVA/mortality <6% Recent Completed Stroke ◦ <100% stenosis ◦ Time frame based on CT changes Crescendo or Evolving TIA

19
Asymptomatic Patient with 80%-99% stenosis ◦ CEA and Best medical therapy ◦ Surgeon with perioperative CVA/mortality <3% Asymptomatic Patient 50-79% stenosis ◦ Consider patient specific factors ◦ Operate symptomatic side first, followed by asymptomatic side ◦ If both symptomatic operate on the dominate side first

21
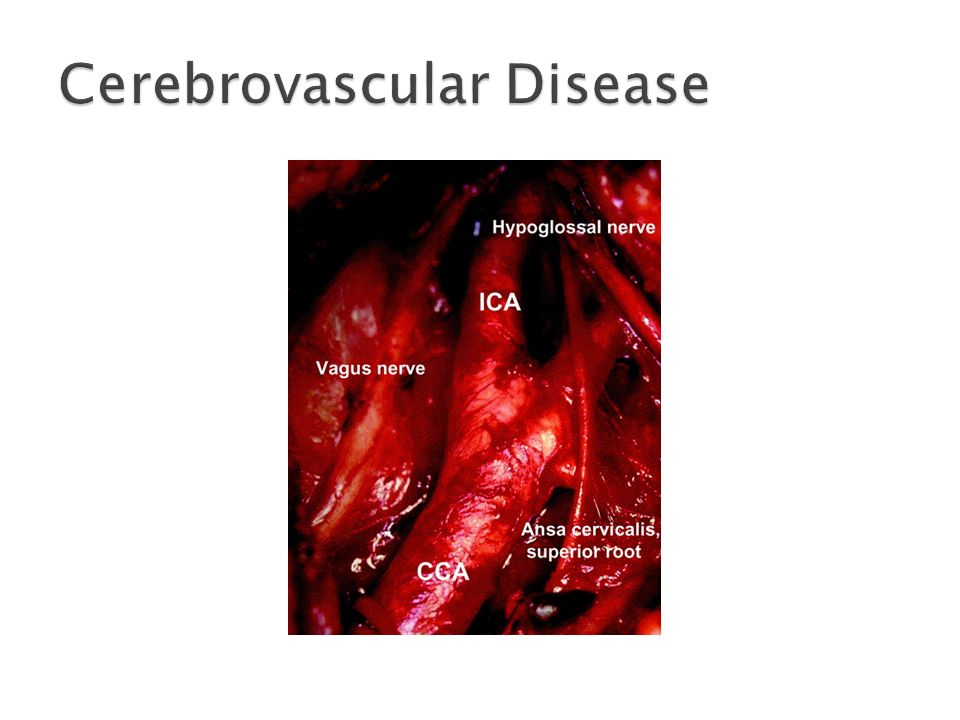
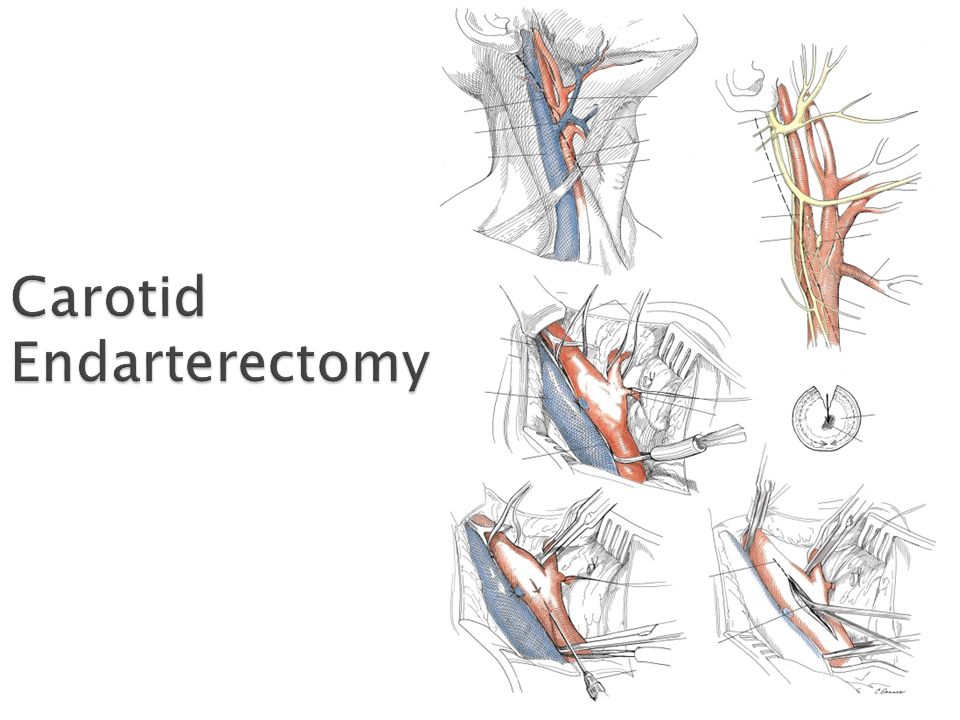
Steps of Carotid Endarterectomy (CEA) SCM incision, open carotid sheath, ligate facial vein, obtain proximal and distal control of CCA, ICA, ECA, Incise and Open carotid, Shunt vs Stump Pressure vs EEG vs Doppler, perform Endarterectomy, close with patch Relevant anatomy Facial Vein crosses over carotid birfurcation to the inernal jugular lying anterolateral to carotid Hypoglossal nerve may cross over both ICA and ECA and need to be retracted; higher up a nerve diving between the two is glossopharyngeal Internal Carotid has no extracranial branches Ansa Cervicalis can be divided if needed for exposure
 SCM incision, open carotid sheath, ligate facial vein, obtain proximal and distal control of CCA, ICA, ECA, Incise and Open carotid, Shunt vs Stump Pressure vs EEG vs Doppler, perform Endarterectomy, close with patch Relevant anatomy Facial Vein crosses over carotid birfurcation to the inernal jugular lying anterolateral to carotid Hypoglossal nerve may cross over both ICA and ECA and need to be retracted; higher up a nerve diving between the two is glossopharyngeal Internal Carotid has no extracranial branches Ansa Cervicalis can be divided if needed for exposure")
22
Mortality 0.5-1% Myocardial Infarction 2-4% ◦ Most common complication Stroke 1-2% Asx patients, 2-6% Sx patients Cranial Nerve Injury ◦ most common hypoglossal tongue deviation towards side of injury (4-17%) ◦ Vagal or recurrent nerve injury from clamping hoarseness (1-15%) Systemic Blood Pressure Instability Bleeding requiring reoperation
 ◦ Vagal or recurrent nerve injury from clamping hoarseness (1-15%) Systemic Blood Pressure Instability Bleeding requiring reoperation")
23
Recurrence Rates and Reoperation Carotid Stenting

25
Dilatation of >50% from normal diameter True vs False Law of Laplace; T=PR/δ Can occur at any artery Usually degenerative

26
Increasing Incidence Screening in certain high risk populations ◦ Ultrasound vs CTA Follow patients with known aneurysms ◦ Follow up every 6 months >4.5 cm, yearly >4 cm +everything else on slide

27
Incidental Screening Embolization Physical Exam Rupture

28
Symptomatic >5.5 cm Men or >5.0 cm Women Inflammatory Aneurysms Open Repair vs EVAR

30
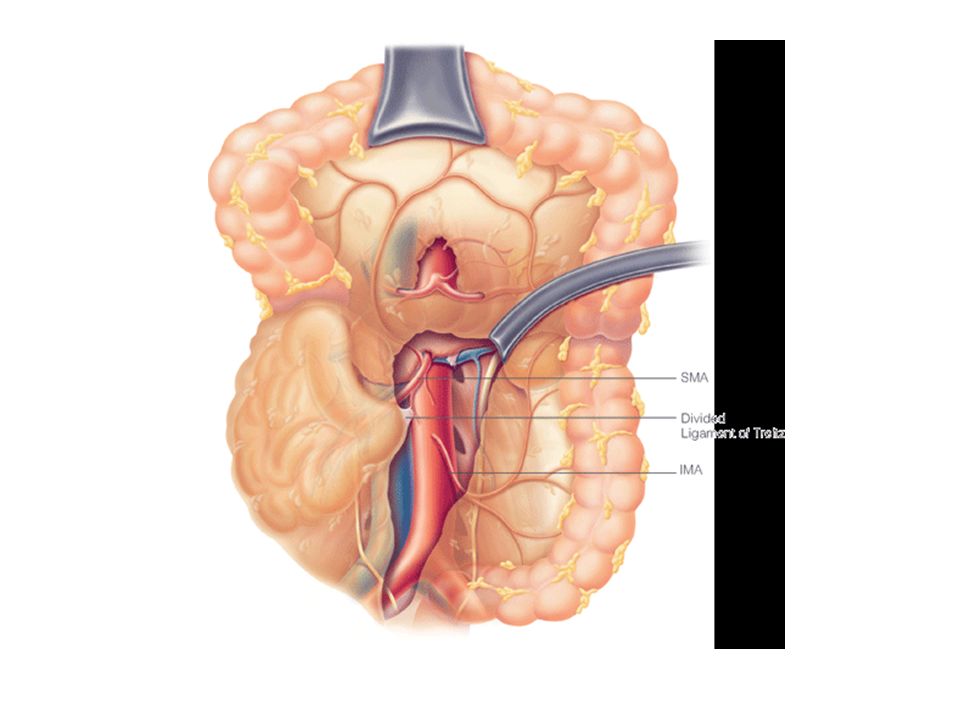
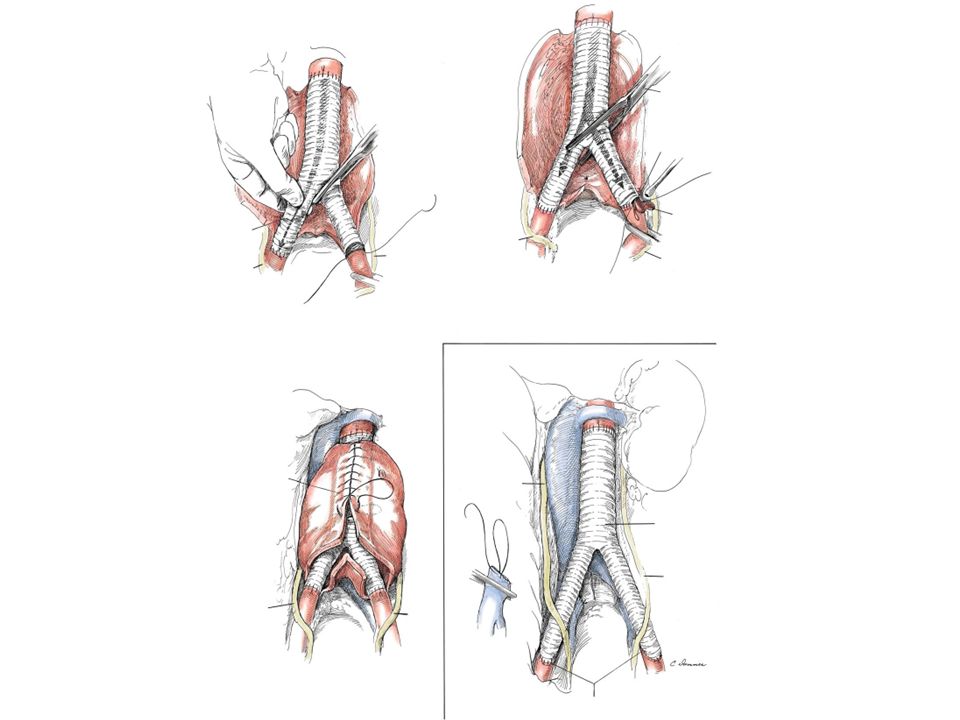
Left Medial Visceral Rotation

31
- Left renal vein crosses aorta collaterals include left gonadal vein, left adrenal vein and left inferior phrenic veins, lumbar veins Ureters cross over common iliacs to reach pelvis

32
Open Repair

39
Impotence – 33% MI – 6.8% Renal Failure – 1-8% Arrhythmia – 9.7% Pseudoaneurysm – 1% Graft Infection – 0.4% Ischemic Colitis

40
Proximal neck – cylinder, 15mm long w diameter 28mm or less Neck angulation (between suprarenal aorta and proximal neck) – 60 degrees Distal landing zone-common iliac less than 18mm in diameter and 2cm in length Quality of access vessels – 7mm or more
 – 60 degrees Distal landing zone-common iliac less than 18mm in diameter and 2cm in length Quality of access vessels – 7mm or more")
41
EVAR

42
Indications Early postoperative survival benefit Differences in Complications Need for reimaging and reoperation Endoleak

45
++

46
=

47
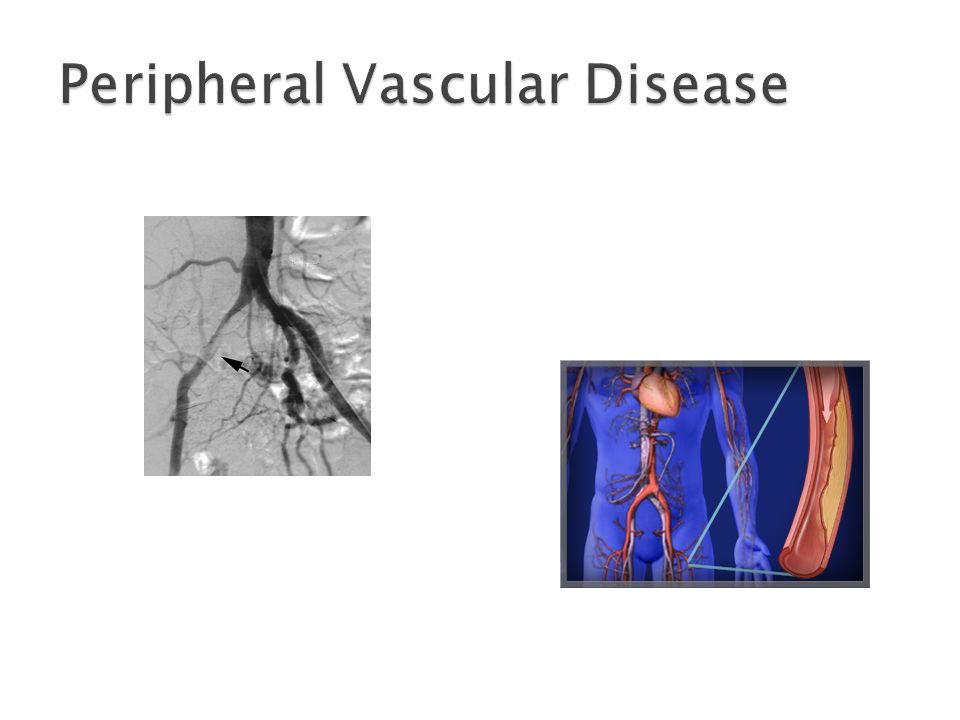
Atherosclerosis Lower Extremities Signs & Symptoms ◦ Claudication ◦ Rest Pain ◦ Poor Wound Healing ◦ Ulcers ◦ Dependent Rubor ◦ Hair Loss ◦ Dry Gangrene

48
<0.9 Claudication <0.5 Rest Pain <0.4 Ulceration <0.3 Gangrene

49
Ratio of Systolic Blood Pressure in the lower extremity to the upper extremity Normal is greater than 1.0. ◦ Symptoms correlate with decreasing ABI Can be inaccurate in diabetic patients due to medial calcinosis (Monckeburg) ◦ use TBI, Plethysmography Depends on degree of chronicity and collateralization Symptoms are typically one level below the area of narrowing: ◦ aortoiliac disease (AIOD) thigh and buttock claudication, impotence (Leriche Syndrome) ◦ femoral disease calf claudication (most common lesion within Hunter’s canal, also called adductor canal) ◦ tibioperoneal disease foot claudication
 ◦ use TBI, Plethysmography Depends on degree of chronicity and collateralization Symptoms are typically one level below the area of narrowing: ◦ aortoiliac disease (AIOD) thigh and buttock claudication, impotence (Leriche Syndrome) ◦ femoral disease calf claudication (most common lesion within Hunter’s canal, also called adductor canal) ◦ tibioperoneal disease foot claudication.")
50
Smoking Cessation Exercise Statins ASA Cilostazol

51
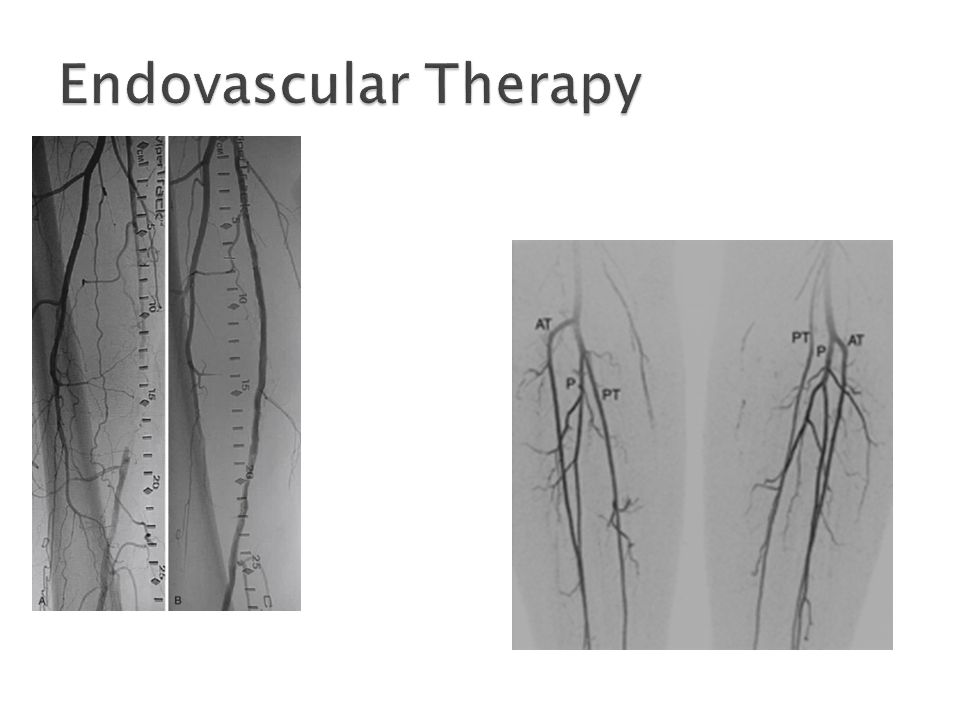
Indications Percutaneous Balloon Angioplasty Stenting Bypass

53
Based on Anatomic distribution of disease Basic Principles of Vascular Surgery Graft Choice ◦ PTFE (synthetic), Reversed Saphenous Vein, In-Situ Saphenous Vein
, Reversed Saphenous Vein, In-Situ Saphenous Vein")
55
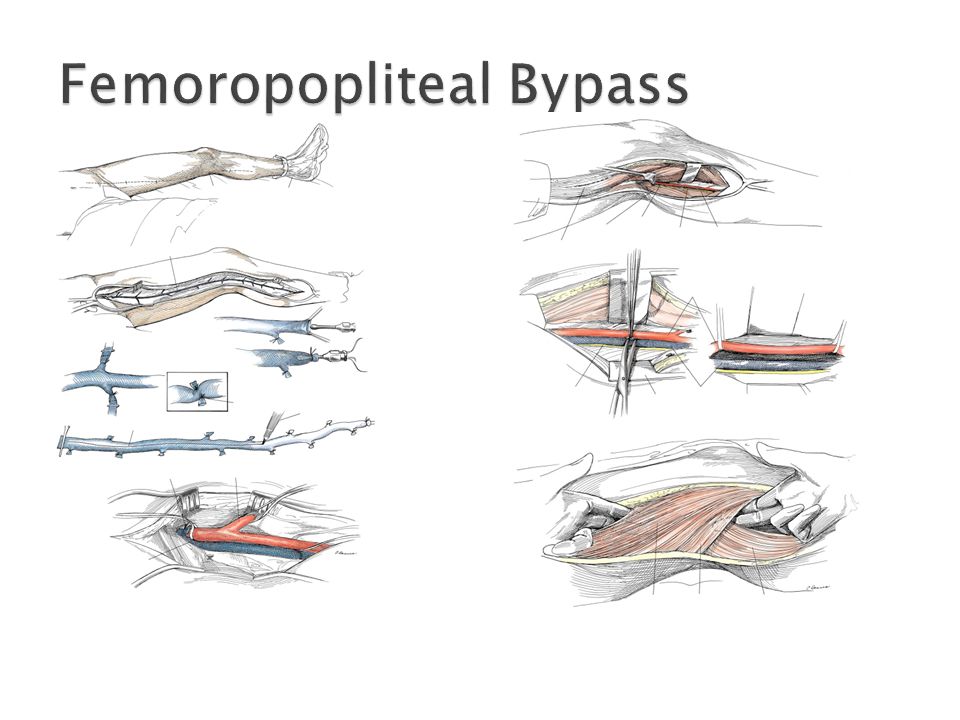
Saphenous vein is mapped preoperatively with ultrasound, exposed along its length and taken off saphenofemoral junction. Tributaries are ligated. 3mm distended diameter is minimum required. Line drawn down vein to maintain orientation and prevent twisting. Large single or multiple separate incisions can be made. Lymphatic tissue medial to vein is ligated to prevent leak postop Incision posteromedial to knee (immediately posterior to tibia if below), above or below based on area of stenosis is made for access to popliteal vessels Posterior fascial compartment is opened and gastrocnemius and soleus are retracted posteriorly while the adductor muscles are retracted anteriorly Artery is located laterally to popliteal vein and tibial nerve Tunnel is made deep to the sartorius and adductor muscles
, above or below based on area of stenosis is made for access to popliteal vessels Posterior fascial compartment is opened and gastrocnemius and soleus are retracted posteriorly while the adductor muscles are retracted anteriorly Artery is located laterally to popliteal vein and tibial nerve Tunnel is made deep to the sartorius and adductor muscles.")
56
- Gastrocnemius medial head may need to be incised to prevent compression of the graft - Anastomosis is made with running prolene suture

57
Outcomes 5 year patency approaches 90% with saphenous vein above the knee Lower patency for PTFE Lower patency for Limb Salvage May require Secondary Interventions for patency Follow with duplex ultrasound

58
Overall Morbidity ~25% MI – most common Mortality ~2-3% Wound infection Amputation ◦ End stage vascular surgery

Similar presentations
























 LECT7 ALI B ALHAILIY.>")
 Aneurysms Thrombangitis obliterans Inflammatory arteritis Aetiology.>")


