Download presentation
Presentation is loading. Please wait.

2
Defining abnormality is not simple, it appears to be more a matter of degree of behavioral change and distress rather than the presence or absence of a behavioral change or distress Some criterion that is helpful in defining abnormality Behavior is outside of social norms Inability to function Personal Distress Prolonged Suffering (ex: depression that lasts months rather than days)
")
3
Psychological Disorder **** a “harmful dysfunction” in which behavior is judged to be: Rare Disturbing to the person or others Maladaptive Dangerous

4
Psychological Disorders Medical Model concept that diseases have physical causes can be diagnosed, treated, and in most cases cured assumes that these mental illnesses can be diagnosed on the basis of their symptoms and cured through therapy which may include treatment in a psychiatric hospital

5
Psychological Disorders Bio-Psycho-Social Perspective assumes that biological, social, cultural, and psychological factors combine and interact to produce psychological disorders

6
Psychological Disorders

7
Classifying Psychological Disorders DSM-IV American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition) a widely used system for classifying psychological disorders presently distributed as DSM-IV-TR (text revision)
 a widely used system for classifying psychological disorders presently distributed as DSM-IV-TR (text revision)")
8
DSM IV-TR Five axis criteria for diagnostic classification of psychological disorders Axis 1: Clinical Syndromes Axis 2: Personality Disorders Axis 3: Medical Conditions Axis 4: Psychosocial and environmental factors Axis 5: Global Assessment of Functioning

9
Schizophrenia Disorder Schizophrenia literal translation “split mind” a group of severe disorders characterized by: disorganized and delusional thinking disturbed perceptions inappropriate emotions and actions

10
Schizophrenia Disorder Delusions false beliefs, often of persecution or grandeur, that may accompany psychotic disorders Hallucinations sensory experiences without sensory stimulation

11
Group of disorders marked by disturbances in thought patterns. These disorders can be accompanied by distortions in perception and abnormal emotional responses. 1% of population in every culture 30% resistant to drugs Gradual vs Sudden onset

12
Paranoid: marked by delusion of persecution and/or grandeur, and frequent auditory hallucinations Disorganized: marked by inappropriate affect, disorganized speech Catatonic: marked by motor disturbances ranging from immobility to excessive, purposeless activity Undifferentiated: mixtures of symptoms from other subtypes

13
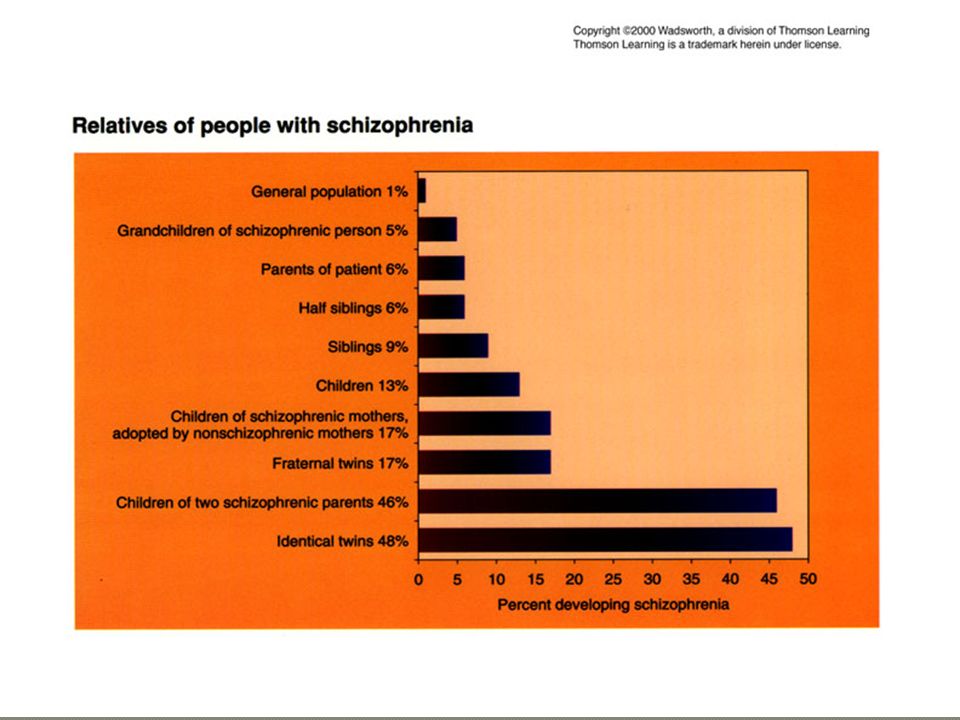
Physiological Explanations neurochemicals-excess dopamine enlargement of the ventricles of the brain genetics-there is a 48% likelihood - identical twins Environmental Explanations Stress can precede the onset of schizophrenia and precede subsequent relapses Unhealthy family dynamics-high expression of emotion and communication difficulties in a family have been associated with the development of schizophrenia

15
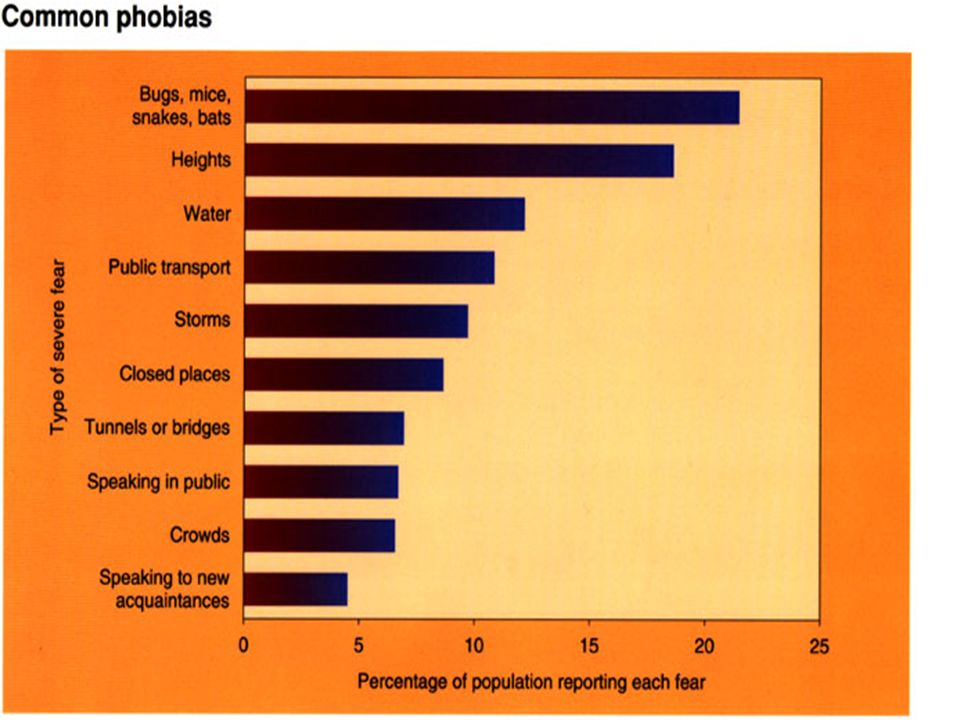
Anxiety Disorders: distressing, persistent anxiety or maladaptive behaviors that reduce anxiety Generalized Anxiety Disorder: chronic anxiety that is not caused by a specific stimulus Panic Attacks: recurrent attacks of anxiety not due to a specific event Phobias: chronic, irrational fear of a specific object or situation Obsessive-Compulsive Disorder: persistent obtrusive thoughts (obsessions) & need to engage in unnecessary rituals (compulsions) Post Traumatic Stress Disorder (PTSD) is a severe anxiety disorder that can develop after exposure to any event that results in psychological trauma. PTSD include re- experiencing the original trauma(s) through flashbacks or nightmares avoidance of stimuli associated with the trauma, and increased arousal – such as difficulty falling or staying asleep, anger.
 through flashbacks or nightmares avoidance of stimuli associated with the trauma, and increased arousal – such as difficulty falling or staying asleep, anger..")
17
Behavioral explanations: Classically conditioned phobic responses Neuro-chemical: decreases in GABA activity and serotonin activity are associated with anxiety disorders Cognitive: people who suffer from anxiety disorders may chronically overestimate the severity of a perceived threat

18
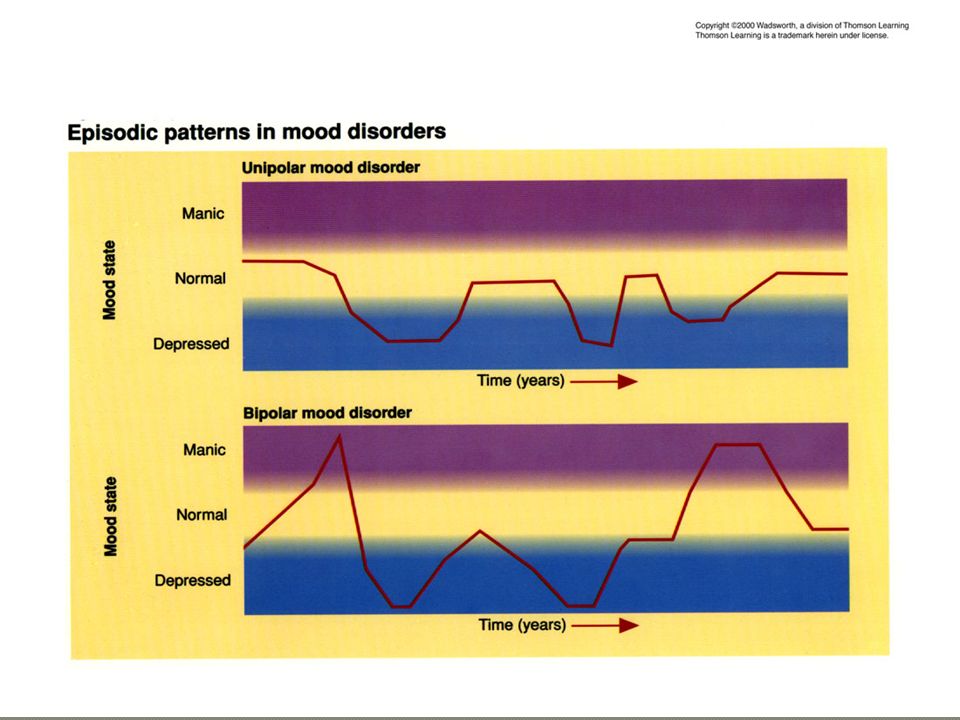
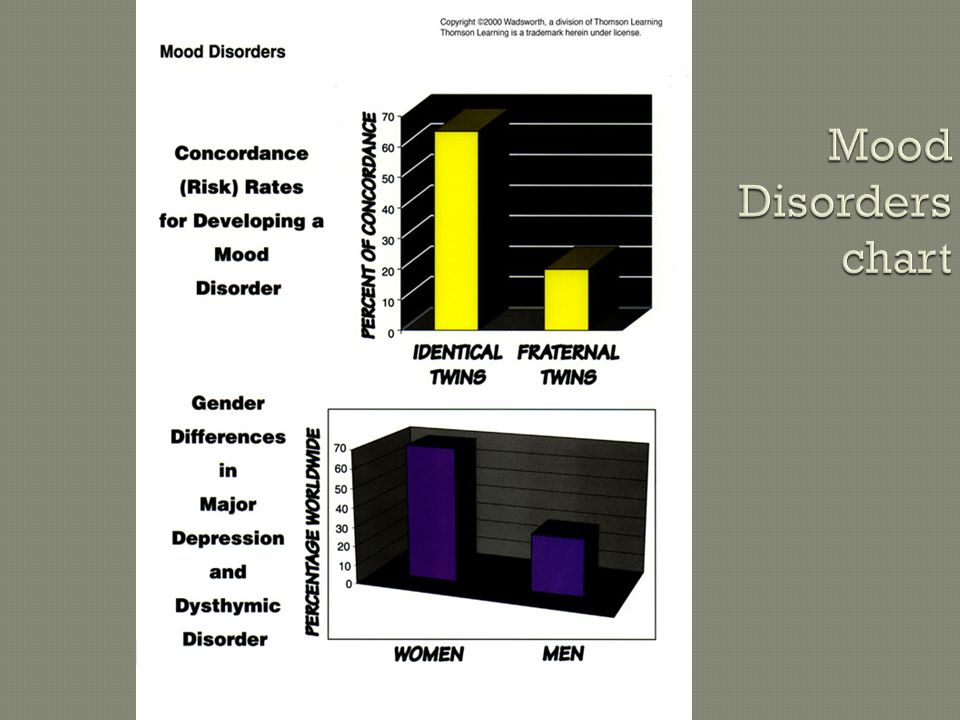
Mood Disorders characterized by emotional extremes Major Depressive Disorder: persistent feelings of sadness and a loss of interest in finding pleasure Bipolar Disorder: marked by chronic experience of manic and depressive episodes formerly called manic-depressive disorder Manic Episode a mood disorder marked by a hyperactive, wildly optimistic state

20
Cognitive and Behavioral Mechanisms Behavioral: ”learned helplessness” believe outcomes in their life are out of their control (external locus of control) Cognitive: negative self-talk is associated with depressive episodes Physiological Mechanisms Neurotransmitters: decreased norepinephrine and serotonin is associated with depression Genetics: there is a 65% concordance rate between identical twins
 Cognitive: negative self-talk is associated with depressive episodes Physiological Mechanisms Neurotransmitters: decreased norepinephrine and serotonin is associated with depression Genetics: there is a 65% concordance rate between identical twins")
22
Personality Disorders Personality Disorders disorders characterized by inflexible and enduring behavior patterns that impair social functioning usually without anxiety, depression, or delusions

23
Personality Disorders PET scans illustrate reduced activation in a murderer’s frontal cortex Normal Murderer

24
Types of Personality Disorders The “Odd” personality disorders: Paranoid: deep distrust, persecution fears Paranoid: deep distrust, persecution fears Schizoid: avoidance of people Schizoid: avoidance of people Schizotypal: discomfort in relationships, odd thinking and behavior patterns Schizotypal: discomfort in relationships, odd thinking and behavior patterns

25
Types of Personality Disorders “Dramatic” Personality Disorders Antisocial Personality Disorder (sociopath): marked by impulsive, callous, manipulative, aggressive, and irresponsible behavior that reflects a failure to accept social norms (often charming) Borderline Personality Disorder: moody, impulsive, manipulative, empty, worthlessness, self-destructive, and fear of abandonment Histrionic: OVERLY emotional/seductive, attention seeking
: marked by impulsive, callous, manipulative, aggressive, and irresponsible behavior that reflects a failure to accept social norms (often charming) Borderline Personality Disorder: moody, impulsive, manipulative, empty, worthlessness, self-destructive, and fear of abandonment Histrionic: OVERLY emotional/seductive, attention seeking")
26
Histrionic Personality Disorder: drama kings and queens, lies, exaggerations Narcissistic Personality Disorder: exaggerated feelings of self-worth and constant need for affirmation Types of Personality Disorders cont…

27
Types of Personality Disorders “Anxious” Personality Disorders Avoidant Personality Disorder: restrained social relationships, inadequacy, sensitive Avoidant Personality Disorder: restrained social relationships, inadequacy, sensitive Dependent Personality Disorder: excessive need to be taken care of, clinging, fearing abandonment Dependent Personality Disorder: excessive need to be taken care of, clinging, fearing abandonment Obsessive-Compulsive Personality Disorder: focus on order, high standards, rigid, stubborn, lack of affection Obsessive-Compulsive Personality Disorder: focus on order, high standards, rigid, stubborn, lack of affection

28
Dissociative Amnesia: sudden loss of memory for personal information that is not due to normal forgetfulness Dissociative Fugue: a loss of memory for their entire lives and sense of identity Multiple-Personality Disorder (DID): the coexistence of more than one personality in an individual Depersonalization: Feelings of unreality concerning the self and environment. Anxiety producing. Many young adults have felt this.

29
Physiological issues without cause Hypochondriasis: excessive preoccupation with becoming ill Conversion Disorder: significant loss of function in one single organ system without a physiological cause

30
Personality Factors: people with histrionic and neurotic personality traits seem to be more susceptible to the somatoform disorders Behavioral Factors: people who have previously received a lot of attention because of illness may begin to find reward in the somatoform disorders

31
Rates of Psychological Disorders

32
Does not know right from wrong A disorder alone does not absolve responsibility

33
Thomas Sasz- no such thing as mental ill Labeling theory Not easy to classify- crossover Infers more understanding than actual

Similar presentations
>")
 Chapter 16 Psychological Disorders James A. McCubbin, PhD Clemson University Worth Publishers.>")











 Chapter 13 Psychological Disorders Modified from: James A. McCubbin, PhD Clemson University Worth Publishers.>")


: Atypical not enough in.>")


