Download presentation
Presentation is loading. Please wait.

1
Carotid artery stenting in the patients with high surgical risk : a single-center experience with 326 patients Jiang Xiong-jing, Teng Si-yong, Ji wei, Yang Yue-jin, Xu Bo, Gao Run-lin Dept. of Cardiology, Fuwai Hospital Dept. of Cardiology, Fuwai Hospital Beijing 100037,China

2
Background Endovascular techniques have recently been evolving. Carotid artery stenting (CAS) is challenging CEA for the best treatment in high surgical risk patients with extracranial carotid arterial disease. However, significant controversies still persist.
 is challenging CEA for the best treatment in high surgical risk patients with extracranial carotid arterial disease. However, significant controversies still persist..")
3
RCTs EV3 + SPACE SAPPHIRE Effectiveness of Management Strategies for Carotid Artery Stenosis CAS Vs CEA

4
Objectives To evaluate the safety of CAS in the patients with high surgical risk

5
Methods A retrospective study of consecutive carotid artery stenting (CAS) cases in Fuwai hospital, From Jan. 2003 to Dec. 2008 Significant carotid artery disease was defined as luminal diameter reduction of >60%(symptomatic) or >80%(asymptomatic) FDA-approved indications for CAS Patients were excluded if 1) they had severe renal impairment 2) an ipsilateral cerebrovascular event within the prior 1 months 3)major neurological deficit. 4) severe diffuse atherosclerosis of the common carotid artery, chronic total occlusions, and long preocclusive lesions.5) unstable medical situation. All patients gave written informed consent.
 or >80%(asymptomatic) FDA-approved indications for CAS Patients were excluded if 1) they had severe renal impairment 2) an ipsilateral cerebrovascular event within the prior 1 months 3)major neurological deficit. 4) severe diffuse atherosclerosis of the common carotid artery, chronic total occlusions, and long preocclusive lesions.5) unstable medical situation. All patients gave written informed consent..")
6
End-Point Definition The primary end point : the combined incidence of death and stroke from time of CAS to 30 days after cardiac surgery. Fatal stroke : death attributed to an ischemic or hemorrhagic stroke. major Strokes : a modified Rankin score of >3 at 30 days after onset of symptoms. A minor stroke : a Rankin score of 3 or less that resolved completely within 30 days. Transient ischemic attack and amaurosis fugax : the symptoms disappeared within 24 hours.

7
Secondary end points MI and combined death, stroke, and MI from time of CAS to 30 days after cardiac surgery. The diagnosis of MI was based on the ECG and an elevated creatine kinase with an elevated level of MB isoenzyme. Cardiocerebrovascular mortality was reported separately and was defined as death related to a cardiac or neurological event.

8
Routine procedures aspirin 100 mg + clopidogrel 75 mg daily was administered at least 2 days before the procedure and maintained at least 30 days Antihypertensive medication and B- blockers was tapered 1 day before the procedure to decrease baroreceptor stimulation–related bradycardia and hypotension.

9
Routine procedure All procedures were performed via femoral access according to the standard technique. A distal/proximal cerebral protection device was used in every procedure, unless the lesion was considered not to allow using the device. Procedural success : stent deployment with a residual diameter stenosis<30%. All patients were evaluated clinically before the procedure, during the procedure, and immediately afterward.

10
Special consideration In Pts scheduled for OHS In Pts scheduled for OHS > 1 week after CAS, Aspirin and clopidogrel were discontinued 3-5 days before surgery, only LMW heparin 100-120u/kg, Q12 h, was administered until OHS. In Pts scheduled for OHS within 1 week after CAS, LMW heparin 100-120u/kg, Q12 h, with or without aspirin 100 mg daily was administered at least 2 days before the procedure and maintained until OHS

11
Subsequent Cardiac Surgery Cardiac surgery was performed after CAS or with simultaneous carotid stenting, based on clinical situation and consensus decision. Aspirin and clopidogrel was re-administered 1 day after OHS and overlaped with LMW heparin 3 days after OHS. Our institution is a large cardiovascular center. More than 6,000 adult cardiovascular surgery procedures and 8,000 percutaneous cardiovascular interventions were performed in 2009.

12
Baseline Clinical Patient Characteristics (n=326 Patients) Age, mean±SD, y69.2±7.2 Women(%)78 (23.9) Hypertension (%)228 (69.9) Diabetes mellitus (%)91 (27.9) dyslipidemia (%)189(58.0) Smoking (%)196 (60.1) History of ischaemic stroke (%)56(17.2%) Coronary heart disease (%)292(89.6) Valvular heart disease (%)20 (6.1) Congestive heart failure (%)39 (12.0) Previous CEA (%)6 (1.8) Pulmonary disease (%)25 (7.7) Renal failure (creatinine 133–264 µmol/L) (%)38 (11.7) Bilateral carotid stenosis >60% (%)40 (12.3) unilateral carotid occlusion (%)12 (3.7)
 Age, mean±SD, y69.2±7.2 Women(%)78 (23.9) Hypertension (%)228 (69.9) Diabetes mellitus (%)91 (27.9) dyslipidemia (%)189(58.0) Smoking (%)196 (60.1) History of ischaemic stroke (%)56(17.2%) Coronary heart disease (%)292(89.6) Valvular heart disease (%)20 (6.1) Congestive heart failure (%)39 (12.0) Previous CEA (%)6 (1.8) Pulmonary disease (%)25 (7.7) Renal failure (creatinine 133–264 µmol/L) (%)38 (11.7) Bilateral carotid stenosis >60% (%)40 (12.3) unilateral carotid occlusion (%)12 (3.7)")
13
Angiographic and Stenting Results Unilateral stenting 296 ( 91.8% ) Bilateral stenting 30 ( 9.2% ) Ostial and proximal lesions of CCA 11 ( 3.4% ) Middle and distal lesions of CCA 29 (8.9%) Ostial and proximal lesions of ICA 286(87.7%) Lesion MLD(mm) 0.9±1.1 Lesion stenosis(%) 84.1±8.5 Nitinol self-expandable stents 318 (97.5%) Balloon expandable stents 8 ( 2.5% ) Stent nominal diameter (mm) 8.0±0.5 Length of stent (mm) 35.0±4.6 Balloon nominal diameter(mm) 5.1±0.5 Maximal inflation(atm) 10.3± 2.5 Residual stenosis(%) 8.5±2.8 Distal embolic protection devices 321 (98.5%)
 Bilateral stenting 30 ( 9.2% ) Ostial and proximal lesions of CCA 11 ( 3.4% ) Middle and distal lesions of CCA 29 (8.9%) Ostial and proximal lesions of ICA 286(87.7%) Lesion MLD(mm) 0.9±1.1 Lesion stenosis(%) 84.1±8.5 Nitinol self-expandable stents 318 (97.5%) Balloon expandable stents 8 ( 2.5% ) Stent nominal diameter (mm) 8.0±0.5 Length of stent (mm) 35.0±4.6 Balloon nominal diameter(mm) 5.1±0.5 Maximal inflation(atm) 10.3± 2.5 Residual stenosis(%) 8.5±2.8 Distal embolic protection devices 321 (98.5%)")
14
Other procedures combined with CAS Other proceduresN(%) Cardiac Surgery145(44.5%) Coronary artery stenting78(23.9%) Renal artery stenting65 (19.9) Subclavian artery stenting62 (19.0) Vertebal artery stenting23(7.1) Illiac artery stenting10 (6.1 )
 Cardiac Surgery145(44.5%) Coronary artery stenting78(23.9%) Renal artery stenting65 (19.9) Subclavian artery stenting62 (19.0) Vertebal artery stenting23(7.1) Illiac artery stenting10 (6.1 )")
15
Cardiac Surgery procedures Cardiac surgery : 128 (88.3%) CABG,; 12 (8.3%) CABG + CVR, and 5 (3.4%) CVR. The mean time to cardiac surgery after CAS was 14 days, with a range of 0 day to 3 months. 29 pts (20.0%) underwent simultaneous carotid stenting before CABG, 58 pts (40.0%) underwent CABG within 14 days after CAS, 30(20.7%) after 14 to 30 days, and 28 (19.3%) after 30 days.
 underwent simultaneous carotid stenting before CABG, 58 pts (40.0%) underwent CABG within 14 days after CAS, 30(20.7%) after 14 to 30 days, and 28 (19.3%) after 30 days..")
16
Periprocedural Outcome and 30-Day Follow-Up Event PCI Pts (n=78)Cardiac Surgery Pts (n=145)Others (n=103)Total (n=326) All deaths0 (0.0)2 (1.4)1 (1.0)3 (0.9) Cardiac deaths0 (0.0)1 (0.7)0 (0.0)1 (0.3) Neurological deaths01(0.7)1(1.0)2 (0.6) other deaths00(0.0) All strokes2 (2.6)4 (2.8)2 (2.0)8 (2.45) Major ipsilateral nonfatal1 (1.3)2 (1.4)1 (1.0)4 (1.2) Major contralateral nonfatal (0.0)1 (0.7)0 (0.0)1 (0.3) Minor strokes1 (1.3)1 (0.7)1 (1.0)3 (0.9) Transient ischemic attacks2 (2.6)2 (1.4)2 (1.9)6 (1.8) Nonfatal MIs0 (0.0)2 (1.4)0 (0.0)2 (0.6) All deaths and major strokes1 (1.3)5 (3.4)2 (1.9)8 (2.45) All deaths, major strokes, and MIs 1 (1.3)7 (4.8)2 (1.9)10 (3.1) Values are n (%).
Cardiac Surgery Pts (n=145)Others (n=103)Total (n=326) All deaths0 (0.0)2 (1.4)1 (1.0)3 (0.9) Cardiac deaths0 (0.0)1 (0.7)0 (0.0)1 (0.3) Neurological deaths01(0.7)1(1.0)2 (0.6) other deaths00(0.0) All strokes2 (2.6)4 (2.8)2 (2.0)8 (2.45) Major ipsilateral nonfatal1 (1.3)2 (1.4)1 (1.0)4 (1.2) Major contralateral nonfatal (0.0)1 (0.7)0 (0.0)1 (0.3) Minor strokes1 (1.3)1 (0.7)1 (1.0)3 (0.9) Transient ischemic attacks2 (2.6)2 (1.4)2 (1.9)6 (1.8) Nonfatal MIs0 (0.0)2 (1.4)0 (0.0)2 (0.6) All deaths and major strokes1 (1.3)5 (3.4)2 (1.9)8 (2.45) All deaths, major strokes, and MIs 1 (1.3)7 (4.8)2 (1.9)10 (3.1) Values are n (%).")
17
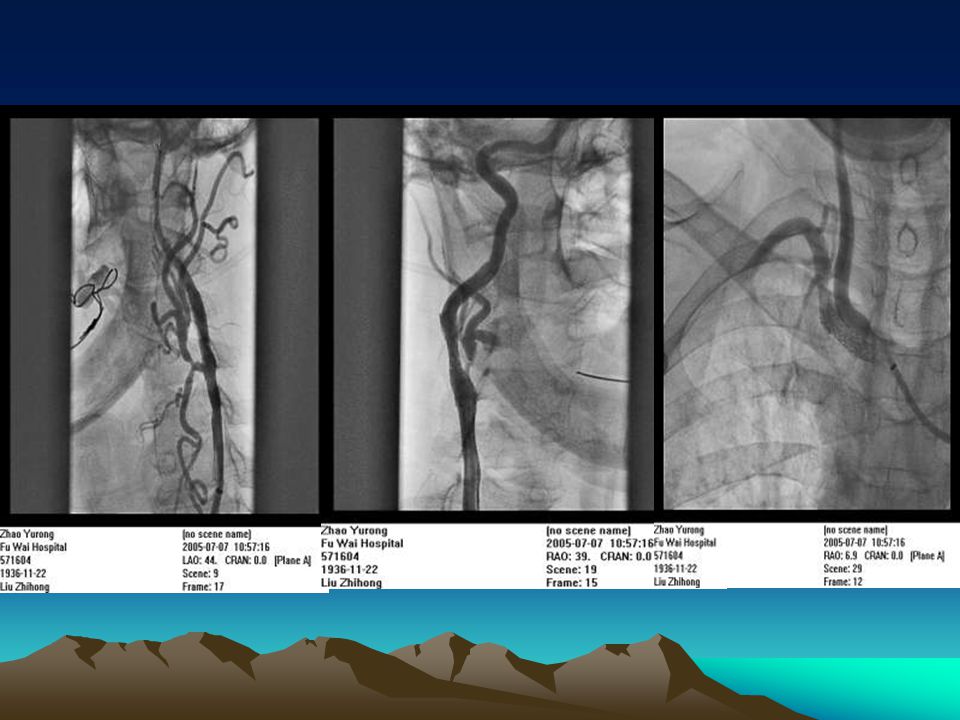
Coronary angiogram findings: triple vessels disease carotid angiogram findings: bilateral ICA stenoses 90% + right subcl stenoses 80% Strategy: Staged carotid stenting(right) + CABG
 + CABG")
19
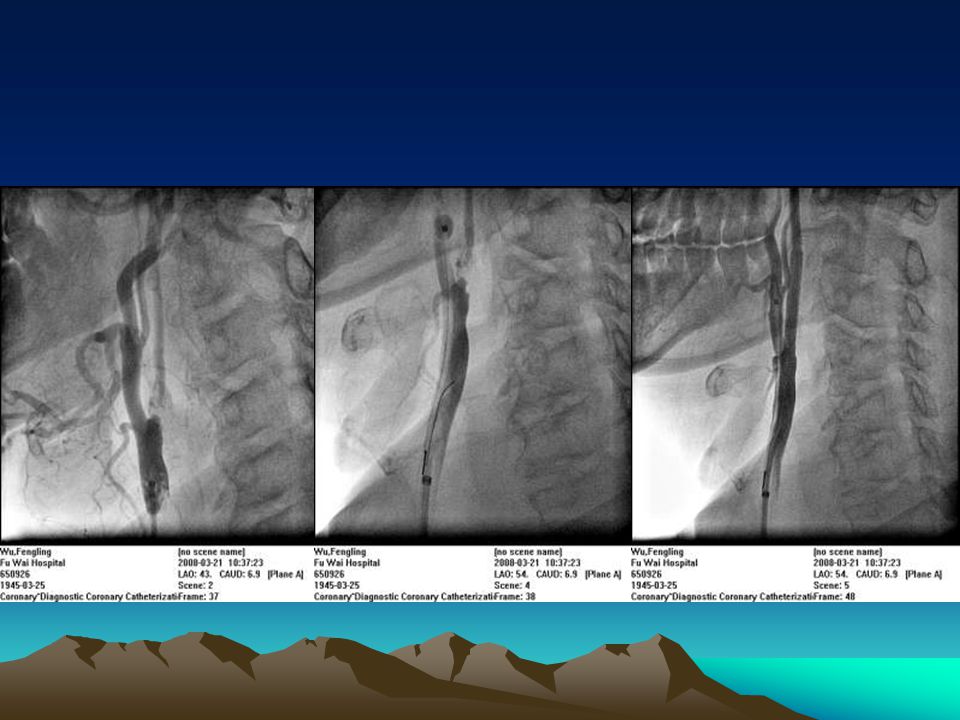
Mar. 7 th, 2008 Coronary angiogram findings: triple vessels disease Mar. 19 th, 2008 carotid angiogram findings: right ICA stenoses 99% Strategy: Staged carotid stenting(right) + CABG
 + CABG.")
21
Conclusions CAS is a technically feasible and a safe alternative to treat extracranial carotid stenosis in this high surgical risk population, comparable to reported results from CEA. The subgroup indicated it is safe and effective carotid artery stenting before open heart surgery in ischemic stroke protection. The results are well comparable with that of staged carotid endarterectomy before open heart surgery reported previously. However, it should be investigated further.

Similar presentations















>")




