Download presentation
Presentation is loading. Please wait.

1
Large BowelObstruction Dr. Mohammed H. Alarawi Consultant General surgeon Al- Iman General Hospital FRCS, ED – ABCS

2
Anatomy Distal end of Ileum anus (about 1.5 m) Smallest diameter: Sigmoid colon ( where the diverticulosisis most common to form here due to the high pressure especially duringstraining.) Primary function of the large intestine 1. Completion of absorption, esp. final absorption of water 2. Normal flora manufacture certain vitamins (B complex, K) 3. Formation, storage and expulsion of feces
 3. Formation, storage and expulsion of feces.")
3
General characteristics larger internal diameter Presence of epiploic appendices Presence of taeniae coli Presence of the haustra

5
Large bowel obstruction An emergent condition requires early identification and prompt surgical intervention because of the possibility of perforation of the distended or compromised colon with risk of fecal peritonitis.

6
Pathophysiology of LBO LBO can result from either A. Mechanical interruption of the flow of the intestinal contents bowel dilatation above the obstruction mucosal edema + impaired venous drainage and arterial blood flow to the bowel (ischemia) : Mucosal permeability bacterial translocation +systemic toxicity + dehydration + electrolyte abnormalities. Perforation and fecal peritonitis The process is accelerated in closed loop obstruction
 : Mucosal permeability bacterial translocation +systemic toxicity + dehydration + electrolyte abnormalities. Perforation and fecal peritonitis The process is accelerated in closed loop obstruction.")
7
B. Dilatation of the colon without anatomical lesion, as in acute colonic psudo-obstruction (ogilivie’s syndrome) where multiple medical and surgical illness PSY and SY activity loss of peristalsis distention by gas and fluid maximum in the coecum perforation and fecal peritonitis (3-15%)
 where multiple medical and surgical illness PSY and SY activity loss of peristalsis distention by gas and fluid maximum in the coecum perforation and fecal peritonitis (3-15%).")
8
Etiology It is age dependent Prevalence increase with age as does its main causes Neoplasm (benign or malignant) 60% Stricture (diverticular or ischemic) 20% Volvulus (colonic, sigmoid or coecal) 10% Intussusceptions Adynamic ileus, Ogilvie’s syndrome (ACPO)
 60% Stricture (diverticular or ischemic) 20% Volvulus (colonic, sigmoid or coecal) 10% Intussusceptions Adynamic ileus, Ogilvie’s syndrome (ACPO)")
9
Etiology Fecal impaction, foreign body Adhesions Hernia IBD Hirschsprung’s, meconium ileus, imperforate anus

10
Etiology

11
Con’t Neoplasm and diverticular disease: Tumor growth luminal narrowing gradual onset of obstruction. Diverticular disease muscular hypertrophy of the colonic wall with repeated inflammation and fibrosis luminal narrowing

12
Con’t Colonic volvulus: Twisting of the bowel on its mesentery ischemia perforation. 20% of the causes of LBO. A. Sigmoid volvulus: Common in elderly and frail Pt with long h/ o constipation and laxatives Younger Pt can be afflicted in association with high fiber diet. The twist is ante-clockwise B. Coecal volvulus: Less common Clockwise twist

14
Intussusception: Primarily pediatric disease, usually with no leading point. Two third of adult intussusception are caused by tumor Entero-colic Or Colo-colic

15
Con’t Acute colonic P.obstruction (Ogilivie’s syndrome): Functional obstruction. Elderly debilitated patients caused by medical (infections, Cardiac disease) or trauma (operative, non operative).
 or trauma (operative, non operative)..")
16
Clinical presentation Complaints suggesting LBO Constipation Abdominal distention Crampy abdominal pain Nausea and Vomiting Symptoms suggestive of peritonitis Fistula (passage of air, mucus or feces in the urine)
")
17
Con’t Assessment of symptoms should attempt to distinguish the following: Acute Vs acute on chronic obstruction onset, H/o bowel movement, stool caliber, recurrent LLQ pain and weight loss Complete Vs partial obstruction By symptoms and rectal examination

18
Con’t Mechanical Vs functional obstruction (illeus or Ogilvie’s syndrome) In ACPO, symptoms develop over 1-2 days up to 1 week, distention is early sign, fever is a bad sign Intussusception Recurrent, intermittent colicky pain relevied by fetal position with weight loss and fatigability
 In ACPO, symptoms develop over 1-2 days up to 1 week, distention is early sign, fever is a bad sign Intussusception Recurrent, intermittent colicky pain relevied by fetal position with weight loss and fatigability")
19
Physical examination Although a complete examination is necessary it should emphasize on the following: Abdomen (inspection, auscultation, percussion, palpation) Inguinal and femoral region Rectum
 Inguinal and femoral region Rectum")
20
Laboratory investigation CBC Serum chemistry Serum lactate Coagulation profile Stool for Occult blood

21
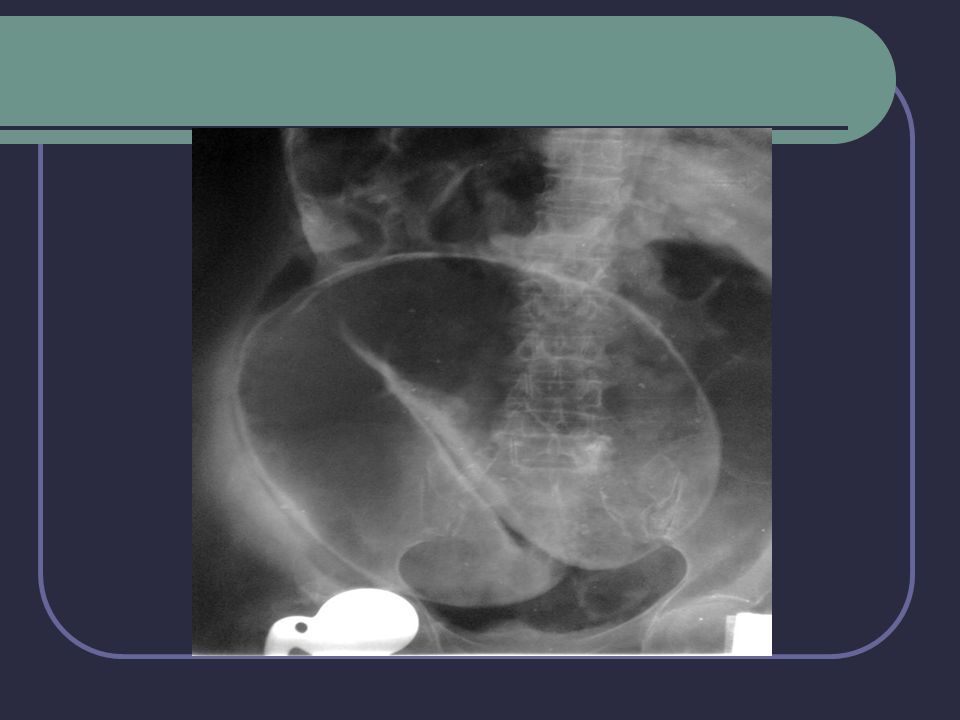
Imaging modalities Plain radiograph chest and abdomen (flat and upright)
")
23
Con’t Contrast radiography with enema

24
Contrast enhanced CT Can distinguish between partial and complete obstruction and site of obstruction Gastrographine (water soluble contrast) should be used esp if bowel perforation is suspected.
 should be used esp if bowel perforation is suspected.")
25
Management Initial therapy include: Correction of fluid and electrolytes imbalance with fluid monitoring Bowel rest NGT Appropriate preoperative antibiotic Specific management: Illeus: Tx of the underlying disorder Cessation of drugs slowing colonic motility

26
ACPO (ogilivie’s syndrome) If no perforation conservative Tx and management of the underlying disorder for 24hr. If failed, consider neostigmine or colonic decompression (success rate 80%) If perforation or if conservative Tx failed surgical intervention with high mortality and morbidity. Volvulus: Sigmoiod volvulus: Sigmoidoscopy and deflation with flatus tube followed by later elective surgery. If failed, urgent laparotomy, un-twisting of the loop and per anal decompression followed by either fixation of the sigmoid loop “if viable” or resection (Paul-mikulicz procedure, sigmoid colectomy with anastomosis or Hartmann’s procedure.
 If perforation or if conservative Tx failed surgical intervention with high mortality and morbidity. Volvulus: Sigmoiod volvulus: Sigmoidoscopy and deflation with flatus tube followed by later elective surgery. If failed, urgent laparotomy, un-twisting of the loop and per anal decompression followed by either fixation of the sigmoid loop if viable or resection (Paul-mikulicz procedure, sigmoid colectomy with anastomosis or Hartmann’s procedure..")
28
Con’t Coecal or transverse colon volvulus: Volvuls should be reduced followed by either fixation (caecopixy) and, or caecostomy. If the cecum is ischemic or gangrenous right hemicolectomy. Intussusception: if no peritonitis contrast enema (barium or air) success rate in child >in adults. If failed or with signs of peritonitis surgery Surgery is indicated in adult intussusception why? Recurrence rate is 3% after contrast and 1%after surgery.
 success rate in child >in adults. If failed or with signs of peritonitis surgery Surgery is indicated in adult intussusception why. Recurrence rate is 3% after contrast and 1%after surgery..")
29
Colonic masses and strictures: Endoscopic dilatation and stenting of obstructed colon: palliative for high risk patients with unresctable tumor preparation for surgery: Relieve the acute stage Allow time for ressuscitation and bowel preparation Surgery Right colon resection with anastomosis Left colon resection without anastomosis or resection with intra- operative lavage and anastomosis Diverticular disease: Conservative followed by elective surgery If failed surgery (same principles of Ca tx)
")
30
Prognosis Depends on: Patient’s factors Underlying disease Management timing and procedures Development of complications Mortality rate: mechanical obstruction 20%-40% (with perforation) ACPO 15%-36% (with ischemia or perforation)
 ACPO 15%-36% (with ischemia or perforation)")
31
Colostomies

32
Colostomy Colostomy refers to a surgical procedure where a portion of the large intestine is brought through the abdominal wall to carry stool out of the body. It may be permanent or temporary.

33
Indications in Adults Colorectal ca Colonic Obstruction Traumatic perineal injury Colonic,High anal Fistulae Protect a distal anastom Diverticular disease Ischemia IBD

34
Indications in children Hirschsprung disease Meconium ileus Imperforate anus Complex hindgut anomalies Volvulus Trauma

35
End colostomy The working end is brought through the abdomen to the skin surface after the damaged section of the bowel is removed End colostomy can be temporary to allow bowel rest or healing, such as following tumor resection, traumatic injury to the colon, or inflammation of the bowel. End colostomy can be permanent when the distal colon is reseceted or unresectable Hartmann procedure involves leaving the distal portion of the colon in place, which is closed to create a Hartmann’s pouch.

36
Loop colostomy A loop of the bowel is brought through the abdomen to the skin surface and temporarily supported by a plastic bridge or rod. A communicating wall remains between the proximal and the distal bowel. Can be created in transverse colon (transverse loop colostomy) or in sigmoid colon (sigmoid loop colostomy) Is typically created as an emergency procedure to relieve an intestinal obstruction or perforation. May be opened at the time of surgery or a few days later. It has two openings through the stoma – the proximal end drains stool while the distal portion drains mucus. Loop colostomies are typically temporary.
 or in sigmoid colon (sigmoid loop colostomy) Is typically created as an emergency procedure to relieve an intestinal obstruction or perforation. May be opened at the time of surgery or a few days later. It has two openings through the stoma – the proximal end drains stool while the distal portion drains mucus. Loop colostomies are typically temporary..")
38
Double-barrel colostomy Both ends of the bowel are brought through the abdomen to the skin surface as two separate sections. The proximal stoma (colostomy), diverts feces through the abdominal wall. The distal stoma (mucous fistula), expels mucus from the distal colon A double-barrel colostomy may be created because of trauma, tumors, or inflammation, and it may be temporary or permanent.
, diverts feces through the abdominal wall. The distal stoma (mucous fistula), expels mucus from the distal colon A double-barrel colostomy may be created because of trauma, tumors, or inflammation, and it may be temporary or permanent..")
39
Complications Excessive bleeding Ischemic stoma Surgical wound infection Retraction Prolapse Stenosis Parastomal hernia

40
Thank You ! The End

Similar presentations