Download presentation
Presentation is loading. Please wait.

1
Vertebral PTA: Indications and Technique Patrick L. Whitlow, MD Director, Interventional Cardiology The Cleveland Clinic Foundation Patrick L. Whitlow, MD Director, Interventional Cardiology The Cleveland Clinic Foundation I have NO relationships related to this presentation. Off label use of products will be discussed in this presentation.

2
Vertebral Artery Stenosis/ Occlusion: Symptoms 50% present with stroke as 1st symptom Embolic: sudden maximum onset, blurred vision, or homonymous hemianopsia- usually originate from VA origin Vertebrobasilar TIA’s - 22-35% stroke by 5yrs, and mortality with CVA 20-30%

3
Vertebral Artery Stenosis/ Occlusion: Symptoms Hemodynamic: tandem/severe lesions Multiple Symptoms: vertigo,nausea, visual dysfunction; perioral paresthesia; ataxia; dysarthria; syncope; headache; nystagmus; facial palsy,numbness Thrombotic: prolonged, fluctuating course to maximum neurologic deficit or coma

4
Vertebral Artery Stenosis/ Occlusion: Symptoms Symptoms:Hemodynamic Thrombotic Predominantly occur in Patients with Multi-Vessel Disease because of Redundant Blood Supply Emboli may occur with isolated disease

5
Vertebral Artery Stenosis/ Occlusion: Treatment Symptomatic angiography > revascularization Asymptomatic majority get medical rx Consider revascularization if high risk for CVA (Remember 50% of these have no warning TIA’s) > 70% stenosis, esp. if worsening and dominant or single vertebral Posterior hypoperfusion or decreased reserve

6
Vertebral Artery Stenosis/ Occlusion: Treatment Traditional: Avoid Hypotension;use Antiplatelet or Anticoagulant; carotid duplex; IC Doppler Vertebral Origin Lesions difficult to quantify w/o angiography, and need to assess collaterals >Consider surgery for V 1 disease(unusual) >Consider percutaneous intervention
 >Consider percutaneous intervention")
7
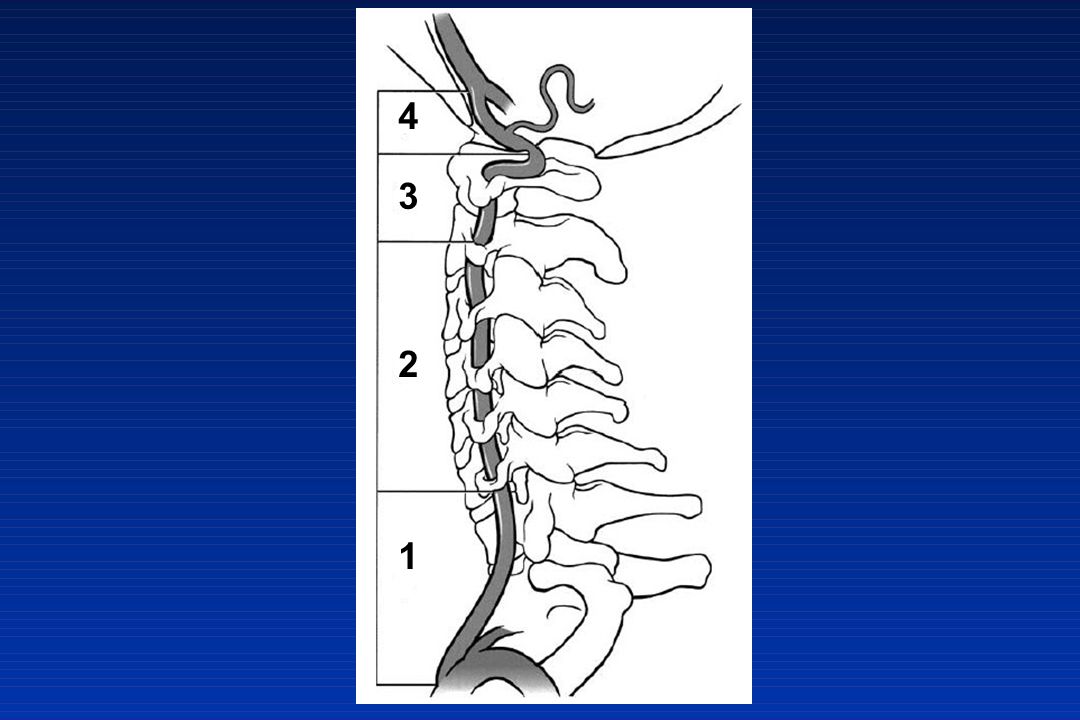
Background Limited data exists on percutaneous treatment of symptomatic vertebral artery disease Surgical treatment for symptomatic vertebral artery disease has significant morbidity and is limited to V1 segment

8
4 3 2 1
9
Vertebral Artery Disease: Surgery for V 1 Segment Carotid-Vertebral Transposition or Endarterectomy Mortality > 4% Morbidity 10-20%

10
Vertebral Surgery Complications of V1 Surgery: Transient ischemic attack2.2% Thrombosis8.7% Koskas, Ann Vasc Surg 9:515-524 Recurrent laryngeal nerve palsy2% Horner’s syndrome15% Lymphocele4% Chylothorax0.5% Thrombosis1% Beurger, Long Term Results in Vascular Surgery 1993:69-79

11
Vertebral Artery Stenosis / Occlusion: Treatment No randomized studies Meds vs Surgery and No Trials Intervention vs either Meds or Surgery Symptoms are frequently vague: may need flow study to determine significance Neuro Consult very helpful

12
Vertebral Artery Angiography Baseline Angiography: 30-45% LAO Arch Angio with 4 vessel study to define collateral support of the posterior circulation( non-selective) For Selective vertebral: JR4,Berenstein, MP A-P ; 20-30 o contralateral oblique;cranial 20º
 For Selective vertebral: JR4,Berenstein, MP A-P ; o contralateral oblique;cranial 20º")
13
Vertebral Artery Stenting Pretreat with ASA, Clopidogrel > 3 days Access Femoral Artery, or Radial / Brachial JR4, IMA, MP, H 1, 6Fr Guide or /Ansel Sheath Heparin 50-70 units/kg: ACT 240-300 seconds Rarely consider IIb/IIIa blocker (IC Hemorrhage) Consider Embolic Protection: Tortuosity, landing zone, branches, retrieval
 Consider Embolic Protection: Tortuosity, landing zone, branches, retrieval")
14
Vertebral Artery Stenting Consider subclavian “Buddy-Wire” Roadmap; cross with 0.014” wire or EPD - stay out of Branches Consider predilation with coronary balloon vs direct stent Artery size 2.7 - 5.5mm, mean 4.5mm; lesion length typically 5-10mm - so use coronary stents

15
Vertebral Artery Stenting If ostial, use balloon expandable stent for precise placement ~2mm into subclavian origin High restenosis rates in some series (up to 43%) - ?ostial coverage, ?recoil Consider DES; stents with radial force
 - ostial coverage, recoil Consider DES; stents with radial force")
16
Vertebral Artery Stenting Precise Deployment, slow inflation to ~8atm Pull balloon back high pressure (12-14atm) to minimize risk distal dissection, Flare edge Nitro and angio to assess size, edges
 to minimize risk distal dissection, Flare edge Nitro and angio to assess size, edges")
17
Optimize stent size with post-dilation Frequent Neuro status checks Final angios to asses for embolization, EPD damage,wire trauma,kinking Esp with EPD, push/pull guide into stent for retrieval Vertebral Artery Stenting

18
Usual post Sheath care Usual ASA, Plavix Independent Neuro Exam Monitor overnight Usual Risk Factor Control

19
Vertebral Artery Stenting Results 94-100% Technical Success Complications: Dissection, spasm, embolism, CVA, TIA, thrombosis, IC bleeding - All rare Usual 1-2% sheath related events

20
Vertebral Artery Stenting Follow-Up Work with a Neurologist Non-invasive assessment not reliable Consider Re-Angio 4-6 months Restenosis 10-43% - usually asymptomatic Randomized Trials, long term follow-up are needed!! ?Role of EPD, DES, surgery

21
Severe Ostial Vertebral Stenosis Post-procedure Pre-procedure

Similar presentations









, PhD(Lond.), FEBVS Professor of Vascular Surgery Chairman, Dept. of Vascular Surgery,>")












