Download presentation
Presentation is loading. Please wait.

1
Pharmacological Management of ADHD and Associated Comorbidities Regina Bussing, M.D., M.S.H.S. Professor, Division of Child and Adolescent Psychiatry

2
ADHD: Etiology and Prevalence Etiology No single cause No single cause Many possible etiologies Many possible etiologies Genetic causation increasingly implicated Genetic causation increasingly implicatedPrevalence Estimates in school-age children: 3% to 9% Estimates in school-age children: 3% to 9% More commonly diagnosed in boys (4:1 to 9:1) More commonly diagnosed in boys (4:1 to 9:1) Girls were under-represented in clinical populations, but increasing numbers of girls receiving ADHD treatment Girls were under-represented in clinical populations, but increasing numbers of girls receiving ADHD treatment More prevalent in 1st degree biologic relatives More prevalent in 1st degree biologic relatives Ref: Greenhill 1993; Biederman 1989; Safer 1988; Lambert 1981
 More commonly diagnosed in boys (4:1 to 9:1) Girls were under-represented in clinical populations, but increasing numbers of girls receiving ADHD treatment Girls were under-represented in clinical populations, but increasing numbers of girls receiving ADHD treatment More prevalent in 1st degree biologic relatives More prevalent in 1st degree biologic relatives Ref: Greenhill 1993; Biederman 1989; Safer 1988; Lambert 1981")
3
Percent of Youth (4-17y) ever diagnosed Percent of Youth (4-17y) ever diagnosed and currently medicated National Survey of Children's Health, 2003: Attention- Deficit/Hyperactivity Disorder Source: http://www.cdc.gov/ncbddd/adhd/default.htm
 ever diagnosed Percent of Youth (4-17y) ever diagnosed and currently medicated National Survey of Children s Health, 2003: Attention- Deficit/Hyperactivity Disorder Source:")
4
ADHD: Core Symptoms Varying degrees of: Inattention Inattention Hyperactivity Hyperactivity Impulsivity Impulsivity Symptoms also vary in: Degree of impairment Degree of impairment Frequency of occurrence Frequency of occurrence Pervasiveness Pervasiveness Ref: Greenhill 1993; Swanson 1992; Cantwell 1985

5
DSM-IV ADHD Criteria: Inattention Symptoms Behaviors manifested often: Careless mistakes Careless mistakes Difficulty sustaining attention Difficulty sustaining attention Seems not to listen Seems not to listen Fails to finish tasks Fails to finish tasks Difficulty organizing Difficulty organizing Avoids tasks requiring sustained attention Avoids tasks requiring sustained attention Loses things Loses things Easily distracted Easily distracted Forgetful Forgetful Ref: APA 1994

6
DSM-IV ADHD Criteria: Hyperactivity/Impulsivity Symptoms Hyperactivity behaviors manifested often: Difficulty engaging in leisure activities quietly Difficulty engaging in leisure activities quietly Fidgeting Fidgeting Unable to stay seated Unable to stay seated Moving excessively (restlessness) Moving excessively (restlessness) “On the go” “On the go” Talking excessively Talking excessively Impulsivity behaviors manifested often: Blurting out answer before question is completed Blurting out answer before question is completed Difficulty waiting turn Difficulty waiting turn Interrupting/intruding upon others Interrupting/intruding upon others Ref: APA 1994
 Moving excessively (restlessness) On the go On the go Talking excessively Talking excessively Impulsivity behaviors manifested often: Blurting out answer before question is completed Blurting out answer before question is completed Difficulty waiting turn Difficulty waiting turn Interrupting/intruding upon others Interrupting/intruding upon others Ref: APA 1994")
7
ADHD: DSM-IV General Criteria and Subtypes Inattention and hyperactivity-impulsivity symptoms: Onset before age 7 Onset before age 7 Present for > 6 months Present for > 6 months Present in 2 settings (e.g., home, school, work) Present in 2 settings (e.g., home, school, work)Subtypes: AD/HD, combined type: criteria from both dimensions AD/HD, combined type: criteria from both dimensions –6 of 9 from both symptom lists AD/HD, predominantly inattentive type: inattentive criteria AD/HD, predominantly inattentive type: inattentive criteria –6 of 9 inattentive symptoms AD/HD, predominantly hyperactive-impulsive type: hyperactive-impulsive criteria AD/HD, predominantly hyperactive-impulsive type: hyperactive-impulsive criteria –6 of 9 hyperactive-impulsive symptoms Ref: APA 1994
 Present in 2 settings (e.g., home, school, work)Subtypes: AD/HD, combined type: criteria from both dimensions AD/HD, combined type: criteria from both dimensions –6 of 9 from both symptom lists AD/HD, predominantly inattentive type: inattentive criteria AD/HD, predominantly inattentive type: inattentive criteria –6 of 9 inattentive symptoms AD/HD, predominantly hyperactive-impulsive type: hyperactive-impulsive criteria AD/HD, predominantly hyperactive-impulsive type: hyperactive-impulsive criteria –6 of 9 hyperactive-impulsive symptoms Ref: APA 1994")
8
ADHD: Context for Pharmacological Treatment - Overview of Assessment Process What is the child’s developmental level? What is the child’s developmental level? Does the child meet criteria for ADHD? Does the child meet criteria for ADHD? What are the areas of functional impairment? What are the areas of functional impairment? What comorbidities are present? What comorbidities are present? What is family history of mental disorders? What is family history of mental disorders? What are the strengths of the child, family, school setting and social environment? What are the strengths of the child, family, school setting and social environment? What treatment plan is indicated? What treatment plan is indicated?

9
ADHD: Patient Evaluation Procedures Parent/child interviewsParent/child interviews Parent-child observationParent-child observation Behavior rating scalesBehavior rating scales Physical examination (including neurologic)Physical examination (including neurologic) Cognitive testing (as indicated)Cognitive testing (as indicated) Other studiesOther studies – Check on audiology/vision testing – Laboratory studies are not pathognomonic Ref: Reiff 1993
Physical examination (including neurologic) Cognitive testing (as indicated)Cognitive testing (as indicated) Other studiesOther studies – Check on audiology/vision testing – Laboratory studies are not pathognomonic Ref: Reiff 1993")
10
Differential diagnosis and possible comorbidities of childhood ADHD Ref: Reiff 1993; Barkley 1990

11
ADHD: Comorbidities in Children/Adolescents Learning disordersLearning disorders Language and communication disordersLanguage and communication disorders Oppositional defiant disorderOppositional defiant disorder Conduct disordersConduct disorders Anxiety disordersAnxiety disorders Mood disordersMood disorders Tourette’s syndrome; chronic ticsTourette’s syndrome; chronic tics Ref: Biederman 1991; Hinshaw 1987

12
Historical Context 1902 G. F. Still “Defect in Moral Control” 1937 Amphetamine reduces disruptive behavior 1956 Ritalin introduced DSM-II 1968 Hyperkinetic Reaction of Childhood DSM-III 1980 ADD/+-Hyper DSM-IV 1994 AD/HD 1998 NIH Consensus Conference 2000 -2005 Concerta, Metadate CD, Ritalin LA, Strattera, Focalin XR Minimal Brain Dysfunction 1900 1910 1920 1930 1940 1950 1960 1970 1980 1990 2000 2011 Post-encephalitic Behavior Disorder Period of Increasing Access and Medication Use: 1987–96 Medicaid/HMO prescription studies 1989–99 NAMCS studies 1987-97 NMES/MEPS studies Period of “Use Attenuation”: 1997-02 MEPS 2001-04 NHANES 2003 NCHS 2006 NHIS

13
MMWR, September 2, 2005 / 54(34);842-847 United States 2003 (NCHS) Reflects variations in prevalence, parental help seeking, provider practice patterns and other factors
; United States 2003 (NCHS) Reflects variations in prevalence, parental help seeking, provider practice patterns and other factors")
16
ADHD Pharmacotherapy Stimulants — Methylphenidate-based — Dextroamphetamine-based — Mixed Amphetamine Salts Non-Stimulant — Atomoxetine Other (Off-label, but with EB) — — Antidepressants — — Antihypertensives
 — — Antidepressants — — Antihypertensives")
17
Long-Acting Stimulant Agents AMPHETAMINE-BASEDMETHYLPHENIDATE-BASED D-ISOMERD/L-ISOMER 3:1 ratio STEREO-ISOMERD-ISOMER ® Dexedrine Spansule ® ® Adderall XR ® 2001 Adult approval ® Concerta ® 2000 ® Metadate CD ® 2001 ® Ritalin LA ® 2002 ® Focalin XR ® 2005 Adult approval OROSDIFFUCAPSSODAS Microtrol Beads 50% IR 50% DR Tri-layer core 22% IR 78% DR Multiparticulate beads 30% IR 70% DR Bead mix 50% IR 50% DR Bead mix 50% IR 50% DR Start: 10mg Max: 40mg Start: 20mg Max: 40mg Start: 36mg Max: 72mg Start: 20mg Max: 60mg Start: 20mg Max: 60mg Start: 10mg Max: 20mg 5, 10, 15 mg 5, 10, 15, 20, 25, 30 mg 18, 27,36, 54 mg 10, 20, 30 mg10, 20, 30, 40 mg 5, 10, 20 mg

18
Begin ADHD algorithm

20
ADHD and Other Disruptive Disorders ODD ODD –Diagnosis: Similar age of onset, course Similar age of onset, course Likely the most frequent comorbidity encountered Likely the most frequent comorbidity encountered Prompts specialty mental health referral (over-represented) Prompts specialty mental health referral (over-represented) –Treatment implications Family and patient education Family and patient education Raises caregiver stress more than ADHD or CD Raises caregiver stress more than ADHD or CD Psychotherapy choices (PCIT; parenting interventions) Psychotherapy choices (PCIT; parenting interventions) Medication implications (stimulants; non-stimulant ADHD treatments; alpha agonists) Medication implications (stimulants; non-stimulant ADHD treatments; alpha agonists)
 Prompts specialty mental health referral (over-represented) –Treatment implications Family and patient education Family and patient education Raises caregiver stress more than ADHD or CD Raises caregiver stress more than ADHD or CD Psychotherapy choices (PCIT; parenting interventions) Psychotherapy choices (PCIT; parenting interventions) Medication implications (stimulants; non-stimulant ADHD treatments; alpha agonists) Medication implications (stimulants; non-stimulant ADHD treatments; alpha agonists)")
21
ADHD and Other Disruptive Disorders CD CD –Diagnosis: Variations in age of onset, course Variations in age of onset, course Comorbidity with significant prognostic impact (increased risk of drug abuse; antisocial behaviors) Comorbidity with significant prognostic impact (increased risk of drug abuse; antisocial behaviors) –Treatment implications Family likely has significant other risk factors Family likely has significant other risk factors Psychotherapy choices (PCIT; parenting interventions; MST) Psychotherapy choices (PCIT; parenting interventions; MST) Medication implications (stimulants; non-stimulant ADHD treatments; atypical neuroleptics; possibly mood stabilizers for anti-aggressive effects) Medication implications (stimulants; non-stimulant ADHD treatments; atypical neuroleptics; possibly mood stabilizers for anti-aggressive effects)
 Comorbidity with significant prognostic impact (increased risk of drug abuse; antisocial behaviors) –Treatment implications Family likely has significant other risk factors Family likely has significant other risk factors Psychotherapy choices (PCIT; parenting interventions; MST) Psychotherapy choices (PCIT; parenting interventions; MST) Medication implications (stimulants; non-stimulant ADHD treatments; atypical neuroleptics; possibly mood stabilizers for anti-aggressive effects) Medication implications (stimulants; non-stimulant ADHD treatments; atypical neuroleptics; possibly mood stabilizers for anti-aggressive effects)")
22
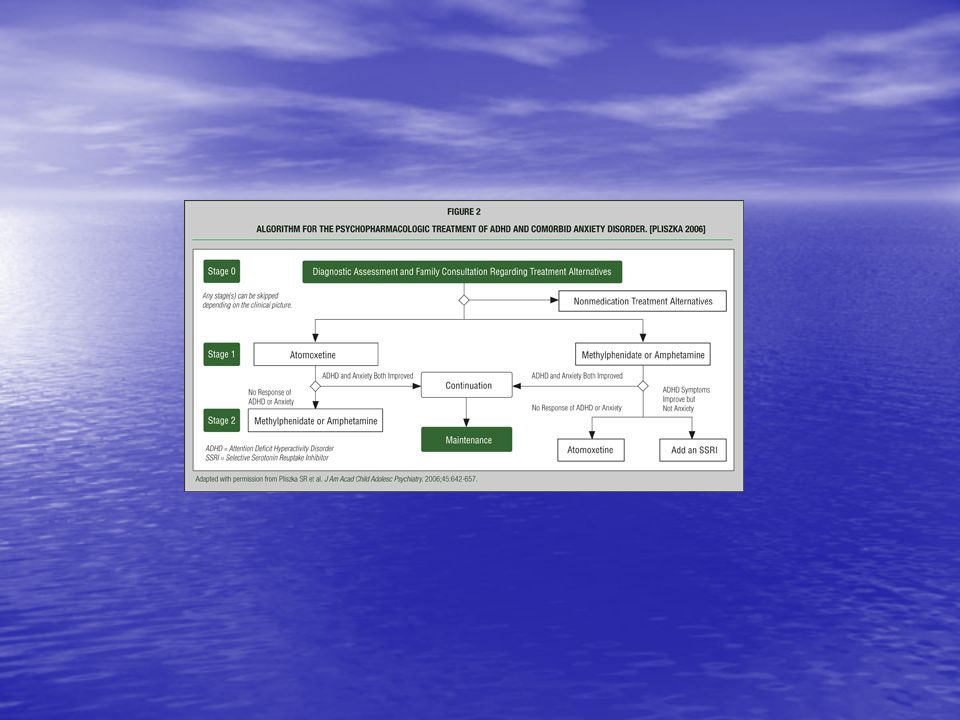
ADHD and Anxiety Disorders GAD and SAD GAD and SAD –Diagnosis: Tease out age of onset and course of symptoms Tease out age of onset and course of symptoms “Shared” symptoms (inattention, hyperactivity; academic performance problems; sleep problems) “Shared” symptoms (inattention, hyperactivity; academic performance problems; sleep problems) Unique features (worry; fears; significant somatic complaints) Unique features (worry; fears; significant somatic complaints) –Treatment implications Families may be reinforcing avoidances and fears Families may be reinforcing avoidances and fears Psychotherapy choices (CBT) Psychotherapy choices (CBT) Medication implications (stimulants; non-stimulant ADHD treatments; antidepressant options) Medication implications (stimulants; non-stimulant ADHD treatments; antidepressant options)
 Shared symptoms (inattention, hyperactivity; academic performance problems; sleep problems) Unique features (worry; fears; significant somatic complaints) Unique features (worry; fears; significant somatic complaints) –Treatment implications Families may be reinforcing avoidances and fears Families may be reinforcing avoidances and fears Psychotherapy choices (CBT) Psychotherapy choices (CBT) Medication implications (stimulants; non-stimulant ADHD treatments; antidepressant options) Medication implications (stimulants; non-stimulant ADHD treatments; antidepressant options)")
23
ADHD and Anxiety Disorders PTSD PTSD –Diagnosis: Identify stressor event Identify stressor event Tease out age of onset and course of symptoms Tease out age of onset and course of symptoms “Shared” symptoms (inattention, hyperactivity; academic performance problems; sleep problems) “Shared” symptoms (inattention, hyperactivity; academic performance problems; sleep problems) –Treatment implications Families often have significant other stressors Families often have significant other stressors Psychotherapy choices Psychotherapy choices Medication implications (stimulants; non-stimulant ADHD treatments; antidepressant options) Medication implications (stimulants; non-stimulant ADHD treatments; antidepressant options)
 Shared symptoms (inattention, hyperactivity; academic performance problems; sleep problems) –Treatment implications Families often have significant other stressors Families often have significant other stressors Psychotherapy choices Psychotherapy choices Medication implications (stimulants; non-stimulant ADHD treatments; antidepressant options) Medication implications (stimulants; non-stimulant ADHD treatments; antidepressant options)")
24
ADHD and Mood Disorders Major Depression/Dysthymia Major Depression/Dysthymia –Diagnosis: Differentiate age of onset, course Differentiate age of onset, course “Shared” symptoms (inattention, academic performance problems; sleep problems) “Shared” symptoms (inattention, academic performance problems; sleep problems) –Treatment implications Family and patient education Family and patient education Psychotherapy choices (CBT; IPT; DBT) Psychotherapy choices (CBT; IPT; DBT) Medication implications (stimulants; non-stimulant ADHD treatments; antidepressant options) Medication implications (stimulants; non-stimulant ADHD treatments; antidepressant options)
 Shared symptoms (inattention, academic performance problems; sleep problems) –Treatment implications Family and patient education Family and patient education Psychotherapy choices (CBT; IPT; DBT) Psychotherapy choices (CBT; IPT; DBT) Medication implications (stimulants; non-stimulant ADHD treatments; antidepressant options) Medication implications (stimulants; non-stimulant ADHD treatments; antidepressant options)")
25
ADHD and Mood Disorders Bipolar Disorder Bipolar Disorder –Diagnosis: Differentiate age of onset, course (issues of mixed presentation and of rapid cycling) Differentiate age of onset, course (issues of mixed presentation and of rapid cycling) “Shared” symptoms (attention problems; hyperactivity; increased speech output; loud; sleep problems; academic performance problems) “Shared” symptoms (attention problems; hyperactivity; increased speech output; loud; sleep problems; academic performance problems) Unique symptoms (grandiosity; psychotic symptoms; severe mood lability; severe aggression) Unique symptoms (grandiosity; psychotic symptoms; severe mood lability; severe aggression) –Treatment implications Family and patient education Family and patient education Medication implications (mood stabilizers; atypical neuroleptic medications; issue of stimulants; non-stimulant ADHD treatments; antidepressant options) Medication implications (mood stabilizers; atypical neuroleptic medications; issue of stimulants; non-stimulant ADHD treatments; antidepressant options)
 Differentiate age of onset, course (issues of mixed presentation and of rapid cycling) Shared symptoms (attention problems; hyperactivity; increased speech output; loud; sleep problems; academic performance problems) Shared symptoms (attention problems; hyperactivity; increased speech output; loud; sleep problems; academic performance problems) Unique symptoms (grandiosity; psychotic symptoms; severe mood lability; severe aggression) Unique symptoms (grandiosity; psychotic symptoms; severe mood lability; severe aggression) –Treatment implications Family and patient education Family and patient education Medication implications (mood stabilizers; atypical neuroleptic medications; issue of stimulants; non-stimulant ADHD treatments; antidepressant options) Medication implications (mood stabilizers; atypical neuroleptic medications; issue of stimulants; non-stimulant ADHD treatments; antidepressant options)")
26
ADHD and Tic Disorders Chronic Tics or Tourette’s Disorder Chronic Tics or Tourette’s Disorder –Onset of ADHD often precedes onset of Tics or TS –Important to inquire about family history and educate parents about stimulants and tics/TS Treatment Treatment –Stimulants were considered “contraindicated” in past –Focus now on improving functioning – ADHD may be more impairing than tics –Complex regimens may be used, combining ADHD medications with alpha-agonists and/or atypical neuroleptic medications

27
Case Example Bob presented to child psychiatrist for ADHD, SLD, expressive language disorder Bob presented to child psychiatrist for ADHD, SLD, expressive language disorder Family history + ADHD, depression Family history + ADHD, depression Treated with stimulants, school interventions as preadolescent Treated with stimulants, school interventions as preadolescent Developed severe aggression, mood instability, some seasonal variations in mood in early adolescence Developed severe aggression, mood instability, some seasonal variations in mood in early adolescence Repeated inpatient crisis stabilization, family therapy, medication adjustments Repeated inpatient crisis stabilization, family therapy, medication adjustments Developed psychotic symptoms with hypomanic component Developed psychotic symptoms with hypomanic component Residential treatment pursued Residential treatment pursued

28
Bob follow-up Temporarily stopped ADHD medication treatment, used antipsychotic medications Temporarily stopped ADHD medication treatment, used antipsychotic medications Moved into mood stabilization, resumed ADHD medications once Bob had remained free of psychotic symptoms for 3 months Moved into mood stabilization, resumed ADHD medications once Bob had remained free of psychotic symptoms for 3 months Continued family intervention (“the explosive child”) Continued family intervention (“the explosive child”) Able to resume regular school attendance, with partial special education services, continued ADHD treatment, ongoing mood stabilization, off all antipsychotic medications Able to resume regular school attendance, with partial special education services, continued ADHD treatment, ongoing mood stabilization, off all antipsychotic medications Continued to experience social isolation, but markedly improved overall functioning Continued to experience social isolation, but markedly improved overall functioning Young adult outcome: subclinical ADHD symptoms without further mood disturbance; completed high school; dropped out of community college; works successfully as cook; terminated outpatient therapy and medication therapy age 22. Young adult outcome: subclinical ADHD symptoms without further mood disturbance; completed high school; dropped out of community college; works successfully as cook; terminated outpatient therapy and medication therapy age 22.

29
Questions/Discussion

Similar presentations






>")
 By: Bianca Jimenez Period:5.>")
. Diagnostic and.>")

 is one of the most common childhood disorders and can continue.>")







 Kiefer, MaryJane ED 6362 – Education of Exceptional Children Dr. M. McCloulskey Fall 2001.>")


