Download presentation
Presentation is loading. Please wait.

1
The role of vitamin B12 within the body
Ahmad Sh. Silmi Msc Haematology, FIBMS

2
Vitamin B12

3
The role of vitamin B12 within the body
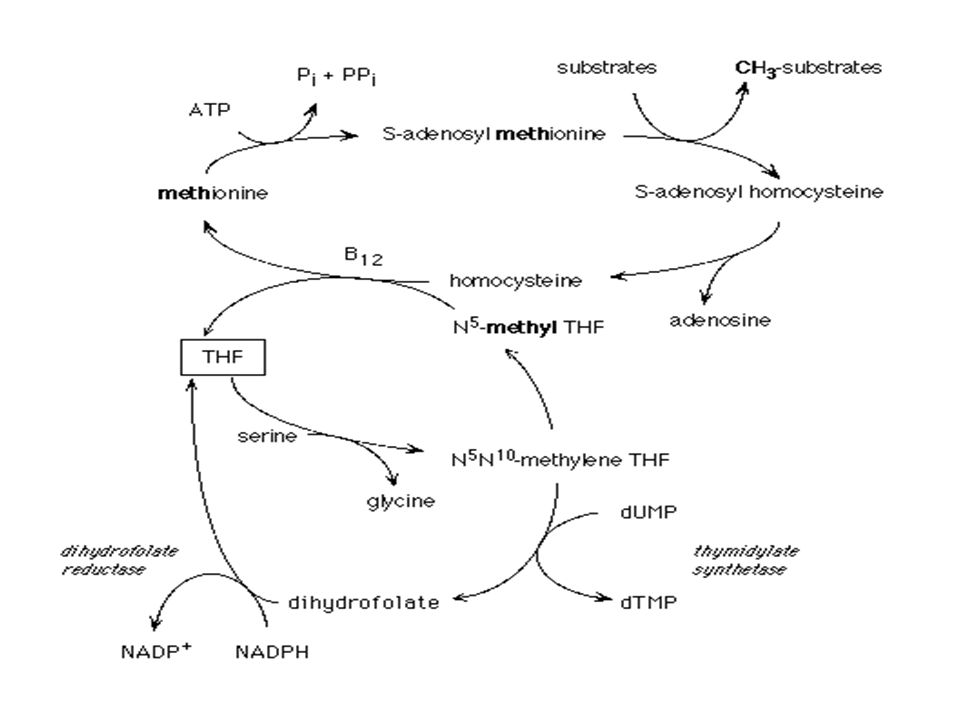
Vitamin B12 is required as coenzyme for two metabolic reaction: (1) Isomerization of L-methylmalonyl CoA to succinyl CoA. This is important substrate in Hb synthesis. (2) Methylation of homocystine to methionine. This step is important in intracellular synthesis of folate coenzyme.
 Isomerization of L-methylmalonyl CoA to succinyl CoA. This is important substrate in Hb synthesis. (2) Methylation of homocystine to methionine. This step is important in intracellular synthesis of folate coenzyme.")
4
COBALAMIN REACTIONS Methylmalonyl CoA Succinyl CoA Homocysteine
Methionine Methyl Cobalamin Adenosyl Cobalamin THF N H N H CH3 Succinyl CoA

5
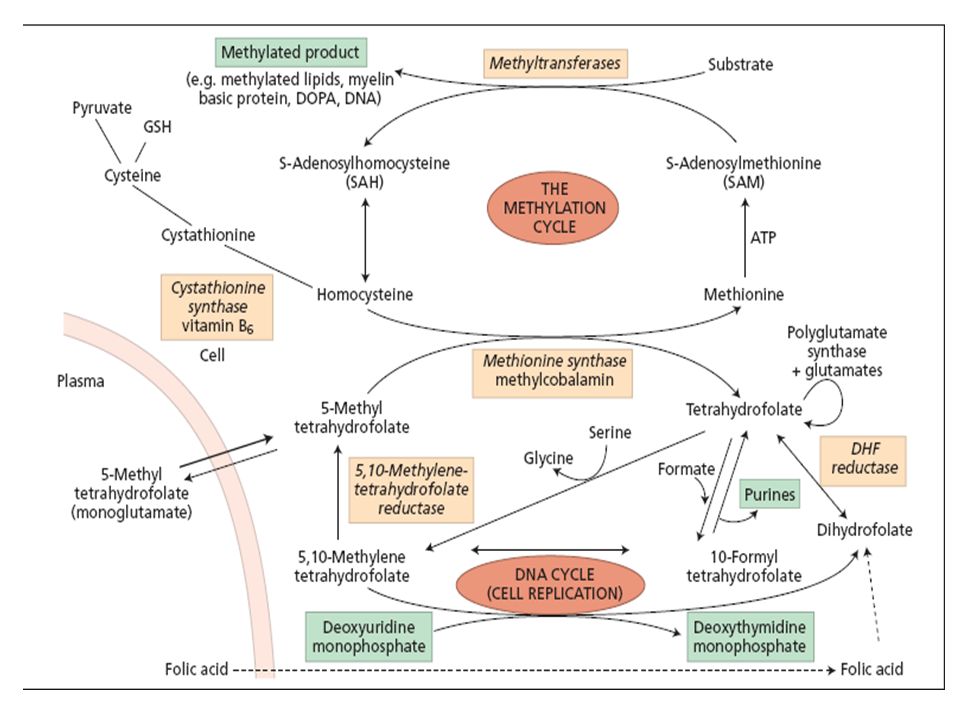
Folate/B12 DNA Synthesis

6
Daily vitamin B12 requirement
The only source available to man is dietary. The main dietary source is liver, kidney, red meat, eggs, shellfish and dairy products. Normal mixed diet contains 5-30 μg /day. Vitamin B12 is relatively stable and little is lost during cooking. Typical daily losses of vitamin B12 are between 1-4 μg. The vitamin is lost mainly in urine and faeces. Since normally there is no consumption of vitamin B12 within the body, the daily requirement matches daily losses.

7
Vitamin B12 Stores Normal body stores of vitamin B12 about 3-4 mg, primarily in liver. This would be sufficient for 3 years if dietary intake ceased or if the ability to absorb the vitamin was lost.

8
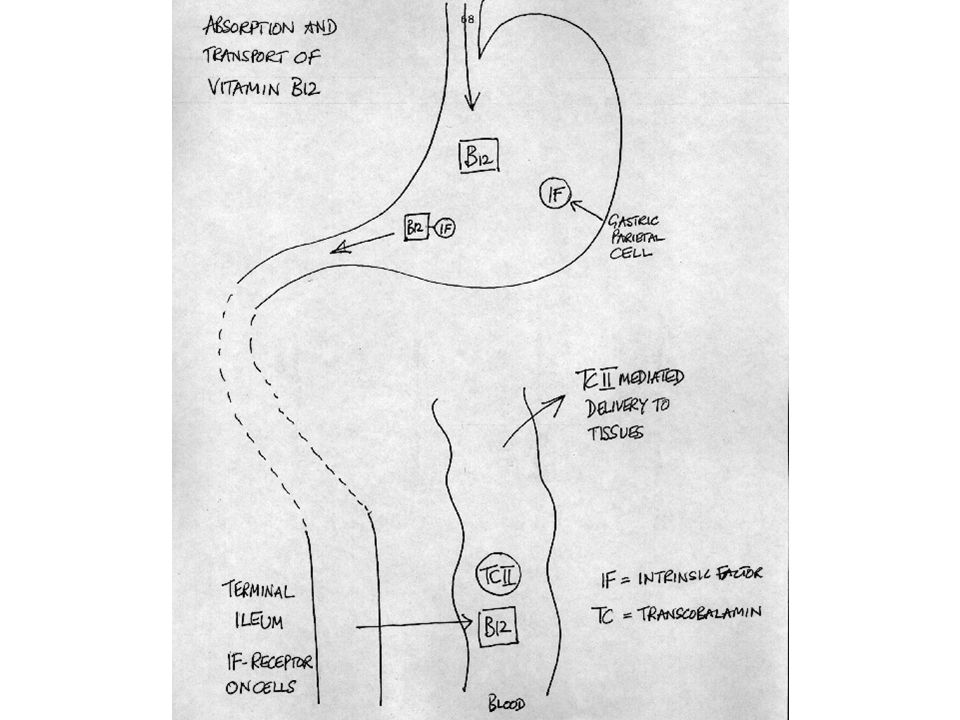
Vitamin B12 absorption VitaminB12 absorption is an active process, which occurs in the ileum. Vitamin B12 is liberated from food by gastric and duodenal enzymes and complexes in a 1:1 ratio with the intrinsic factor. IF is a glycoproein, MW 45,ooo, which is synthesized and secreted by gastric parietal cells. IF: B12 complex then progresses to the ileum where it attaches to specific receptors on the ileal mucosal cells. This process requires the presence of calcium ions and neutral pH. The vitamin is internalized from the complex and released into the portal circulation after 6 hours.

9
(a) Intrinsic factor; (b) intrinsic factor–cobalamin complex.
 Intrinsic factor; (b) intrinsic factor–cobalamin complex.")
10
Vitamin B12 Transport There are three vitamin B12 transport proteins normally present in the plasma, which are known as Transcobalamines (TCI-TCII-TCIII). The physiologically active is TCII which complex in a 1:1 ratio with vitamin B12. The complex is then binds to specific surface receptors on developing blood cells in the bone marrow. Vitamin B12 is then released by hydrolysis. The TCII is not reutilized. The plasma half-life of TCII is 12 hours and congenital absence of it causes megaloblastic anaemia within weeks of birth. Transcobalamines I and III are -globulins synthesized by granulocytes and known as R-binders that are found in a wide range of body fluids. TCI&III do not readily release vitamin B12 to the developing tissues. The plasma half-life is 9-12 days and congenital absence of them causes no physiological impairment.
. The physiologically active is TCII which complex in a 1:1 ratio with vitamin B12. The complex is then binds to specific surface receptors on developing blood cells in the bone marrow. Vitamin B12 is then released by hydrolysis. The TCII is not reutilized. The plasma half-life of TCII is 12 hours and congenital absence of it causes megaloblastic anaemia within weeks of birth. Transcobalamines I and III are -globulins synthesized by granulocytes and known as R-binders that are found in a wide range of body fluids. TCI&III do not readily release vitamin B12 to the developing tissues. The plasma half-life is 9-12 days and congenital absence of them causes no physiological impairment.")
12
GI ABSORPTION OF COBALAMIN
IF R Cbl R-Cbl IF-Cbl TCII TCII-Cbl Stomach Duodenum Terminal Ileum TCI-Cbl

13
Folates

14
Folates The parent of folate family compounds is folic acid which has the following basic structure. Humans are incapable to synthesize it so the only source is diet. Folic Acid

15
The role of folate within the body
The various form of folate function as a single-carbon donor-acceptors in a variety of biosynthetic reactions as shown below: Synthesis of methionine. By donation of methyle group from N-5-methyl-tetrahydrofolate and requires vitamin B12 as a coenzyme. Pyrimidine synthesis which is a rate limiting step in DNA synthesis. Purine synthesis. Conversion of serine into glycin. Histidine catabolism.

18
Daily folate requirement and storage
Daily folate losses are about 100 g per day, mainly in the faeces, urine, and sweat and skin cells. Faeces contain large amount of vitamin B12 and folic acid, but these are due to the microbial flora activities rather than losses from body stores. In order to maintain body stores, the total daily requirement must match losses. Thus, the normal adult daily requirement for folate is about 100 g. Folate is present mainly in liver, leafy vegetables, whole grains and yeast. Folate is extremely sensitive to heat. Cooking involves prolonged boiling result in sever loss.

19
Daily folate requirement and storage
Normal mixed diet may contain as much as 700 g of folate per day but improper food preparation can reduce this amount close to the minimum daily requirement. Typical body stores of folate in a normal, healthy adult are about 10mg and are located in liver. Thus, if dietary folate intake or intestinal absorption ceased, the body stores would become exhausted in about 3-4 months.

20
Folate absorption and transport
Folates are absorbed maximally from the upper jejunum. Folate polyglutate must be digested to form monoglutamate before absorption. Absorbed folates are converted into N-5-methyltetrahydrofolate and released into portal blood stream. Plasma folates circulate freely or loosely bound to a variety of specific plasma proteins. There is some evidence that a specific folate transport protein exists and that its concentration is increased by folate deficiency but its physiological significance is unknown.

21
FOLATE/COBALAMIN Properties

22
Megaloblastic Anaemia
Megaloblastic anemia is referred to a group of panhypoplastic disorders, which are characterized by retardation of DNA synthesis but RNA synthesis proceeds at a normal rate. The resulting asynchrony between nuclear and cytoplasm maturation in developing cells is responsible for the distinctive morphological and biochemical features of the megaloblastic anaemias.

23
Megaloblastic Anaemias Causes
Deficiency of either vitamin B12 or folic acid or sometimes both. A number of uncommon exceptions exist where the cause of the disorder is not attributable to haematinic deficiency.

24
Causes of Vitamin B12 Deficiency
1- Inadequate dietary intake. 2- Intestinal malabsorption. 3- Increased requirements, which cannot be met from the diet. 4- Failure of utilization of absorbed vitamin.

25
Inadequate Dietary Intake
This is uncommon for three main reasons: 1- Vitamin B12 is present in a wide range of readily available foodstuffs. 2- Vitamin B12 is relatively heat-stable. 3- Body stores of vitamin B12 are sufficient to meet the requirements for at least three years following complete cessation of dietary intake or intestinal absorption.

26
Malabsorption of vitamin B12
The most common cause of the deficiency, which could be due to: Lack of intrinsic factor Gastrointestinal disease. Drug-induced Malabsorption.

27
1- Lack of intrinsic factor (pernicious anaemia)
Pernicious anemia is by far the most common cause of B12 deficiency. This condition is especially common among the elderly, with an observed prevalence of up to 1.9%. The disease is more common in women than in men and is associated with blood group A.

28
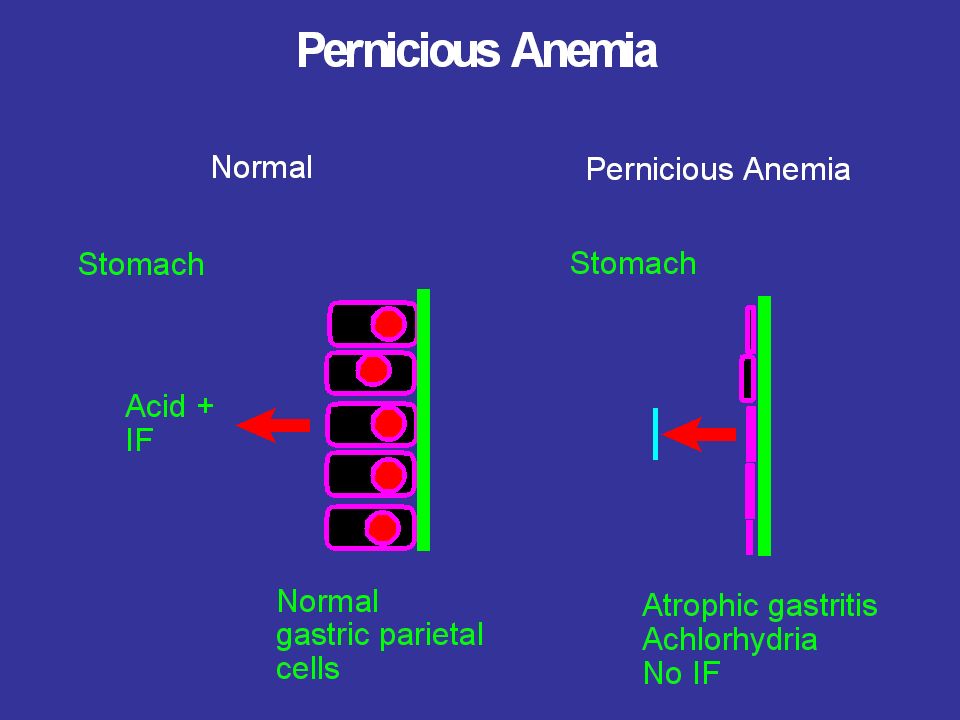
pernicious anaemia Pernicious anemia is caused by intestinal malabsorption due to atrophy of the gastric mucosa and decreased secretion of intrinsic factor. One recent hypothesis suggests an autoimmune mechanism, as illustrated by a case of spontaneous remission of pernicious anemia after corticosteroid therapy. The question of a relationship between pernicious anemia and Helicobacter pylori has also been investigated, but evidence for this theory has not been conclusive.

29
pernicious anaemia About 90% of patients have cytotoxic IgG directed against gastric parietal cells or intrinsic factor demonstrated in serum. In about 75% of these the antibody is demonstrated in gastric juice. Polyclonal IgG or IgA are demonstrated in serum and gastric juice in 50% of patients with pernicious anaemia, this acts in one of two ways: Either prevents the binding of vitamin B12 to intrinsic factor. OR inhibit the absorption of VitB12-IF complex.

30
pernicious anaemia Pernicious anaemia is associated with an increased incidence with congenital deficiency of autoimmune thyriod disease, rheumatoid arthritis and gastric carcinoma. A rare type of pernicious anaemia is associated with congenital deficiency of intrinsic factor or the synthesis of dysfunctional variant of intrinsic factor.

32
Diagnosis of Pernicious Anemia
The diagnosis is achieved by Schilling test as: Failure to absorb radiolabelled B12 on the initial assay, followed by absorption when B12 is co-administered with intrinsic factor, establishes the diagnosis.

33
Treatment of Pernicious Anemia
It consists of intramuscular injections of 1000 mcg of vitamin B12 at weekly intervals until B12 stores are replenished, followed by monthly injections for life. Oral and intranasal preparations of B12 have been tried but without compelling success.

34
2- Gastrointestinal Disease
The most obvious follows surgical removal of the source of intrinsic factor, or the site of absorption of the vitamin. a) Total gastrectomy: the anaemia is developed after depletion of the body stores, which is usually, occur within 5 years. This is sever when accompanied with iron deficiency anaemia. b) Partial gastrectomy: (stagnant or blind loop syndrome) Partial removal of the stomach, and refashioning the junction with the gut. The sterile duodenal part will colonized with bacteria, which will consume huge amount of the vitamin. c) Ileal resection or ileostomy: Involve removal of the vitB12 receptor.
 Total gastrectomy: the anaemia is developed after depletion of the body stores, which is usually, occur within 5 years. This is sever when accompanied with iron deficiency anaemia. b) Partial gastrectomy: (stagnant or blind loop syndrome) Partial removal of the stomach, and refashioning the junction with the gut. The sterile duodenal part will colonized with bacteria, which will consume huge amount of the vitamin. c) Ileal resection or ileostomy: Involve removal of the vitB12 receptor.")
35
Gastrointestinal Disease
d) Crohn's disease: Granulomatous disease, which most commonly affects the terminal ileum and the ascending colon. It's manifested by generalized Malabsorption of nutrients from the diet. e) Infestation of the gut with the fish tapeworm Diphyllobothrium lattum, which is capable of extracting substantial quantities of vitamin B12 both complexed with intrinsic factor and free.
 Crohn s disease: Granulomatous disease, which most commonly affects the terminal ileum and the ascending colon. It s manifested by generalized Malabsorption of nutrients from the diet. e) Infestation of the gut with the fish tapeworm. Diphyllobothrium lattum, which is capable of extracting substantial quantities of vitamin B12 both complexed with intrinsic factor and free.")
36
3- Drug-induced Malabsorption
A number of drugs have been reported to impair vitamin B12 absorption such as: Anticonvulsant, phenytoin Antimicrobial, neomycin Antigout, colchicine Alcohol.

37
Increased Requirements
The requirements are increased during pregnancy. The increase is not sufficient to cause deficiency unless the pregnant was previously borderline body stores of the vitamin.

38
Failure of Vitamin B12 Transport
Congenital deficiency of transcobalamin II develops megaloblastic anaemia in the first weeks of life, despite the presence of normal vitamin B12 concentration in the serum. Early diagnosis prevents neurological damages

39
Failure of Vitamin B12 Metabolism
Rare number of congenital failure to convert the absorbed vitamin B12 to it's active coenzyme forms have been described, resulting in the excretion of methylmalonic acid and homocystine in the urine. These patients are mentally retarded, but for unknown reasons, rarely develop megaloblastic anaemia. Anaesthetic nitrous oxide inactivates vitamin B12 coenzymes and induces megaloblastic changes & mild neuropathy.

40
Folic acid deficiency Causes:
Deficiency of folic acid can result from an 1- inadequate diet. 2- intestinal malabsorption. 3- increased requirement. 4- failure of utilization the absorbed vitamin.

41
Inadequate dietary Intake
This is common for 3 main reasons: The ideal diet contains 700 g of folate of which about half is absorbed. b) Folate is very labile to heat; cooking can destroy up to 90% of folate in it. c) Body stores are only sufficient for 3 months when dietary intake stop.
 Folate is very labile to heat; cooking can destroy up to 90% of folate in it. c) Body stores are only sufficient for 3 months when dietary intake stop.")
42
Malabsorption This can be due to several conditions like:
Coelic disease: villous atrophy, which decreases iron and folate absorption. Tropical sprue: similar to coelic disease. Crohn disease: generalized malabsorption in the intestine.

43
Increased requirements
This most commonly seen in: Pregnancy: the daily requirement for folate can rise to 500μg in the 3ed trimester of pregnancy. More than 60% of pregnant women have subnormal folate concentration. This recently, demonstrated to be associated with neural tube defects. Prophylactic folic acid therapy is recommended several months before conception.

44
Increased requirements
The anaemia of chronic haemolytic conditions such as sickle cell anaemia frequently is exacerbated by folate deficiency. Sever haemolytic conditions increases the rate of haemopoiesis by a factor of 10, which cannot be met by dietary sources.

45
Drug-induced folate deficiency
Some drugs are demonstrated to inhibit folate absorption such as: Long-term therapy with anticonvulsant, phenyton. Alcohol The cytotoxic drugs methotrexate, which inhibit the enzyme dihydrofolate reducates and cause depletion of thymidin and purine nucleotides.

46
Failure of folate metabolism
A number of rare enzyme deficiencies have been reported which cause impairment of folate metabolism. Most of these are associated with megaloblastic changes and mental retardation.

47
Pathophysiology Patients with megaloblastic anemia typically display :
pallor, weakness, shortness of breath, and congestive heart failure. In some cases, loss of appetite, weight loss and gastrointestinal disturbances. In addition to these non-specific changes, a range of signs which are specific to megaloblastic patients, such as those affecting tissue, where the tissue divide most rapidly associated with impaired mitotic function and premature cell death. These can be described under three headings:

48
General tissue manifestations
Deficiency of vitamin B12 or folic acid affects all dividing cells but the effects are manifest most clearly in rapidly dividing tissues such as bone marrow and epithelial cells. Disturbances in the epithelial cells causes: 1- Angular stomatitis (lesions at the corner of the mouth) 2- Glossitis (inflammation of the tongue)
 2- Glossitis (inflammation of the tongue)")
49
Neurological manifestations
Degeneration of the dorsal and lateral columns of the spinal cord are typical findings in sever megaloblastic anemia due to deficiency of vitamin B12. The mechanism is not known yet. Folic acid deficiency in pregnancy is associated with the incidence of neural tube defects such as spina bifida and is also believed to lead to mild dementia and impairment of intellectual function.

50
Haematological manifestations
The megaloblastic bone marrow is hypercellular, with an increased in erythropoietic activity. There is immature forms of all cell lines, and premature death of cells in the process of development. This is known as ineffective haemopoiesis, and responsible for the pancytopenia, which characterizes this condition. The increased cell turnover leads to increase in the concentration of unconjugated bilirubin, LDH and lysozyme. Peripheral blood shows macrocytosis and the presence of the late megaloblast. Reticulocytopenia is present. Megaloblastic leucopoiesis is reflected by the appearance of bizarre, giant metamylocyte in the bone marrow, and an increased in the circulating hypersegmented granulocytes. Morphological changes in megaloblastic megakaryocytes include an increase in cell size and failure of cytoplasmic granulation. However, these changes often are indistinct.

51
Summary

52
All you need to know is contained in the following list
Vitamin B12 and folate All you need to know is contained in the following list

53
Both vitamin B12 and folate deficiency cause an identical megaloblastic anemia
Vitamin B12 deficiency causes demyelination in the spinal cord and peripheral nerves It takes about 3 months to run out of folic acid, and 3 years to run out of vitamin B12 Folate is in meat and vegetables (foliage) and is absorbed from the jejunum Vitamin B12 is only in foods of animal origin; its absorption from the terminal ileum requires a specific binding protein called intrinsic factor Folate deficiency results from poor diet, malabsorption or increased requirements Vitamin B12 deficiency is commonly the result of Pernicious Anemia Pernicious Anemia results from an autoimmune attack on gastric parietal cells causing achlorhydria and Intrinsic Factor deficiency Low vitamin B12 levels are common in the elderly and usually do not cause anemia: they should be managed with oral vitamin B12 replacement Deficiency of vitamin B12 and folic acid can be diagnosed by measuring serum levels; homocysteine and methylmalonic acid levels may help Folate can be replaced orally. Vitamin B12 is traditionally given parenterally, but high dose oral therapy also works for Pernicious Anemia Increasing dietary folate intake in a population lowers its average level of serum homocysteine: the daily dose for a maximum effect is 400 mcg Neural tube defects can be prevented by using folate supplements in women intending to become pregnant
 and is absorbed from the jejunum. Vitamin B12 is only in foods of animal origin; its absorption from the terminal ileum requires a specific binding protein called intrinsic factor. Folate deficiency results from poor diet, malabsorption or increased requirements. Vitamin B12 deficiency is commonly the result of Pernicious Anemia. Pernicious Anemia results from an autoimmune attack on gastric parietal cells causing achlorhydria and Intrinsic Factor deficiency. Low vitamin B12 levels are common in the elderly and usually do not cause anemia: they should be managed with oral vitamin B12 replacement. Deficiency of vitamin B12 and folic acid can be diagnosed by measuring serum levels; homocysteine and methylmalonic acid levels may help. Folate can be replaced orally. Vitamin B12 is traditionally given parenterally, but high dose oral therapy also works for Pernicious Anemia. Increasing dietary folate intake in a population lowers its average level of serum homocysteine: the daily dose for a maximum effect is 400 mcg. Neural tube defects can be prevented by using folate supplements in women intending to become pregnant.")
54
Practical approach to Macrocytosis
History for alcohol, liver CBC and blood film for evidence of marrow disease Reticulocyte count B12/Folate levels Liver function, TSH Bone marrow exam if cause in doubt and you really want to know

55
MCV Low Hb=Anemia Low=microcytic High=macrocytic Normal=normocytic
Ferritin Measure B12 + folate Fe deficient Fe normal Normal Low - Establish cause Establish cause Obvious cause Cause not obvious Consider bone marrow Anemia of chronic disease or hemoglobinopathy Reticulocyte count Hemolysis or blood loss low Anemia of chronic disease Renal failure Marrow failure high

56
Normal

57
oval macrocytes

58
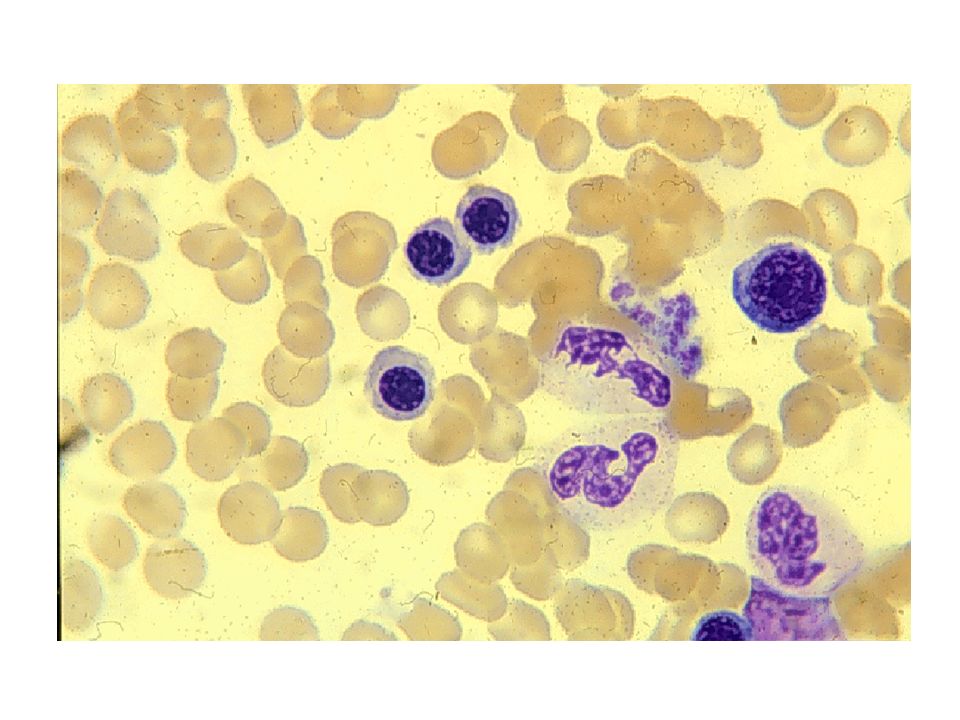
hypersegmented polymorph

60
Normal marrow cells

61
Megaloblastic marrow cells

62
Megaloblastic marrow cells
giant metamyelocyte

63
Vitamin B12 deficiency causes demyelination in the spinal cord and peripheral nerves

Similar presentations











i.>")







