Download presentation
Presentation is loading. Please wait.

1
ACUTE LUNG INJURY Acute lung injury is a spectrum of pulmonary lesions (endothelial and epithelial), which can be initiated by numerous conditions. Clinically, acute lung injury manifests as (1) the acute onset of dyspnea, (2) decreased arterial oxygen pressure (hypoxemia), (3) development of bilateral pulmonary infiltrates on radiographs, (4) absence of clinical evidence of primary left-sided heart failure. acute lung injury ---- damage to the alveolar capillary membrane rather than left-sided heart failure noncardiogenic pulmonary edema. Acute lung injury can progress to the more severe acute respiratory distress syndrome,
 the acute onset of dyspnea, (2) decreased arterial oxygen pressure (hypoxemia), (3) development of bilateral pulmonary infiltrates on radiographs, (4) absence of clinical evidence of primary left-sided heart failure. acute lung injury ---- damage to the alveolar capillary membrane rather than left-sided heart failure noncardiogenic pulmonary edema. Acute lung injury can progress to the more severe acute respiratory distress syndrome,.")
2
Acute Respiratory Distress Syndrome (ARDS) ARDS is non cardiogenic pulmonary edema due to diffuse alveolar capillary and epithelial damage. Rapid onset of severe life-threatening respiratory insufficiency Cyanosis Severe arterial hypoxemia Extrapulmonary multisystem organ failure Diffuse alveolar damage (DAD)
.")
3
Pathogenesis Diffuse damage to the alveolar capillary walls Capillary endothelium Increased vascular permeability alveolar flooding Loss of diffusion capacity Widespread surfactant abnormalities

4
The normal alveolus (left) compared with the injured alveolus in the early phase of acute lung injury and the acute respiratory distress syndrome
 compared with the injured alveolus in the early phase of acute lung injury and the acute respiratory distress syndrome")
5
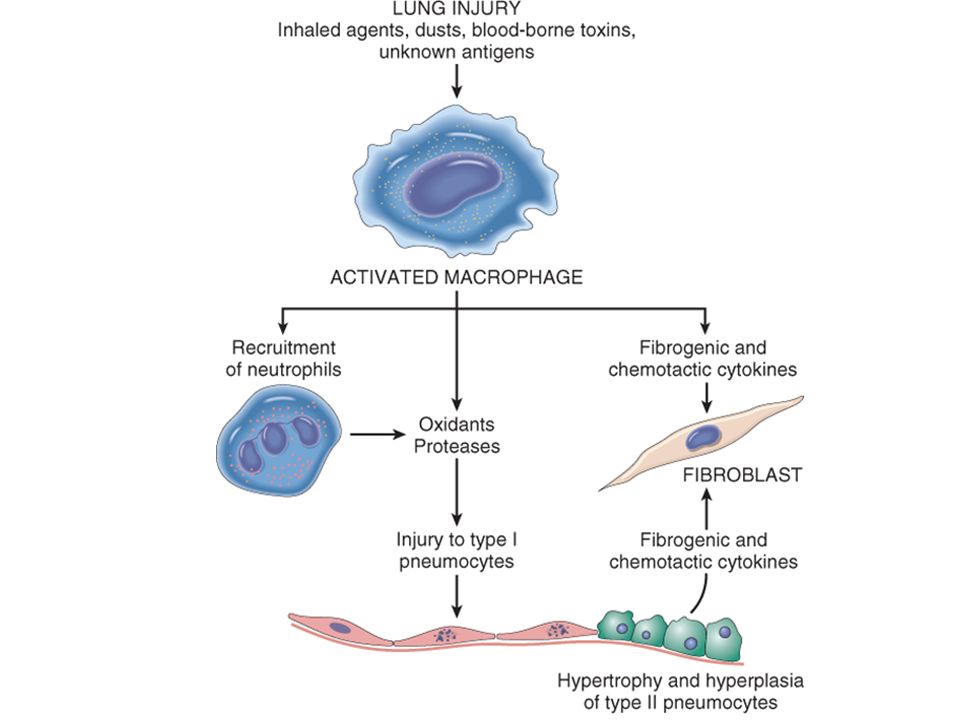
Neutrophils are an important role in the pathogenesis of ARDS. Alveolar macrophages and other cells releases cytokines. Cytokines are chemotactic to neurtophils. Capillary damage causes leakage of protein rich exudate forming hylaine membrane. Neutrophils damage type 1 and 2 pneumocytes. Later repair by type 2 pneumocytesand progressive interstitial fibrosis.

6
Clinical Disorders Associated with the Development of Acute Respiratory Distress Syndrome Direct Lung Injury Common-Pneumonia Aspiration of gastric contents Uncommon- Fat embolism Near drowning Pulmonary contusion Inhalational injury Indirect Lung Injury Common-Sepsis, DIC Severe trauma with shock Uncommon- Cardiopulmonary bypass Acute pancreatitis Uremia Drug overdose

7
Morphology Heavy, firm, red, and boggy Congestion, interstitial and intra-alveolar edema, inflammation, and fibrin deposition Hyaline membrane.

9
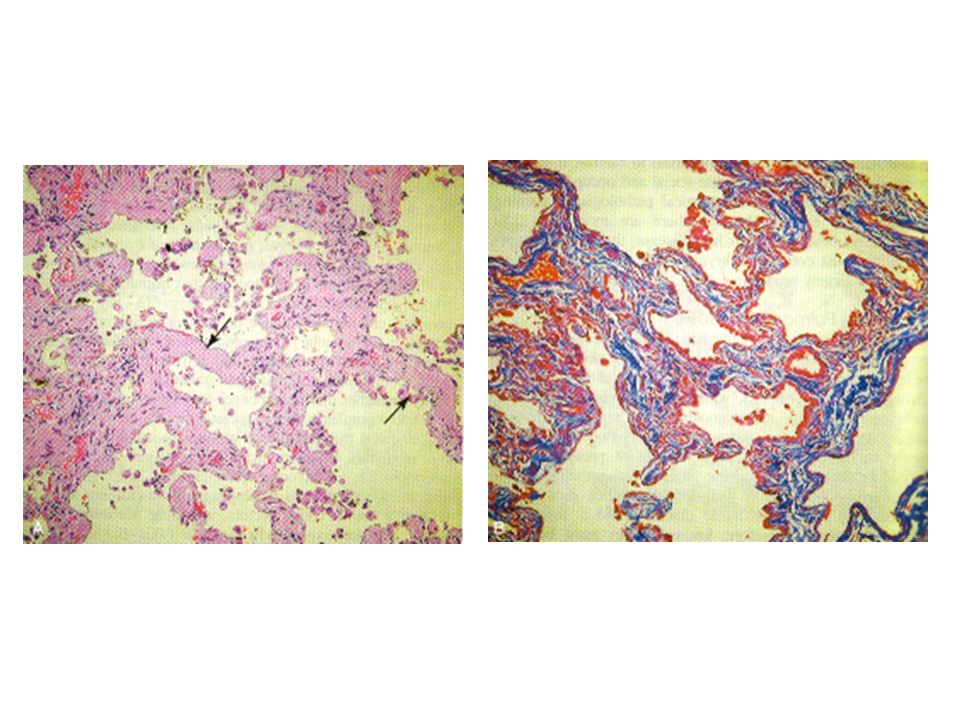
1. Diffuse alveolar damage in acute lung injury and ARDS. Some alveoli are collapsed; others are distended. Many are lined by bright pink hyaline membranes (arrow). 2. In the healing stage there is resorption of hyaline membranes with thickened alveolar septa containing inflammatory cells, fibroblasts, and collagen. Numerous atypical type II pneumocytes are seen at this stage (arrows), associated with regeneration and repair
. 2. In the healing stage there is resorption of hyaline membranes with thickened alveolar septa containing inflammatory cells, fibroblasts, and collagen. Numerous atypical type II pneumocytes are seen at this stage (arrows), associated with regeneration and repair.")
10
Approximately 85% of patients develop the clinical syndrome of acute lung injury or ARDS within 72 hours of the initiating insult. Dyspnea/Tachypnea, late inspiratory crackles poor prognosis in Advanced age, bacteremia (sepsis), multisystem (especially cardiac, renal, or hepatic) failure.
, multisystem (especially cardiac, renal, or hepatic) failure..")
11
Laboratory findings and treatment Severs hypoxemia not responding oxygen Pulmonary arterial wedge pressure <16 mmHg Increased A-a gradient Respiratory acidosis Chest x ray-Bilateral interstitial infiltrates. Treatment- treat underlying cause, Nitric oxide inhalation, mechanical ventilation

12
Diffuse interstitial (restrictive) lung diseases Are a heterogeneous group of disorders characterized predominantly by diffuse and usually chronic involvement of the pulmonary connective tissue, principally the most peripheral and delicate interstitium in the alveolar walls. The pulmonary interstitium basement membrane of the endothelial and epithelial cells (fused in the thinnest portions), collagen fibers, elastic tissue, fibroblasts, a few mast cells, and occasional mononuclear cells.
, collagen fibers, elastic tissue, fibroblasts, a few mast cells, and occasional mononuclear cells..")
13
Spirometry Total lung capacity(TLC)total amount of air in a fully expanded lung. Residual volume(RV)amount of air remain after maximal expiration. Tidal volume(TV)-Volume of air enters or leaves the lung in a quiet respiration. Force vital capacity(FVC)-Amount of air expelled after maximal inspiration. Normal 5 L. Force expiratory volume(FEV1)-Amount of air expelled after from the lung after maximal inspiration after 1 min. Normal 4 L. Ration-FEV1/FVC=4/5=80%.
amount of air remain after maximal expiration. Tidal volume(TV)-Volume of air enters or leaves the lung in a quiet respiration. Force vital capacity(FVC)-Amount of air expelled after maximal inspiration. Normal 5 L. Force expiratory volume(FEV1)-Amount of air expelled after from the lung after maximal inspiration after 1 min. Normal 4 L. Ration-FEV1/FVC=4/5=80%..")
14
Restrictive Lung Diseases Definition: – Reduced lung compliance – More pressure needed to expand lungs – Lungs are stiff – Pulmonary function test: Low FEV1, Low FVC (the ratio FEV1/FVC is increased 100%( normal80%) – Chest X ray show diffuse infiltration by small nodules, irregular lines, or "ground-glass shadows.“
 – Chest X ray show diffuse infiltration by small nodules, irregular lines, or ground-glass shadows.")
15
Restrictive Lung Diseases Initial injury to cells: endothelial, epithelial This is followed by reaction that end by interstitial fibrosis – stiff lung – dyspnea Damage to epithelium and vessels – abnormal ventilation-perfusion – Hypoxia – cyanosis Pulmonary hypertension – cor pulmonale

16
Restrictive Lung Diseases Types: – Chest wall abnormality (not primary lung) Deformities, kyphoscoliosis Neuromuscular disease – Primary lung disease Acute: Acute Respiratory Distress Syndrome ARDS Chronic: – Occupational: Asbestosis, silicosis, coal worker pneumoconiosis – Interstitial lung disease (interstitial pneumonia), Idiopathic pulmonary fibrosis – Immune diseases: Sarcoidosis, SLE, RA, Wegener – Physical injury: : Radiation – Drugs: Chemotherapy, methotrexate
 Deformities, kyphoscoliosis Neuromuscular disease – Primary lung disease Acute: Acute Respiratory Distress Syndrome ARDS Chronic: – Occupational: Asbestosis, silicosis, coal worker pneumoconiosis – Interstitial lung disease (interstitial pneumonia), Idiopathic pulmonary fibrosis – Immune diseases: Sarcoidosis, SLE, RA, Wegener – Physical injury: : Radiation – Drugs: Chemotherapy, methotrexate")
17
Major Categories of Chronic Interstitial Lung Disease Fibrosing Usual interstitial pneumonia (idiopathic pulmonary fibrosis) Nonspecific interstitial pneumonia Cryptogenic organizing pneumonia Associated with collagen vascular disease Pneumoconiosis Associated with therapies (drugs, radiation) Granulomatous Sarcoidosis Hypersensitivity pneumonia Eosinophilic Smoking Related Desquamative interstitial pneumonia Respiratory bronchiolitis
 Nonspecific interstitial pneumonia Cryptogenic organizing pneumonia Associated with collagen vascular disease Pneumoconiosis Associated with therapies (drugs, radiation) Granulomatous Sarcoidosis Hypersensitivity pneumonia Eosinophilic Smoking Related Desquamative interstitial pneumonia Respiratory bronchiolitis")
18
Idiopathic Pulmonary Fibrosis Is also called as Cryptogenic fibrosing alveolitis – Unknown etiology – Diffuse interstitial fibrosis – Sever hypoxemia, and cyanosis – More common in smoking Males than Females, – Occurs in individuals 40 t0 70 years old.

19
Idiopathic Pulmonary Fibrosis Pathogenesis: – Repeated cycles of Alveolar wall injury. – Alveolitis: inflammation, edema – Neutrophil, macrophages, lymphocytes – Interstitial Fibrosis – Macrophages: IL-8, FGF, TGF-beta, PDGF

20
Idiopathic Pulmonary Fibrosis Morphology: – Usual interstitial Pneumonia UIP – Random pattern of interstitial chronic inflammation, fibrosis, in variable stages – 80% idiopathic, 20% associated with collagen vascular diseases

21
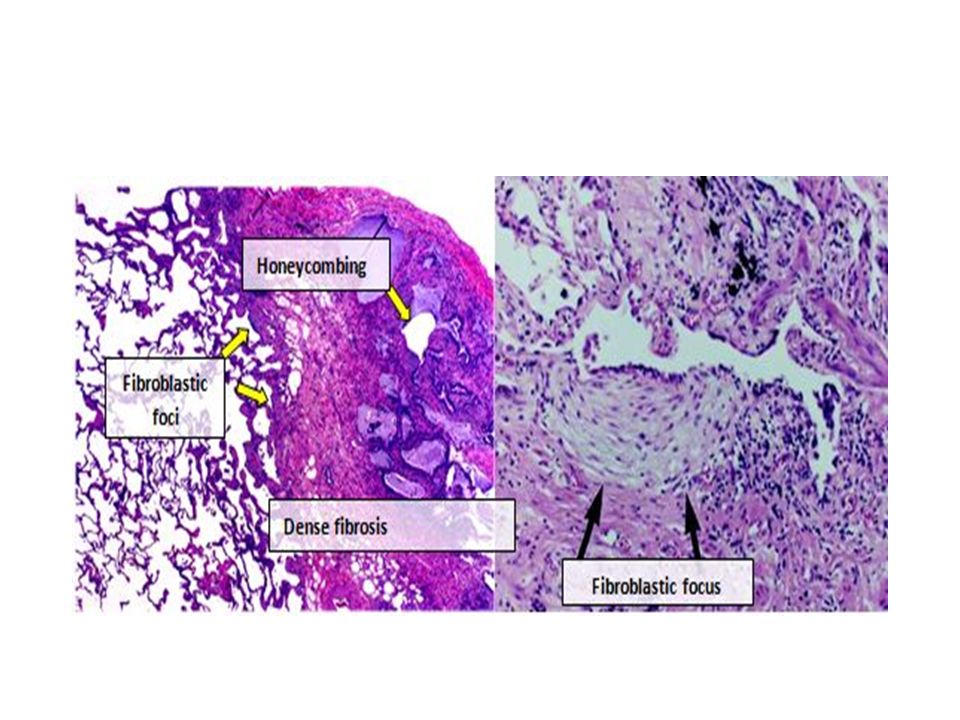
Patchy interstitial fibrosis, The earliest lesions contain exuberant fibroblastic proliferation. Honeycomb fibrosis. The dense fibrosis causes collapse of alveolar walls and formation of cystic spaces lined by hyperplastic type II pneumocytes or bronchiolar epithelium.

23
Idiopathic Pulmonary Fibrosis Clinical: – Gradual, non-productive cough – Progressive Dyspnea, cyanosis – Finger clubbing – Mean survival 2-4 years

26
Pneumoconioses Pneumoconioses- It is non neoplastic lung lesion due to Inhalation of mineral dust in to the lungs, leading to interstitial fibrosis Dust inhalation Coal dust Silica Asbestos Berylium

27
Coal dust (upper lobe) Silica (upper lobe) Asbestos (lower lobe) Beryllium : Coal workers : Stone, Ceramics, Sandblasting : Mining, Milling, Insulation : Nuclear energy, Aircraft industry
 Silica (upper lobe) Asbestos (lower lobe) Beryllium : Coal workers : Stone, Ceramics, Sandblasting : Mining, Milling, Insulation : Nuclear energy, Aircraft industry")
28
Particles that are 1 to 5 μm in diameter are the most dangerous, They get lodged at the bifurcation of the distal airways. Coal dust is relatively least fibrogenic, Asbestos, and beryllium and silica are more fibrogenic

29
The pulmonary alveolar macrophage is a key cellular element in the initiation and perpetuation of lung injury and fibrosis.

30
Coal Worker’s Pneumoconiosis (CWP) Sources of coal dust(anthracotic pigment) Coal mines, urban centers, tobacco smoke simple coalworker’s pneumoconiosis(CWP) accumulations of macrophages occur with little to no pulmonary dysfunction, complicated CWP or progressive massive fibrosis fibrosis is extensive and lung function is compromised.
 Sources of coal dust(anthracotic pigment) Coal mines, urban centers, tobacco smoke simple coalworker’s pneumoconiosis(CWP) accumulations of macrophages occur with little to no pulmonary dysfunction, complicated CWP or progressive massive fibrosis fibrosis is extensive and lung function is compromised.")
31
Pulmonary anthracosis Inhaled carbon pigment is engulfed by alveolar or interstitial macrophages, which then accumulate in the connective tissue along the lymphatics, including the pleural lymphatics, or in lymph nodes. alveolar macrophages with inhaled pigment is called as dust cells.

32
Anthracotic pigment deposition (anthracosis). Fine black pigments are deposited in the interstitium. Progressive massive fibrosis in a coal worker. Large amount of black pigment is associated with fibrosis

33
Simple CWP coal macules larger coal nodule. The coal macule- dust-laden macrophages; The coalnodule- small amounts of collagen fibers. Fibrotic opacities smaller than 1 cm in upper lobes or upper portions of the lower lobes. Coal deposits -produce centrilobular emphysema

34
Complicated CWP (PMF) coal nodules generally requires many years to develop. It is characterized by usually multiple, intensely blackened scars larger than 2 cm, sometimes up to 10 cm in greatest diameter. On microscopic examination the lesions are seen to consist of dense collagen and pigment.

35
Caplan syndrome Rheumatoid nodules (Caplan nodules) in the lungs of coal miners with rheumatoid arthritis. Nodular lesions (1-10 cm in diameter) Multiple, bilateral, and usually peripheral – Microscopy Rheumatoid nodule + dust deposits – Rheumatoid nodules consist of large, central, necrotic areas surrounded by a border of chronic inflammation and palisading macrophages.
 Multiple, bilateral, and usually peripheral – Microscopy Rheumatoid nodule + dust deposits – Rheumatoid nodules consist of large, central, necrotic areas surrounded by a border of chronic inflammation and palisading macrophages..")
36
Silicosis Inhalation of silicon dioxide (silica) Silicosis is currently the most prevalent chronic occupational disease in the world. Sandblasters Stone cutting Polishing and sharpening of metals Ceramic manufacturing Foundry work

37
Silica occurs in Crystalline most toxic and fibrogenic.(quartz) crystalline silica from occupational sources is carcinogenic in humans. Amorphous forms, After inhalation Ingested silica particles cause activation and release of mediators by pulmonary macrophages. IL-1, TNF, fibronectin, lipid mediators, oxygen-derived free radicals, and fibrogenic cytokines.

38
Silicotic nodules tiny, barely palpable, discrete, pale-to-blackened nodules in the upper zones of the lungs. eggshell”calcification thin sheets of calcification occur in the lymph nodes. Silicosis is associated with an increased susceptibility to tuberculosis.

39
The nodular lesions consist of concentric layers of hyalinized collagen Surrounded by a dense capsule of more condensed collagen Examination of the nodules by polarized microscopy reveals the birefringent silica particles.

40
Asbestos is a naturally occurring fibrous silicate that was widely used in the past for commercial applications because of its heat-resistance properties. Geometric forms of asbestos: 1. Amphibole (straight, stiff) Produces interstitial fibrosis, lung cancer and mesothelioma. 2. Serpentine (curly and flexible fibers; 90% used in wide-world). Produces lung cancer and interstitial fibrosis.
 Produces interstitial fibrosis, lung cancer and mesothelioma. 2. Serpentine (curly and flexible fibers; 90% used in wide-world). Produces lung cancer and interstitial fibrosis..")
41
Asbestos exposure has been industrial or occupational and primarily affects workers involved in: mining or processing asbestos shipbuilding construction textile insulation-manufacturing industries However, because the latency period between an initial exposure and the development of most asbestos-related disease is 20 years or longer, Asbestos-related disease remains an important public health issue.

42
Asbestosis Occupational exposure to asbestos parenchymal interstitial fibrosis (asbestosis); localized fibrous plaques pleural effusions; lung carcinomas; malignant pleural peritoneal mesotheliomas; laryngeal carcinoma.
; localized fibrous plaques pleural effusions; lung carcinomas; malignant pleural peritoneal mesotheliomas; laryngeal carcinoma.")
43
Appears in tissue, ferruginous body- Fibers coated with iron and protein. Macrophages engulf them and coat the fibers with ferritin. Asbestos bodies- Golden beaded appearance in sputum or small airways.

44
Lower lobes and subpleural Diffuse pulmonary interstitial fibrosis

45
Asbestos fibers coated with an iron-containing proteinaceous material (ferruginous body)
")
46
Asbestos-Related Lung Disease & Complications Benign pleural plaques Most common and and asymptomatic Calcified plaques on pleura and dome of the diaphragm Not a precurssor lesion for mesothelioma Diffuse pleural fibrosis with or without pleural effusion Primary Bronchogenic carcinoma Latent period aftyer 20 year exposure Risk increase with tobacco smoking Malignant mesothelioma (80% pleural; 20% peritoneal in origin) 25 to 40 years after 1 st exposure. Complications Corpulmonale, Pulmonary hypertension

47
asbestos bodies– golden brown, fusiform or beaded rods with a translucent center. Pleural plaques-are well-circumscribed plaques of dense collagen. Site-anterior and posterolateral aspects of the parietal pleura.

48
Berryliosis Aerospace industry Dusts/fumes of berrylium Acute pneumonitis (high doses) Pulmonary/systemic non caseating granulomatous lesions Progressively fibrotic lung pathology.
 Pulmonary/systemic non caseating granulomatous lesions Progressively fibrotic lung pathology.")
49
Sarcoidosis Multisystem disease Unknown etiology Accounts for 25% of Interstitial lung disease. Non-caseating granuloma in many tissues and organs. Common in blacks and Higher in non-smokers More common in women than men Adult, younger than <40y

50
Sarcoidosis Presenting Picture: – Bilateral hilar lymphadenopathy – Lung involvement, lung nodules – Other organs: skin, eye, any tissue.

51
Sarcoidosis Pathogenesis – Unknown cause – Immunologic factors Activated CD4 T cells Increase number of CD4 Tcells High level f IL-2, Interferon-gamma, IL-8, TNF – Genetic factors: Familial, racial clustering Association with HLA-A1, HLA-B8 – Environmental factors ? Viral infection, mycobacteria

52
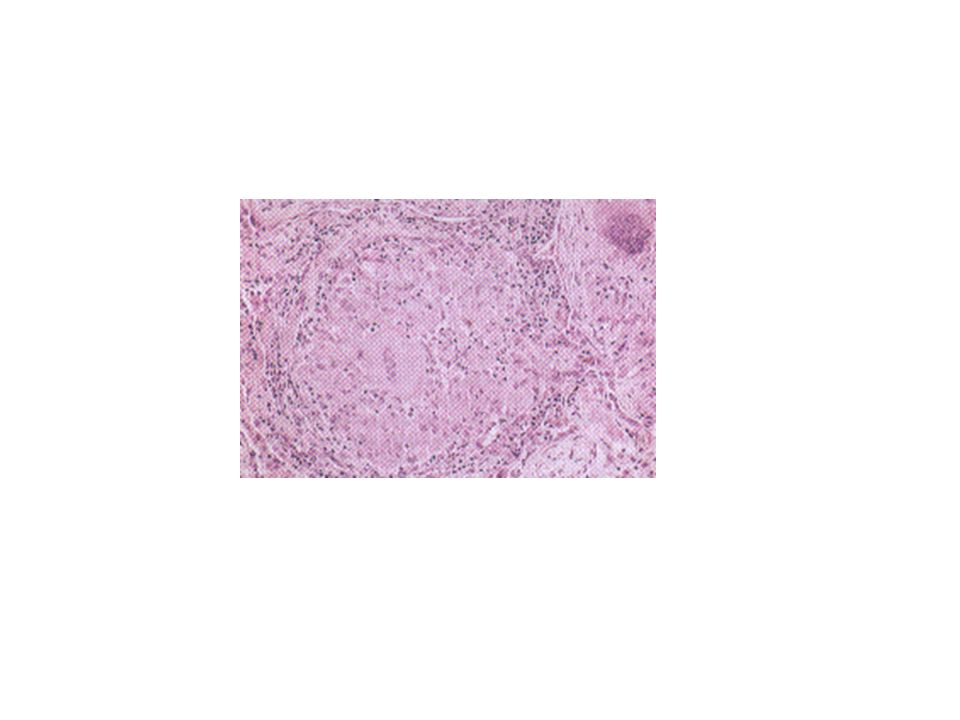
Sarcoidosis Morphology: – Non-caseating granuloma – Collection of epithelioid histiocytes rimmed by CD4 T-cells and fibroblasts – Giant cells – Schqumann bodies (calcium and protein) – Asteroid bodies (inclusions)
 – Asteroid bodies (inclusions)")
54
Sarcoidosis Hilar and paratracheal lymph nodes 75-90% Lung involvement in 90% Diffuse interstitial fibrosis 5-15% Sking 25% – Erythema nodosum: raised, tender, nodule on anterior aspect of legs Eye, Lacrimal glands (sicca syndrome). – Iritis, loss of vision – Choroiditis, retinitis – Mikulicz syndrome-- Parotid gland 10%, Spleen 75%, Liver, Bone marrow, any orga.n

55
Sarcoidosis Clinical: – Asymptomatic in many – Lymphadenopathy, skin, eye lesion – Respiratory disease: dyspnea, dry cough – Fever, fatigue, wt. Loss – Unpredictable course – Progressive or relapsing remitting disease – 10% develop progressive fibrosis

56
Hypersensitivity Pneumonitis Immune mediated disease Type III and type IV hypersensitivity Inflammatory disease Affect alveoli (mainly) (Allergic Alveolitis) Occupational disease Restrictive disease
 (Allergic Alveolitis) Occupational disease Restrictive disease")
58
Hypersensitivity Pneumonitis Presentation: – Acute: 4-6 hours following exposure, Fever, cough dyspnea – Chronic: cough, dyspnea, wt. Loss –

59
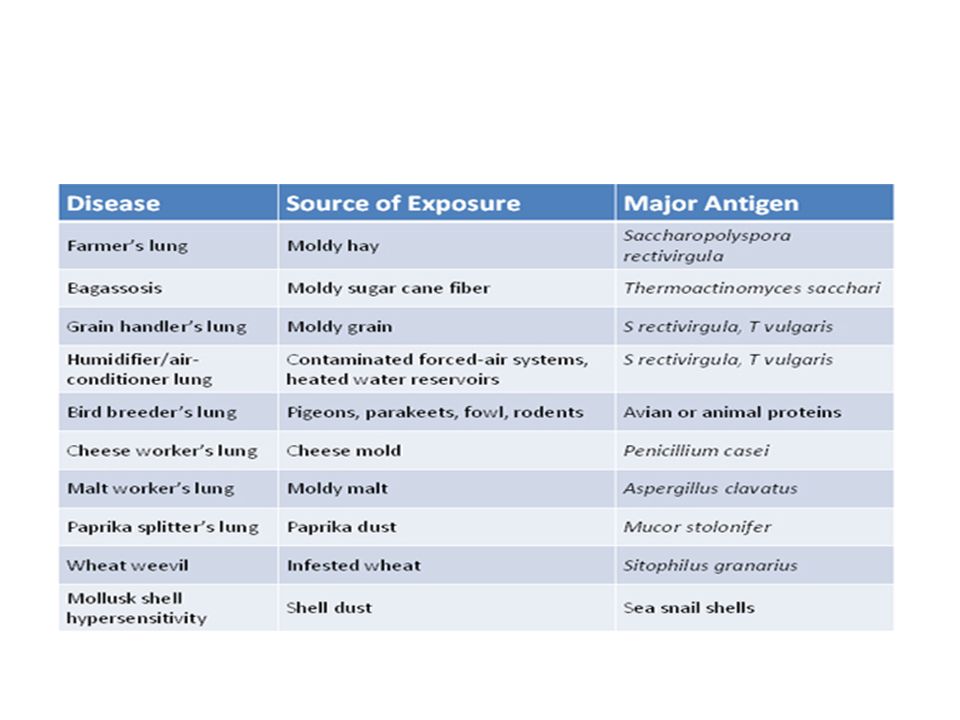
Hypersensitivity Pneumonitis Causes – Fungal/Bacterial Farmer lung: micropolyspora Humidifier lung: Actinomycetes Cheese washer’s lung: Penicillium – Animal Product Pigeon breeder’s lung – Chemicals

60
Hypersensitivity Pneumonitis Morphology: – Particles: not usually seen – Inflammation, edema, Peribronchial – Lymphocytes, plasma cells – Non-caseating granuloma – Fibrosis

61
Pulmonary Eosinophilia Acute eosinophilic pneumonia with respiratory failure, fever, dyspnea, hypoxia, and diffuse pulmonary infiltrates on chest radiograms. The bronchioalveolar lavage fluid typically contains more than 25% eosinophils. There is prompt response to corticosteroids. Simple pulmonary eosinophilia (Löffler syndrome), characterized by transient pulmonary lesions, eosinophilia in the blood, and a benign clinical course. The alveolar septa are thickened by an infiltrate containing eosinophils and occasional giant cells.
, characterized by transient pulmonary lesions, eosinophilia in the blood, and a benign clinical course. The alveolar septa are thickened by an infiltrate containing eosinophils and occasional giant cells..")
62
Tropical eosinophilia, caused by infection with microfilariae, a parasite. Secondary eosinophilia, asthma, drug allergies, and certain forms of vasculitis. Idiopathic chronic eosinophilic pneumonia, characterized by aggregates of lymphocytes and eosinophils within the septal walls and the alveolar spaces high fever, night sweats, and dyspnea.

Similar presentations

 Infections (pneumonia, airways disease)>")


>")




 Dr. Meg-angela Christi Amores.>")










