Download presentation
Presentation is loading. Please wait.

1
Peritoneum and Peritoneal cavity Lecture 13. Dr. Mohammad Muzammil Ahmed Assistant Professor of Anatomy and Embryology

2
OBJECTIVES Enlist functions of peritoneum Discuss the development of peritoneum and peritoneal cavity Identify general arrangement of peritoneal viscera Describe modifications of peritoneum Enumerate cavities and compartments of peritoneum Identify clinical applications (peritonitis, peritoneal pain, peritoneal dialysis and internal abdominal hernia) Suggested reading: Clinical Anatomy by Region 9th edition, page 160- 168
 Suggested reading: Clinical Anatomy by Region 9th edition, page")
3
Peritoneum It is a thin, serous, continuous glistening membrane lining the abdominal & pelvic walls and clothing the abdominal and pelvic viscera. Parietal layer lines the wall & visceral layer covers the organs. The potential space between the two layers is filled with very thin film of serous fluid to facilitate the movement of the abdominal organs. Peritoneal cavity is the largest cavity in the body. The surface area of parietal & visceral layers is enormous.

4
The peritoneal cavity It is divided into two main sacs: 1- Greater sac. 2- Lesser sac or omental bursa. These two sacs are interconnected by a single oval opening called the epiploic foramen or opening into lesser sac or foramen of Winslow

5
Intraperitoneal And Retroperitoneal Relationships Intraperitoneal organ means that the organ is completely covered by visceral layer of peritoneum e.g. stomach, jejunum, ileum & spleen. N.B. No organ lies inside the peritoneal cavity. Retroperitoneal organ means that the organ lies behind the peritoneum and partially covered by visceral peritoneum e.g. pancreas, ascending & descending colon.

6
Falciform Ligament A sickle-shaped fold of peritoneum connects the anterior abdominal wall with the liver slightly to the right of the median plane. Anterior border: Attached to under surface of diaphragm & anterior abdominal wall. Posterior border: Attached to superior & anterior surfaces of liver Free margin connects the umbilicus to liver, it contains the round ligament of the liver or Ligamentum teres. Peritoneal ligaments

7
Greater sac It is the part of peritoneal cavity which lies behind the anterior abdominal wall. Peritoneum lines the anterior abdominal wall then the under surface of diaphragm, from where it is reflected on to superior surface of liver forming the upper layer of coronary ligament

8
Then, it descends from superior surface of liver to anterior surface then inferior surface of liver. From posterior part of inferior surface peritoneum reflected on to front of right kidney & right suprarenal gland forming the lower layer of coronary ligament. The lower & upper layers of coronary ligament bound a large area on the posterior surface of the liver called bare area of the liver which has no peritoneal covering.

9
Ligaments of peritoneum attached to liver Falciform, coronary, right & left triangular ligaments Omenta Two layers of peritoneum that connect stomach to other visceral organs. Lesser & greater omenta and gastrosplenic omentum (ligament ).
..")
10
Mesentery Two layers of peritoneum connecting small intestine to post abdominal wall. It has 2 borders 1- Attached border: to post abdominal wall & 2- Free border: which encloses the jejunum & ileum. Vessels, nerves. Lymphatic enter small intestine between the two layers. Similarly mesocolon is the peritoneum for the large intestine for eg. Transverse mesocolon, sigmoid mesocolon

12
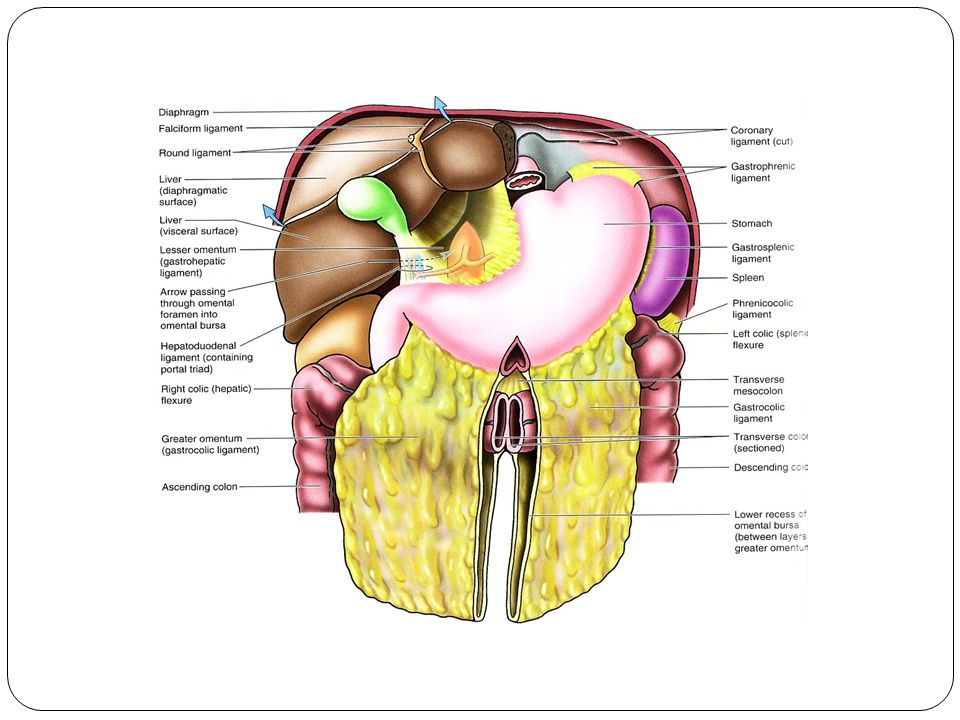
Greater Omentum Connects the greater curvature of the stomach to transverse colon. It hangs like an apron in front of the small intestine It is folded back on itself to be attached to the transverse colon.

14
Lesser Omentum Connects liver to stomach attached above to porta hepatis & fissure for ligamentum venosum inferiorly to lesser curvature of the stomach,& 1 st inch of duodenum. Its free margin contains: Portal vein: Posterior Bile duct : Anterior & right Hapatic artery: anterior &left Gastrosplenic ligament Connects the stomach to the hilum of the spleen Splenicorenal or lienorenal ligament Connects the hilum of spleen to front of the left kidney.

16
Lesser sac A peritoneal pouch lies behind stomach & lesser omentum It projects upwards as far as the diaphragm. Inferiorly it lies within the folding of the greater omentum. Its lower part is usually obliterated due to fusion of the anterior & post layers of the greater omentum.

17
Anterior wall: from above downward lesser omentum, back of stomach & anterior 2 layers of greater omentum. Posterior wall: From below upwards, posterior 2 layers of greater omentum, then the peritoneum which covers many structures on posterior abdominal wall These structures are: 1- Body of pancreas. 2- Part of abdominal aorta 3- Coeliac artery & its branches (splenic, Leftt gastric & hepatic arteries)
.")
18
4- Left crus of diaphragm. 5- Left kidney. 6- Left suprarenal gland. 7- Part of inferior phrenic artery. Upper border: Extends from porta hepatis, fissure for ligamentum venosum to lower end of esophagus. Lower border: Inferior margin of greater omentum. Left border: Left margin of greater omentum, gastrosplenic & lienorenal ligaments. Right border: Right Margin of greater omentum, opening into lesser sac.

19
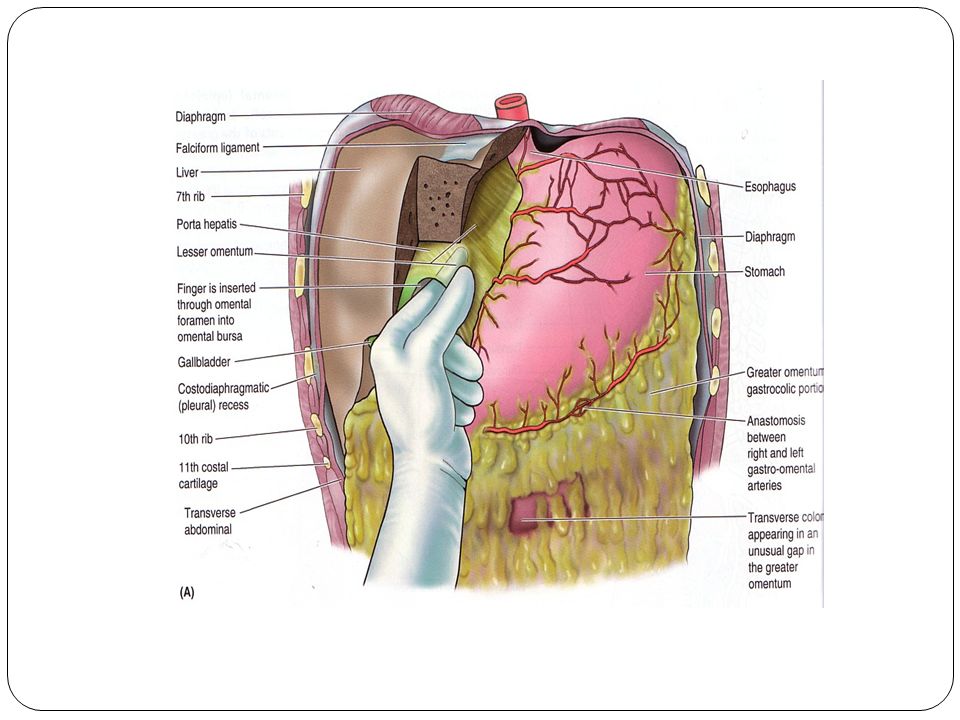
Epiploic Foramen: Boundaries Anterior: free margin of lesser omentum, containing (hepatic artery, bile duct and portal vein) Posterior: peritoneum covering Inferior Venacava. Superior: Caudate process of the caudate lobe of the liver. Inferior: 1 st inch of the1 st part of duodenum.

20
Peritoneal Recesses, Spaces, and Gutters Duodenal Recesses there may be four small pocket like pouches of peritoneum called the superior duodenal, inferiorduodenal, paraduodenal,and retroduodenal recesses. Cecal Recesses three peritoneal recesses called the superior ileocecal, the inferior ileocecal, and the retrocecal recesses.

21
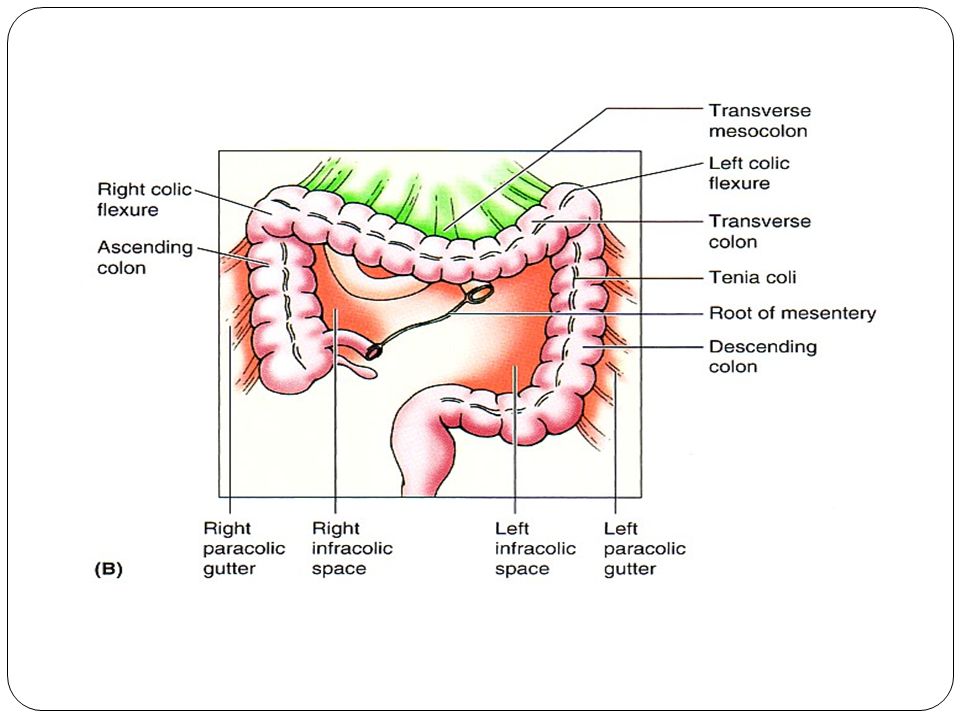
Intersigmoid Recess The intersigmoid recess is situated at the apex of the inverted,V-shaped root of the sigmoid mesocolon its mouth opens downward. Subphrenic Spaces The right and left anterior subphrenic spaces lie between the diaphragm and the liver, on each side of the falciform Ligament. The right posterior subphrenic space lies between the right lobe of the liver, the right kidney, and the right colic flexure. The right extraperitoneal space lies between the layers of the coronary ligament and is therefore situated between the liver and the diaphragm. The paracolic gutters lies lateral and medial to the ascending and descending colon respectively.

22
Function of peritoneum It suspend the organs within the peritoneal cavity. It fixes some organs within the abdominal cavity. Storage of large amount of fat in the peritoneal ligaments (e.g.. Greater omentum) Peritoneal covering of intestine tends to stick together in infection Greater omentum is called the policeman of abdomen to prevent spread of infection It secretes the peritoneal fluid which helps in the gliding of the mobile viscera over one another.
 Peritoneal covering of intestine tends to stick together in infection Greater omentum is called the policeman of abdomen to prevent spread of infection It secretes the peritoneal fluid which helps in the gliding of the mobile viscera over one another..")
23
Innervation of peritoneum: Parietal peritoneum is sensitive to pain, pressure, temperature & touch,(pptt) Parietal peritoneum is supplied by: Lower 6 thoracic nerves (T7-- T12) First lumber nerve ( L1) Central part of diaphragmatic parietal peritoneum is supplied by Phrenic nerve. Peripherally supplied by lower 6 thoracic nerves and in the pelvis supplied by the Obturator nerve. Visceral peritoneum is sensitive to stretch & tearing. It is supplied by autonomic afferent nerves which supply the viscera.

24
Development of peritoneum and peritoneal cavity The peritoneum develops from the lateral plate mesoderm. The lateral plate mesoderm splits to form 2 layers- the parietal(somatic)layer and the visceral (splanchnic) layer The visceral and the parietal layers becomes continuous with each other as the dorsal mesentry, Ventral mesentry is derived from the thinning of the septum transversum. The peritoneal cavity is derived from that part of the embryonic coelom situated caudal to the septum transversum.
layer and the visceral (splanchnic) layer The visceral and the parietal layers becomes continuous with each other as the dorsal mesentry, Ventral mesentry is derived from the thinning of the septum transversum. The peritoneal cavity is derived from that part of the embryonic coelom situated caudal to the septum transversum..")
25
Ascites: Is the excessive accumulation of the peritoneal fluid within the peritoneal cavity.. The infection may spread into the peritoneal cavity and cause inflammation of the peritoneum which is called as peritonitis. The infected fluid may tend to collect in the most dependent area of the peritoneal cavity in supine position, these areas are pelvis and the right subphrenic space. In such condition the patient complains of pain in the shoulder. Peritoneal Pain: abdominal pain arising due to the parietal peritoneum can be localised as it is supplied by the somatic nerves T7-T12 and L1. An inflamed parietal peritoneum is extremely sensitive to stretching. This fact is made use of clinically in diagnosing peritonitis. Pressure is applied to the abdominal wall with a single finger over the site of the inflammation. The pressure is then removed by suddenly withdrawing the finger. The abdominal wall rebounds, resulting in extreme local pain, which is known as rebound tenderness Applied anatomy

26
Pain arising from the visceral peritoneum is dull and poorly localized as the visceral peritoneum is supplied by the autonomic nerves. Peritoneal Dialysis: Because the peritoneum is a semi permeable membrane, it allows rapid bidirectional transfer of substances across itself. Because the surface area of the peritoneum is enormous, this transfer property has been made use of in patients with acute renal insufficiency. Internal abdominal hernia: occasionally a loop of intestine may enter into the peritoneal pouch or recesses and gets strangulated, this is called as internal abdominal hernia.

Similar presentations