Download presentation
Presentation is loading. Please wait.

1
Disorders of pigmentation

2
Hypopigmentation. Hyperpigmentation.

3
Color of the skin Melanin Oxyhemoglobin (in blood) Deoxyhemoglobin
 Deoxyhemoglobin")
4
Melanin is produced from tyrosine from the action of tyrosinase. two forms of melanin are produced :eumelanin and phaeomelanin by melanocytes (synthesised by melanosomes ). transfered to adjacent keratinocytes (phagocytosis ).
. transfered to adjacent keratinocytes (phagocytosis )..")
5
Influence on melanin synthesis: Skin color UV radiation Hormonal (melanocyte stimulating hormone by pitutary gland)
")
6
Abnormal skin pigments

7
Heterotopic Calcification Exogenous Endogenous dust heavy metals & drugs introduced from outside body produced within the body miscellaneous lipofuscin Pigmentation melanin = = haemoglobin breakdown HaemosiderinHaematinBilirubinHaemotoidinPorphyrins hypercarotinaemia pigments in skin (e.g. tatoos)
.")
8
Disorders of Melanin Pigmentation hyperpigmentation ↑ Melanin Production: Epidermal Increased menanocyte no. Lentigins Malignant melanoma Increased activity Endocrine Disease Freckles UV PUVA Pregnancy Dermal Mongolian spots Postinflammatory hypopigmentation ↓ Melanin Production: Anatomical defect in melanocytes Vitiligo Piebaldism Chemicals Postinflammatory Functional defect (defect in tyrosine mech.) Pityriasis versicolor Endocrine disorders Albinism
 Pityriasis versicolor Endocrine disorders Albinism.")
9
Causes of hypopigmentation Genetic: albinism,phenylketonuria,tuberous sclerosis. Infection : yaws,leprosy,pityriasis versicolor. Postinflamatory: cryotherapy,psoriasis, pityriasis alba. Hormonal : hypopituitarism. Others: vitiligo,lichen sclerosis,halo naevi.

10
Causes of hyperpigmentation Endocrinal :chloasma,cushing’s syndrome,addison’s diseases. Genetic: racial freckles, peutz jegher syndrome, neurofibromatosis. Metabolic :biliary cirrhosis,porphyrias,haemochromatosis. Nutritional:carotenemia,pellagra,malnutrional, malabsorption. Drugs:psoralen,oestrogen,minoxidil. Post inflammatory:lichen planus,eczema,lichen sclerosis.

11
Vitiligo Definition: Acquired idiopathic leucoderma Aetiology: 1.Autoimmune theory. 2.Self destruction theory. 3.Neural theory. 4.Genetic theory

12
Neural theory Patients afflicted with a nerve injury who also have vitiligo have hypopigmentation or depigmentation in denervated areas. Additionally, segmental vitiligo frequently occurs in a dermatomal pattern, which suggests that certain chemical mediators are released from nerve endings that affect melanin production. Further, sweating and vasoconstriction are increased in depigmented patches of vitiligo, implying an increase in adrenergic activity. Finally, increased urinary excretion of homovanillic acid and vanilmandelic acid (neurometabolites) has been documented in patients with vitiligo.
 has been documented in patients with vitiligo..")
13
Intrinsic defect of melanocytes Vitiligo melanocytes may have an intrinsic defect leading to melanocyte death. These melanocytes demonstrate various abnormalities, including abnormal, rough endoplasmic reticulum and incompetent synthesis and processing of melanocytes.

14
Genetics of vitiligo Human leukocyte antigens (HLAs) may be associated, An association with HLA-B13 is described in the presence of antithyroid antibodies. Inheritence is polygenic 20-30% gives a family history

15
Autoimmune destruction of melanocytes Hashimoto thyroiditis Graves disease; other endocrinopathies, such as Addison disease and diabetes mellitus; alopecia areata; pernicious anemia; inflammatory bowel disease; psoriasis; and autoimmune polyglandular syndrome are all associated with vitiligo. antibody to melanocytes Histopath. Demonstrates lymphocytes in early lesion

16
Vitiligo (cont.) Precipitating factors: 1.Emotional stress. 2.Sun burn. 3.Physical trauma. (Koebner’s phenomenon)
.")
17
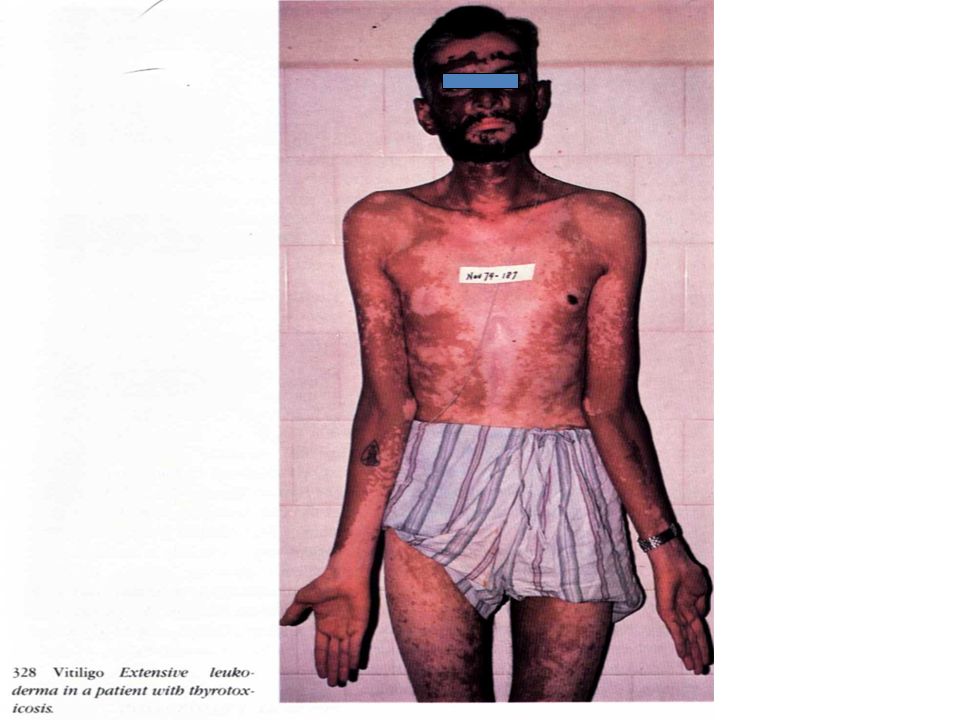
Morphology of the lesion Milky White macule which is sharply defined are often symmetrical. Sites :hand, wrists,knees,neck,and around the orifices :eg mouth Course is unpredictable :may remain static,may progress or repigment. Equal sex incidence M=F Affect any races Age on onset is between 10-30 years.

18
patterns: I-Localized a- Focal. b- Segmental. II- Generalized: a- Acrofacial. b- Vulgaris. III- Universal

19
Body hair (leukotrichia) in vitiliginous macules may be depigmented. Scalp involvement is the most frequent, followed by involvement of the eyebrows, pubic hair, and axillary hair, respectively. Leukotrichia may indicate a poor prognosis in regard to repigmentation. Spontaneous repigmentation of depigmented hair in vitiligo does not occur.

20
During medical therapy, pigment cells arise and proliferate from the following 3 sources: The pilosebaceous unit, which provides the highest number of cells, migrating from the external root sheath toward the epidermis Spared epidermal melanocytes not affected during depigmentation The border of lesions, migrating up to 2-4 mm from the edge

21
Vitiligo

23
Vitiligo vulgaris

24
Focal vitiligo

25
Segmental vitiligo

26
Universal vitiligo

27
D.D.: 1.Albinism. 2.Pityriasis versicolour 3.Post inflammatory. hypopigmentation. 4.Chemical depigmentation.

28
Treatment: I- Localized: a- Topical PUVA. b- Topical corticosteroids. c- Topical covermark creams.

29
Vitiligo (cont.) Treatment: (cont) I- Generalized: a- Systemic PUVA.
 Treatment: (cont) I- Generalized: a- Systemic PUVA.")
30
Vitiligo (cont.) Treatment: (cont) I- Universal: Depigmentation of the normally pigmented areas. Monobenzyl ether of hydroquinone.

31
Surgical Care dermoepidermal grafts epidermal grafting Cultured epidermis with melanocytes or cultured melancyte suspensions

Similar presentations



 and neck 2 yrs. Along with this, he also complained of eructation.>")








 die or stop.>")






