Download presentation
Presentation is loading. Please wait.

1
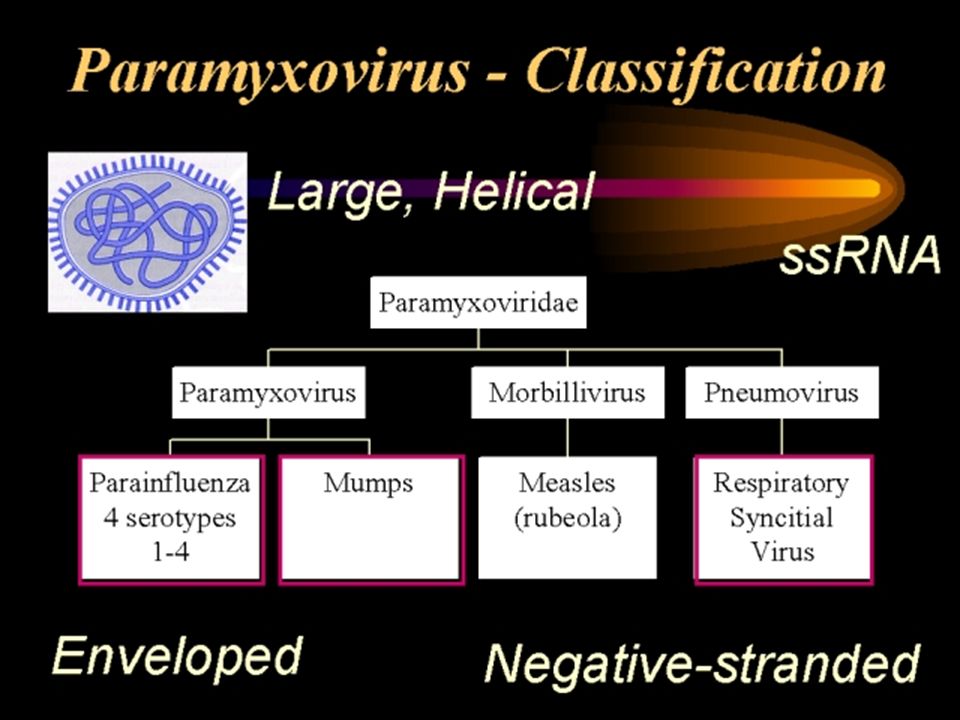
Paramyxoviridae

4
Classification of Paramyxoviruses: There are 3 genera in paramyxoviridae family: (1) Paramyxovirus: have both hemagglutinins & neuraminidase on their envelopes, includes Parainfluenza viruses & Mumps virus. (2) Morbillivirus: express only hemagglutinins on their envelopes, it include Measles virus.(rubeola). (3) Pneumovirus: don’t express neither neuraminidase nor hemagglutinins on their envelopes, Respiratory Syncytial virus.
 Morbillivirus: express only hemagglutinins on their envelopes, it include Measles virus.(rubeola). (3) Pneumovirus: don’t express neither neuraminidase nor hemagglutinins on their envelopes, Respiratory Syncytial virus..")
5
Parainfluenza viruses Includes four major serotypes 1-Parainfluenza virus type 1 & 2 infect infants & children, cause epidemics fall months. 2-Parainfluenza type 3 infects infants < 2 years of age & tends to cause more serious disease. 3-Parainfluenza type 4 cause milder disease. Clinical infections (1) Common cold all serotypes of parainfluenza virus cause common cold, usually mild. (2) Laryngotracheobronchitis (croup) commonly associated with parainfluenza type 1 & 2 in children less than 3 years of age. (3) Bronchiolitis & pneumonia caused by parainfluenza type 3.
 Common cold all serotypes of parainfluenza virus cause common cold, usually mild. (2) Laryngotracheobronchitis (croup) commonly associated with parainfluenza type 1 & 2 in children less than 3 years of age. (3) Bronchiolitis & pneumonia caused by parainfluenza type 3..")
6
Epidemiology Transmission occur through respiratory tract by inhalation of infectious aerosolized secretions, virus reach respiratory tract & produce localized respiratory infection in which viremia is rarely detected. Diagnosis (1) Culture & isolation Throat & nasal swabs are good specimens for viral isolation, primary human & monkey kidney cells are the most sensitive for isolation of parainfluenza viruses. Parainfluenza virus grow slowly & cause minimal CPE in tissue culture. (2) Serology Using paired sera & a fourfold rise in titer is indicative of infection with a parainfluenza virus. Treatment no specific treatment, supportive treatment.
 Culture & isolation Throat & nasal swabs are good specimens for viral isolation, primary human & monkey kidney cells are the most sensitive for isolation of parainfluenza viruses. Parainfluenza virus grow slowly & cause minimal CPE in tissue culture. (2) Serology Using paired sera & a fourfold rise in titer is indicative of infection with a parainfluenza virus. Treatment no specific treatment, supportive treatment..")
8
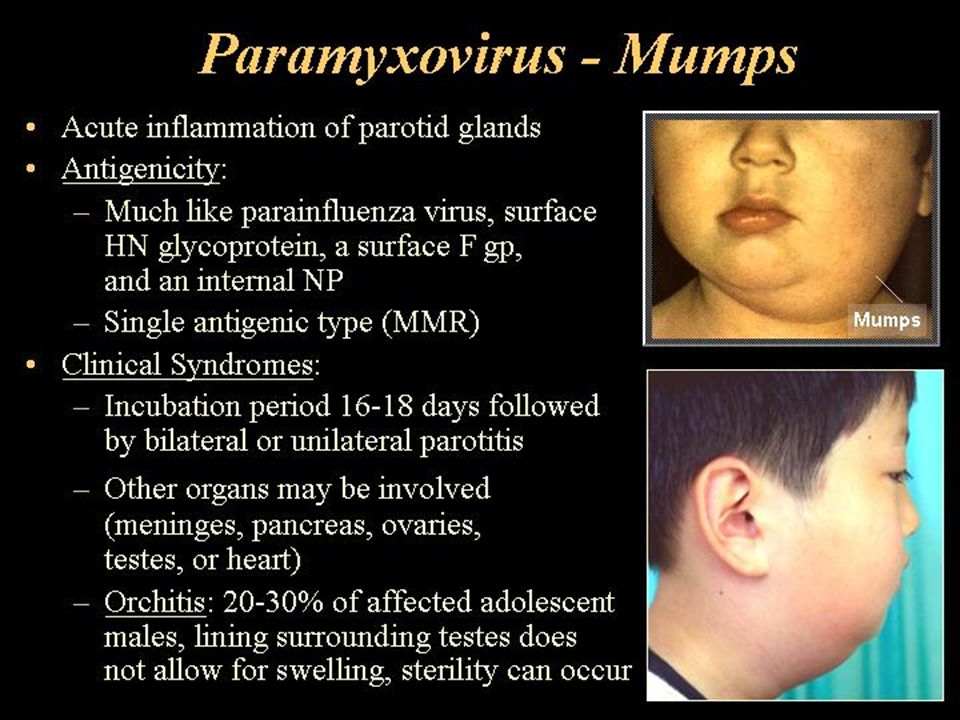
Epidemiology Mumps tends to affect school age children, its unusual in infants, because the mother antibodies remain protective for the 1st year of life. Most cases occur in late winter & early spring months. Transmission is by inhalation of contaminated aerosol droplets & favored by close contact. Mumps virus transmitted about 4 days before to 1 week after the symptoms occur. Pathogenesis:2 theories 1st theory: the virus travels from the mouth through stensons duct to parotid gland where it undergo 1ry replication, followed by generalized viremia, where the virus can infect other organ as a result of a generalized viremia. 2nd theory: After transmission of the virus through respiratory droplets the virus first replicate in the respiratory epithelium followed by generalized viremia where virus localize in salivary glands & other organs.

9
Clinical features: ~ 1/3 of infection are subclinical, whereas in those develop clinical manifestation after incubation period of 16-18 days, early symptoms of fever, anorexia, & body aches, with swelling of stensons duct, this followed in 1-2 days by unilateral or bilateral nonsuppurative swelling of parotid gland. Generalized viremia may lead to infection of testes, ovaries, pancreas, & brain, viruria usually develops during mumps. Complication of mumps virus infection: (1) Orchitis: 20-30 % of affected adolescent males, & usually unilateral & therefore doesn’t generally result in sterility. (2) Aseptic meningitis: About 10-15% of aseptic meningitis is attributed to mumps virus infection. (3) Meningoencephalitis: Incidence of this kind of complication is 2-5/1000 of mumps virus infection.Here there is more sever infection of the CNS, but permanent damage is rare. (4) Other less common complications: Unilateral nerve deafness. Pancreatitis, Thyroditis, Nephritis.
 Orchitis: % of affected adolescent males, & usually unilateral & therefore doesn’t generally result in sterility. (2) Aseptic meningitis: About 10-15% of aseptic meningitis is attributed to mumps virus infection. (3) Meningoencephalitis: Incidence of this kind of complication is 2-5/1000 of mumps virus infection.Here there is more sever infection of the CNS, but permanent damage is rare. (4) Other less common complications: Unilateral nerve deafness. Pancreatitis, Thyroditis, Nephritis..")
10
Diagnosis: (1) Clinical feature in typical cases. (2) Isolation & identification of virus: the most appropriate sample for viral isolation saliva, CSF, urine collected with few days after the onset of illness. Monkey kidney cells are preferred for viral isolation, CPE consist of cell rounding & giant cell formation. (3) Serology Ab rise can be detected using paired sera, these Abs can be detected using CF, HI test or ELISA. Treatment supportive. Prevention: (1) Live attenuated, safe, efficient vaccine. (2) Mumps Ig can be used to prevent the disease in nonimmunized individual exposed to the virus.
 Isolation & identification of virus: the most appropriate sample for viral isolation saliva, CSF, urine collected with few days after the onset of illness. Monkey kidney cells are preferred for viral isolation, CPE consist of cell rounding & giant cell formation. (3) Serology Ab rise can be detected using paired sera, these Abs can be detected using CF, HI test or ELISA. Treatment supportive. Prevention: (1) Live attenuated, safe, efficient vaccine. (2) Mumps Ig can be used to prevent the disease in nonimmunized individual exposed to the virus..")
11
Measles (Rubeola) virus acute, highly infectious, exanthematous disease with fever & respiratory symptoms. Pathogenesis Measles virus, spread by droplets & by fomites, its highly contagious viral infection ( particularly during late prodromal stage 1-2 days before rash) crowding facilitate spread. After the virus enter the body first replication occur in cells of upper respiratory tract or the conjunctival sac of the eye. Then a generalized viremia follows, & vesicles form in the buccal mucosa ( koplik s spots) before appearance of rash. Then virus localized & causes characteristics measles multinucleated giant cells in the skin, L.N., tonsils, lungs & kidney. In ~ 1 case per 1000, measles will localize in the CNS causing encephalitis.
 crowding facilitate spread. After the virus enter the body first replication occur in cells of upper respiratory tract or the conjunctival sac of the eye. Then a generalized viremia follows, & vesicles form in the buccal mucosa ( koplik s spots) before appearance of rash. Then virus localized & causes characteristics measles multinucleated giant cells in the skin, L.N., tonsils, lungs & kidney. In ~ 1 case per 1000, measles will localize in the CNS causing encephalitis..")
12
Clinical feature: IP of 10-20 days, a prodromal phase started which lasts for several days, characterized by fever, coughing, coryza, conjunctivitis, & Kopliks spots( tiny, whitish rash with erythematous base appear on buccal mucosa just above the lower molar teeth, its bilateral ) & appear at the end of prodromal phase 24-36 hours before rash appears. This follows by appearance of rash which is macculopapular rash begin as pink discrete rash that rapidly becomes red & coalescing, spread over the entire body in 2-4 days. The rash finally becomes brownish & desquamative.

14
Complication of Measles viral infection: (1) Encephalitis:(1:1000 cases) occur during or immediately following the rash with 10-30% mortality, survivors may have sequelae with seizer disorders & psychosis. (2) Subacute sclerosing panencephalitis: is a chronic degenerative neurologic disease with mental deterioration & high mortality rate, that occur several years after infection with measles virus, disease most common in children 5-10 years of age, its believed to be the result of a persistent measles infection. (3) Secondary bacterial infection of respiratory tract: Occur in 15% of cases, these infection leads to pneumonia, bronchitis & otitis media. Diagnosis:1- Clinically 2- Isolation & culture of the virus, throat swabs or respiratory secretions. 3- Serology detection of significant in Ab. titer specific to the virus. Prevention : live attenuated vaccine, given after the 1st year of life & 95-98% efficient.
 Subacute sclerosing panencephalitis: is a chronic degenerative neurologic disease with mental deterioration & high mortality rate, that occur several years after infection with measles virus, disease most common in children 5-10 years of age, its believed to be the result of a persistent measles infection. (3) Secondary bacterial infection of respiratory tract: Occur in 15% of cases, these infection leads to pneumonia, bronchitis & otitis media. Diagnosis:1- Clinically 2- Isolation & culture of the virus, throat swabs or respiratory secretions. 3- Serology detection of significant in Ab. titer specific to the virus. Prevention : live attenuated vaccine, given after the 1st year of life & 95-98% efficient..")
15
Respiratory Syncytial Virus (RSV) RSV most serious cause of bronchiolitis & pneumonia in infants < 6 months of age. Epidemiology & Pathogenesis RSV spreads in infants & young children during winter months. highly contagious & spreads by respiratory route. characterize by a short incubation period (1-4) days, with a very localized infection in the ciliated epithelium of the airways & an absence of viremia. Symptoms of fever, lethargy & apnea results as sloughing of epithelium & exudate occlude the lumen of airways. Clinical diseases: (1) Lower respiratory tract infections (bronchiolitis, pneumonia, tracheobronchitis) (major cause of brochiolitis in infant under 6 month of age) (2) Upper respiratory tract infections : manifested as common cold. (3) Complication of RSV : occur in infants includes otitis media ( common), myocarditis ( rare).
 days, with a very localized infection in the ciliated epithelium of the airways & an absence of viremia. Symptoms of fever, lethargy & apnea results as sloughing of epithelium & exudate occlude the lumen of airways. Clinical diseases: (1) Lower respiratory tract infections (bronchiolitis, pneumonia, tracheobronchitis) (major cause of brochiolitis in infant under 6 month of age) (2) Upper respiratory tract infections : manifested as common cold. (3) Complication of RSV : occur in infants includes otitis media ( common), myocarditis ( rare)..")
16
Diagnosis 1-Clinical. 2-RSV isolated using nasal swabs, inoculated at different human cell culture, give characteristics CPE in form of syncytial effect, & presence of cytoplasmic inclusion bodies in infected cells. 3-Rapid diagnostic technique by indirect immunofluorecent test ELISA to detect RSV Ag in exfoliated cells of nasal washes. 4-Serology: to detect four fold in the titer in RSV Abs detected by CF, neutralization assay & ELISA. Treatment: Ribavirin is considered drug of choice, administered by aerosol. Prevention: Life attenuated vaccine have been tried.

17
Rubella virus Rubella virus: is the only member of Rubivirus genus in Togaviridae family. General characteristics: Enveloped, with icosahedral nucleocapsid symmetry, positive sense SS RNA genome, complete virion ~ 60 nm in diameter. The hemagglutinin glycoprotein appear as projection on the surface of the virion.

18
Epidemiology: Rubella is worldwide in distribution. Infection occurs throughout the year with peak incidence in the spring. Infection is transmitted by respiratory route, but less contagious than measles. Pathogenesis: Transmission of this virus primarily by droplet infection through the URT, Ip. ~ 2 weeks. Rubella virus replicate in the cervical L.N. leads to viremia, this occurred ~ 7-14 days after exposure & is followed by a rash that lasts 2-3 days. The virus may be found in the urine & feces during viremic phase. The disease characterize by 3 days rash with generalized lymphadenopathy, & following the rash there is transient arthritis & joint pain.

19
Congenital Rubella: the virus circulate in the blood of the mother, cross the placenta & localized in the embryonic cells, multiplication of the virus causes abnormal development of fetal cells, through alteration of growth rate, dangerous effects on the fetus occurs during the first month, ~ 80% of children will have anomalies, by the third month of the first trimester anomalies develop in ~ 15% of those exposed. Transplacental infection can cause a number of problems, including abortion, miscarriage, stillbirth, & fetal anomalies associated with congenital rubella syndrome which includes: (1)-Ophthalmologic: (cataract, glaucoma, chorioretinitis). (2)-Cardiac: (PDA, pulmonary art stenosis, various septal defects). (3)-Auditory: sensorineural deafness (4)-Neurologic: mental retardation, meningoencephalitis, microcephaly. (5)-Others: growth retardation, hepatosplenomegaly, thromocytopenic purpura.
-Ophthalmologic: (cataract, glaucoma, chorioretinitis). (2)-Cardiac: (PDA, pulmonary art stenosis, various septal defects). (3)-Auditory: sensorineural deafness (4)-Neurologic: mental retardation, meningoencephalitis, microcephaly. (5)-Others: growth retardation, hepatosplenomegaly, thromocytopenic purpura..")
22
Laboratory diagnosis: (1) Viral isolation nasal or throat swab, congenital rubella virus isolated from urine, feces, CSF, & at autopsy from bone marrow & any organ. (2) Serology: a- increase in antibody titer specific for rubella in paired serum samples using hemagglutination inhibition test, ELISA, or Latex agglutination test. b- IgM specific for rubella, very useful in diagnosis of congenital rubella. Treatment: Rubella is mild self-limited illness, & no specific treatment is given. Therapeutic abortion is the only means of avoiding the risk of malformed infants if rubella infection occurred in the first 3-4 months of pregnancy. Prevention & Control: An effective live attenuated vaccine is available. Although the attenuated virus has not shown to cause clinical infection or fetal anomalies, vaccination should be withheld from pregnant women & vaccinated women should avoid pregnancy for 3 months following vaccination.
 Serology: a- increase in antibody titer specific for rubella in paired serum samples using hemagglutination inhibition test, ELISA, or Latex agglutination test. b- IgM specific for rubella, very useful in diagnosis of congenital rubella. Treatment: Rubella is mild self-limited illness, & no specific treatment is given. Therapeutic abortion is the only means of avoiding the risk of malformed infants if rubella infection occurred in the first 3-4 months of pregnancy. Prevention & Control: An effective live attenuated vaccine is available. Although the attenuated virus has not shown to cause clinical infection or fetal anomalies, vaccination should be withheld from pregnant women & vaccinated women should avoid pregnancy for 3 months following vaccination..")
Similar presentations






>")















.>")
