Download presentation
Presentation is loading. Please wait.

1
Dr Samal Nauhria samal@windsor .edu
Plasma cell lesions Dr Samal Nauhria .edu

2
Plasma Cell Lesions Multiple Myeloma Solitary Plasmacytoma/myeloma.
Lympho-plasmacytic Lymphoma Heavy-chain Disease Primary Amyloidosis MGUS

4
Multiple Myeloma Median age at diagnosis - 70 years
M/C in males and in people of African origin Principally involves bone marrow and associated with lytic lesions throughout the skeletal system Evidence of end-organ damage includes Calcium elevation, Renal insufficiency, Anemia, and Bone lesions (CRAB)
")
5
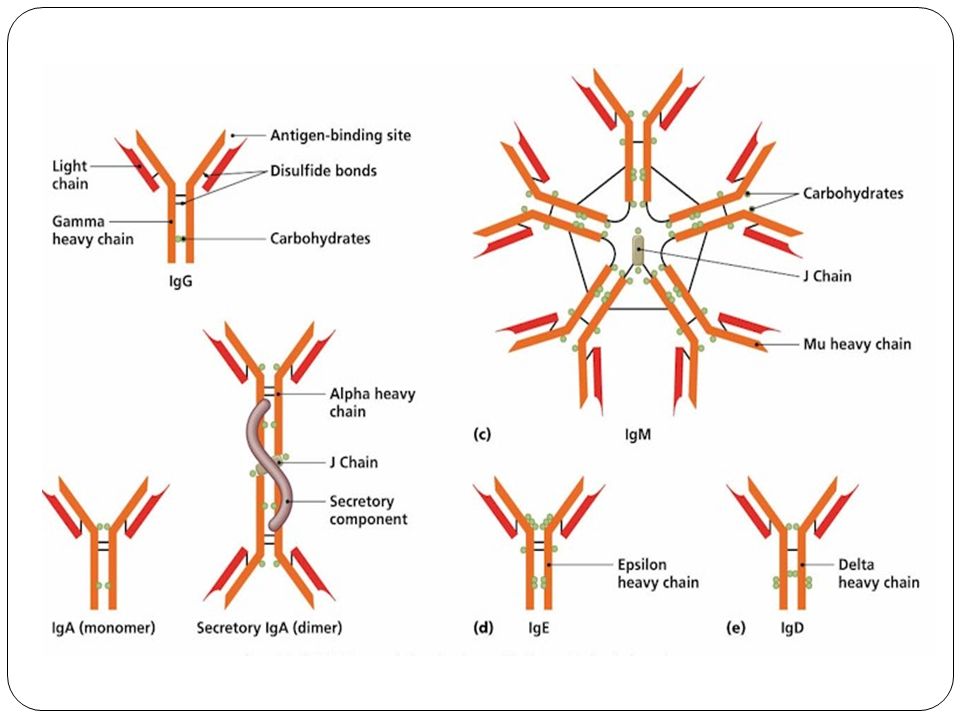
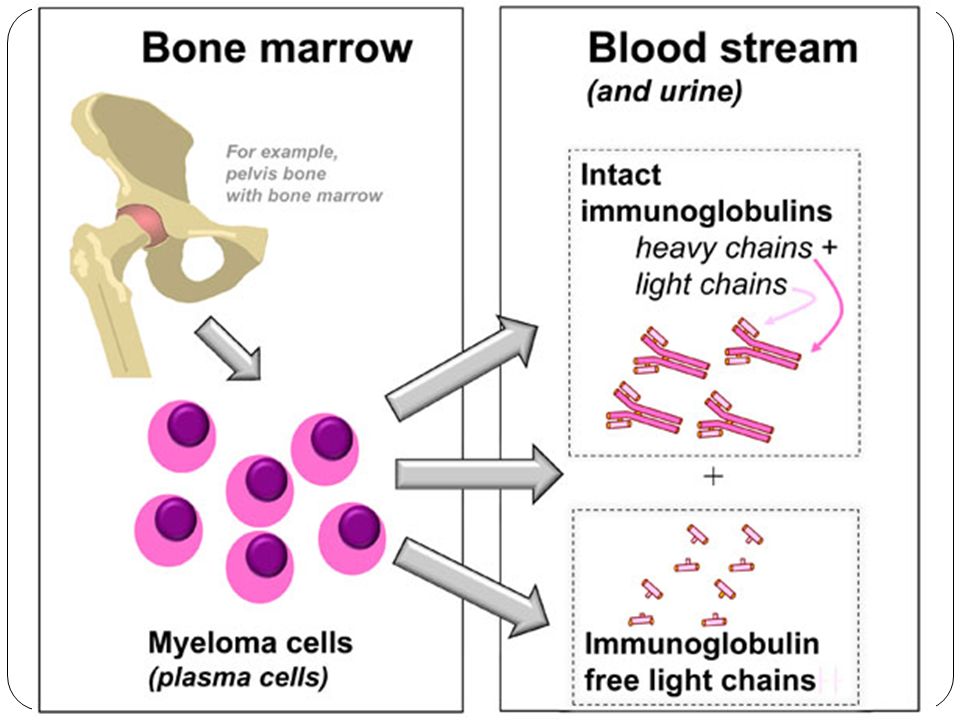
Multiple Myeloma Most frequent M protein is IgG (60%), followed by IgA (20% to 25%) In 15 to 20% cases, the plasma cells produce only κ or λ light chains Bence-Jones proteins: free κ or λ light chains that are excreted in the urine

7
Pathogenesis of Myeloma
Dysregulation of D cyclins is common IL-6 produced by fibroblasts, macrophages in the bone marrow stroma stimulates proliferation of myeloma cells Myeloma Cells secrete IL-1β, TNF, IL-6 which stimulate production of RANK-ligand increased osteoclast bone resorption

8
Pathogenesis of Myeloma
Immunosuppression: Although plasma contains increased Ig’s owing to M protein, the levels of functional antibodies are profoundly depressed, leaving patients at high risk for bacterial infections

9
Morphology Multifocal destructive skeletal lesions,
most commonly involving the VERTEBRAL COLUMN, ribs, skull, pelvis, femur, clavicle, and scapula Punched-out defects 1 to 4 cm in diameter Arise in medullary cavityerode cancellous bone progressively destroy the cortical bone Pathologic fractures, mostly in vertebra or femur

10
Multiple myeloma with multiple vertebral fractures at the thoracic and lumbar levels

11
Microscopic examination
Increased numbers of plasma cells > 30% of the cellularity Abnormal features Prominent nucleoli Abnormal cytoplasmic inclusions(Ig) In terminal stages, a leukemic picture may emerge
 In terminal stages, a leukemic picture may emerge.")
12
PLASMA CELLS Terminally differentiated B-cells
Not normally found in peripheral blood Account for < 3.5% of nucleated cells in the bone marrow

13
Oval cells with cart-wheel nucleus
Cytoplasm is basophilic blue Nucleus is oval or round and typically placed eccentrically A hof is present adjacent to the nucleus contains Golgi apparatus

14
RUSSELL BODIES Globules (2-3 μm) of accumulated immunoglobulins in the cytoplasm of plasma cells Usually round May be found in normal bone marrow 1st described by William Russell

15
MOTT CELLS/MORULA CELLS
Plasma cells crowded with Russell bodies An obstruction blocks the release of Golgi secretions These cells can be found in any case of chronic plasmacytosis

16
FLAME CELLS Eosinophilic torn cytoplasm
Usually associated with IgA myeloma

17
DUTCHER BODIES Immunoglobulin filled cytoplasm invaginating into the nucleus creating the appearance of an intranuclear inclusion PAS +ve Identified by Dutcher and Fahey

18
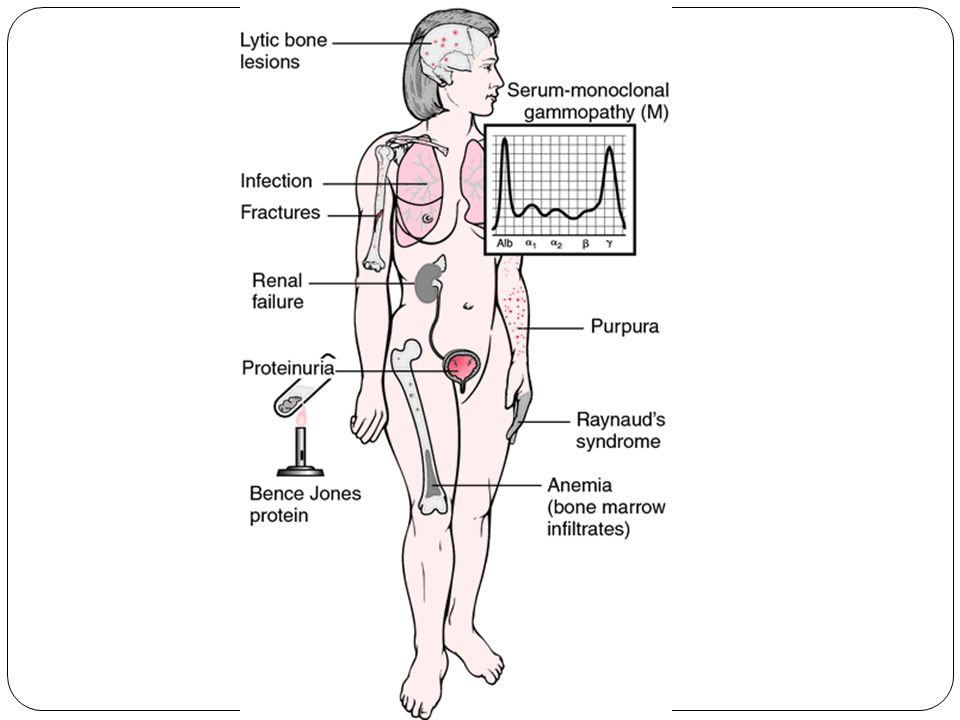
Clinical Features Pathologic fractures Bone Pain Vertebral fracture may lead to spinal cord impingement Hypercalcemia from bone resorption Neurologic manifestations (confusion, lethargy) Renal dysfunction Symptoms related to hyperviscosity Anemia: due to marrow replacement by tumor cells and suppression of hematopoiesis Recurrent infections with bacteria Common cause of death**
 Renal dysfunction. Symptoms related to hyperviscosity. Anemia: due to marrow replacement by tumor cells and suppression of hematopoiesis. Recurrent infections with bacteria. Common cause of death**")
19
Renal findings Renal insufficiency (in 50% of patients)
Proteinaceous tubular casts Casts are composed of BJ protein, which is nephrotoxic and damages tubular epithelium Biopsy reveals an intratubular multinucleated giant cell reaction Nephrocalcinosis Hypercalcemia leads to metastatic calcification of the tubular basement membranes in the collecting ducts Calcium deposits are a common cause of acute renal failure in multiple myeloma AL-type amyloidosis (5% to 10% of patients)
")
21
Diagnosis Clinically suspected when focal, punched-out skeletal defects are present - especially in vertebrae Electrophoresis of the serum and urine - monoclonal complete Ig or monoclonal free Ig light chain Examination of bone marrow: to confirm plasma cell proliferation

22
SERUM PROTEIN ELECTROPHORESIS
Useful in quantitating the M protein and shows a monoclonal spike Does not specify which M protein is increased (e.g., IgG, IgA, IgM)
")
23
Other Tests- Serum immunofixation electrophoresis
Provides a characterization of the M protein (heavy and light chain subclass; e.g., IgGκ or IgGλ; IgMκ or IgMλ) Urine protein electrophoresis Identifies BJ protein (free light chains) and quantitates the amount of light chains in the urine But not specify whether the light chains are κ or λ Urine immunofixation electrophoresis Characterizes whether BJ protein is κ or λ Serum for free light chains Detects and quantitates κ and λ light chains in serum More sensitive for detecting light chains than any of the urine methodologies listed above
 Urine protein electrophoresis. Identifies BJ protein (free light chains) and quantitates the amount of light chains in the urine. But not specify whether the light chains are κ or λ. Urine immunofixation electrophoresis. Characterizes whether BJ protein is κ or λ. Serum for free light chains. Detects and quantitates κ and λ light chains in serum. More sensitive for detecting light chains than any of the urine methodologies listed above.")
24
Treatment and Prognosis
Progressive disease, median survival of around 4 to 6 years Not curable Autologous stem cell transplantation - dramatically improved survival New therapies Proteasome inhibitors (induce plasma cell apoptosis) Thalidomide analogues (alter the marrow microenvironment to inhibit myeloma cell growth and survival)
 Thalidomide analogues (alter the marrow microenvironment to inhibit myeloma cell growth and survival)")
25
Solitary Plasmacytoma/myeloma
Low or no serum and urine M protein No malignant plasma cells in the bone marrow Skeletal Plasmacytoma Occurs in same locations as multiple myeloma Progresses to full-blown multiple myeloma over 5 to 10 years Soft tissue Plasmacytoma Most often in upper respiratory tract Spreads infrequently, cured by local resection

26
Lymphoplasmacytic Lymphoma (Waldenström macroglobulinemia)
Affects older persons; peak incidence between 6 -7th decades Tumor cells secrete an M protein (commonly IgM) Mixture of B cells ranging from small lymphocytes to plasmacytic lymphocytes to plasma cells Involves lymph nodes, bone marrow, and spleen at presentation
 Mixture of B cells ranging from small lymphocytes to plasmacytic lymphocytes to plasma cells. Involves lymph nodes, bone marrow, and spleen at presentation.")
27
Lymphoplasmacytic Lymphoma
↑IgM causes viscous blood - Waldenström Macroglobulinemia No free light chains or Bence Jones proteinuria No lytic bone lesions Renal disease and amyloidosis are rare

28
Waldenström Macroglobulinemia
Visual impairment: tortuosity and distention of retinal veins; retinal hemorrhages and exudates Neurologic problems - headaches, dizziness, tinnitus, deafness, and stupor, (from sluggish blood flow and sludging) Bleeding - formation of complexes between macroglobulins and clotting factors as well as interference with platelet function Cryoglobulinemia - precipitation of macroglobulins at low temperatures - Raynaud phenomenon and cold urticaria
 Bleeding - formation of complexes between macroglobulins and clotting factors as well as interference with platelet function. Cryoglobulinemia - precipitation of macroglobulins at low temperatures - Raynaud phenomenon and cold urticaria.")
29
Heavy-Chain Disease Proliferations in which only heavy chains are produced IgA heavy-chain disease: more common, has a predilection for lymphoid tissues in which IgA normally is produced (Small intestine, Respiratory tract) IgG heavy-chain disease: diffuse lymphadenopathy and hepatosplenomegaly
 IgG heavy-chain disease: diffuse lymphadenopathy and hepatosplenomegaly.")
30
Primary Amyloidosis Monoclonal proliferation of plasma cells that secrete free light chains underlies primary amyloidosis Amyloid deposits (AL type) consist of partially degraded light chains
 consist of partially degraded light chains.")
31
Monoclonal Gammopathy of Undetermined Significance(MGUS)
Asymptomatic monoclonal gammopathy Serum M proteins in 1 to 3% of healthy persons > 50 years < 3 g/dL of monoclonal protein in serum No Bence Jones proteinuria Precursor lesion with a tendency to evolve to multiple myeloma (rate of 1% per year) Diagnosis made only after careful exclusion of other monoclonal gammopathies, particularly multiple myeloma The clonal plasma cells in MGUS contain the same chromosomal translocations found in full-blown multiple myeloma
 Diagnosis made only after careful exclusion of other monoclonal gammopathies, particularly multiple myeloma. The clonal plasma cells in MGUS contain the same chromosomal translocations found in full-blown multiple myeloma.")
Similar presentations
 – A NEW APPROCH AND OUR EXPERIENCE Kamenetsky Natalya (1), Rachmilewitz Eliezer.>")






 Idiopathic Associated with other diseases (autoimmune, infectious, non-heme.>")








>")

BB Topic 3 Autoimmunity Part 8 Immunoproliferative Diseases.>")
