Download presentation
Presentation is loading. Please wait.

1
Speech and Language Therapy in Dementia and Palliative Care
Aideen Lawlor SLT Manager Dublin North City and County- North West Dublin and St. Mary’s hospital Phoenix Park

2
Content of talk How dementia impacts on the communication skills of people with dementia What strategies and tools can help when communicating with people with dementia The role of the Speech and Language Therapist in dementia and palliative care Managing swallowing problems for people with dementia including ethical decisions around swallowing problems

3
Communication and Ageing
Hearing and visual difficulties (Presbyacusis) 35% of UK over 65 pop have a hearing loss sufficient to affect daily living 40% of people prescribed a hearing aid do not use it Changes in attention and memory Motor slowing (facial and respiratory musculature) Dentition and saliva production Drug side effects Reduced communication network
 35% of UK over 65 pop have a hearing loss sufficient to affect daily living. 40% of people prescribed a hearing aid do not use it Changes in attention and memory. Motor slowing (facial and respiratory musculature) Dentition and saliva production. Drug side effects. Reduced communication network.")
4
Communication in older people
Difficulty processing speech structures that rely on working memory, this can include recalling recent events, particularly involving time and place. This may also bias the most recently presented choice. Priming effects may have more impact on older person so providing choice of answers may influence responses. Repetition of information may result in that information being viewed more favourably.

5
Tips for enhancing communication
Normal prosody (intonation, timing and stress) assist rapid detection of linguistic structure. Exaggerated prosody should be avoided. Pausing at natural processing points (sentences/clauses) allows additional time for speech processing.
 assist rapid detection of linguistic structure. Exaggerated prosody should be avoided. Pausing at natural processing points (sentences/clauses) allows additional time for speech processing.")
6
Language characteristics of Alzheimer’s Disease
In Alzheimer’s Disease at mild-moderate stage, semantic system is inaccessible rather than degraded Inconsistencies appear- output versus input tasks Picture versus word recognition tasks Generative naming across time- modality differences- written versus verbal comprehension

7
Late stages of Alzheimer’s Disease
Turn taking preserved Some preservation of appropriate use of language in every day context, greetings, mealtimes Listeners can facilitate ‘conversational’ exchanges

8
Emerging view of dementia
Different disease patterns, Individual variation--Don’t assume input and output the same Drug therapy arresting the decline Preservation of underlying knowledge Person centred approach to dementia Interpersonal communication skills still prevalent at advanced stages of dementia

9
How we communicate? Tone Body Language Words we say

10
The person with Dementia
words Tone Body Language

11
The person with Dementia
“The Person with dementia “sometimes seem to have a heightened awareness of body language, and often their main meanings may be conveyed nonverbally. In the case of those who are very severely impaired in cognition, it seems probable that the words and the sentences are at times more of an accompaniment or adornment than the vehicle for carrying the significant message.” Kitwood 2000

12
Model for intervention
Environment Individual needs remaining skills Focus on

13
Role of SLT with dementia and communication
Early: Convey information for specific circumstances Mid: Increase reliance on printed material Later: Teach communication partners to offer basic choices Activity and engagement materials such as life stories

14
Tools to aid communication
Picture/text based communication aids, notebooks, maps, objects iPad and other high tech tools Use photos to develop ‘little stories’ or themes to develop a life story book

15
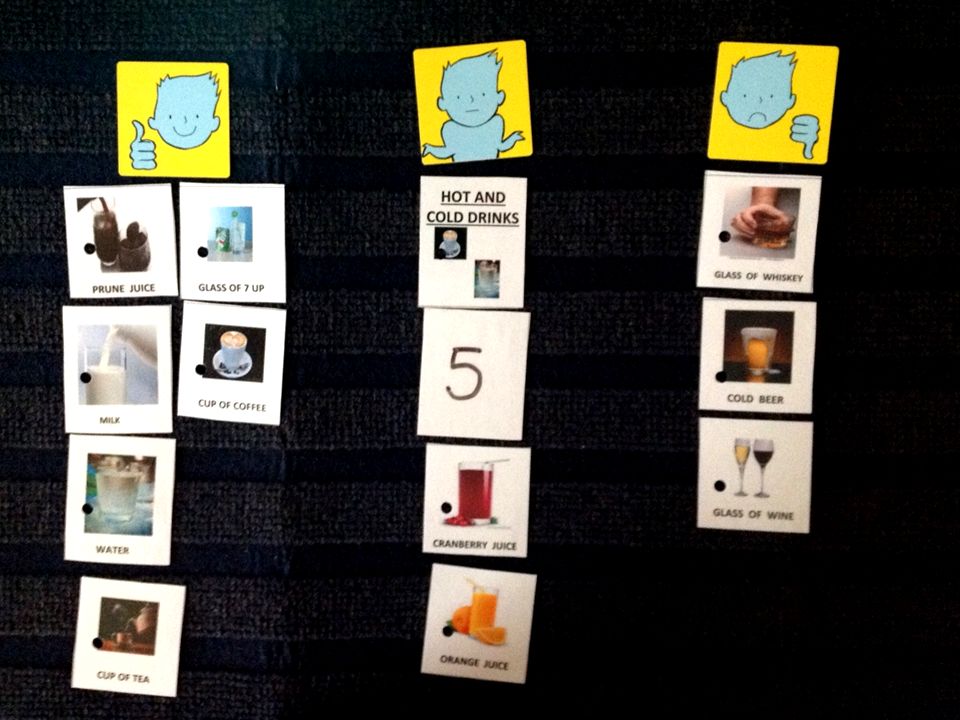
Communication Strategies
Love it Ok Hate it For example: Question - Would you like the priest to come and visit you? Would you like that to happen now?

16
Example of talking board
I don’t watch it I like it Christmas TV Talk Shows Crime Soaps Funny Sound of Music Late Late Show Quincy Coronation Street Interesting Gone With The Wind Parkinson Murder She Wrote Emmerdale Exciting Late Late Toy Show Afternoon Show Midsummer Murders Eastenders Boring White Christmas Richard & Judy Touch of Frost Fair City Silly I I watch it I don’t like it

18
Eating and drinking in the older person
malnourishment in the older patient slower swallow reduced isometric tongue pressure reduced smell and tactile sensitivity altered dentition reduced taste acuity accurate diagnosis of swallow impairment is essential

19
Eating and drinking problems in dementia
Visual agnosia Distractibility Eating apraxia Tactile agnosia for food Apraxia of swallow Delayed pharyngeal swallow Impaired pharyngeal swallow

20
Management of swallowing disorders in dementia
Manipulation of surroundings Compensatory strategies More frequent, smaller meals

21
Palliative care and dementia
Palliative care should not only be considered as having a role at end-of-life, but that it starts from point of diagnosis through the journey of the illness, to end-of-life and bereavement support for family members. FINAL.pdf?ext=.pdf

22
Planning Palliative Care in Dementia
People with dementia receive less pain relief and fewer medical services at end of life Decisions around end of life care often occur as a result of a medical crisis Advance care planning discussion can reduce unnecessary treatments and admissions to hospital at the end of life.

23
Key outcomes from Scotland’s National Dementia Strategy
More people with dementia and their families and carers being involved as equal partners in care throughout the journey of the illness Better respect and promotion of rights in all setting, together with improved compliance with the legal requirements in respect of treatment People with dementia in hospitals or other institutional settings always being treated with dignity and respect

24
SLT in dementia and palliative care
Professional Carers will never fully understand the light and shade, the hope and despair, and the frustration and joy of each family member’s relationship with a person who has dementia. The best that they can do is to develop, in partnership with families, a mutually agreed plan that includes the very best physical care, thoughtful and sensitive social support and emotional and spiritual space for each unique passing. Hudson (2003)
")
25
Barriers to palliative care for people with dementia
Dementia not always seen as a life limiting illness Communication around preference and wishes often left too late Dementia can cause death but it is not generally recorded as the primary cause of death (O’ Shea 2008) Difficult to identify the final phase of dementia. Few palliative care staff have education in dementia care and dementia care staff have little education in palliative care
 Difficult to identify the final phase of dementia. Few palliative care staff have education in dementia care and dementia care staff have little education in palliative care.")
26
Recognising when someone is dying with(or from) dementia
where the person is non-ambulatory has lost meaningful conversation is dependent for most activities of daily living weight loss of 10% recurrent infections multiple pressure sores hip fracture pneumonia in advanced dementia No longer meeting full nutritional requirements orally (Gold Standard Framework UK 2006)
")
27
Dehydration It is assumed that dehydration and starvation can cause a painful death. Data from hospice caregivers indicates that dry mouth, thirst, and increased secretions in dying patients were unrelated to their level of hydration. (Slomka 2005)
")
28
Dehydration “Nothing would be more tiresome than eating and drinking if [they were not] a pleasure as well as a necessity.” Voltaire When food and fluids are not desired by dying clients, administering them does not add to client comfort. Dehydration can aid the dying process by inducing fatigue.
![Dehydration Nothing would be more tiresome than eating and drinking if [they were not] a pleasure as well as a necessity. Voltaire.](http://slideplayer.com/slide/10059655/32/images/28/Dehydration+Nothing+would+be+more+tiresome+than+eating+and+drinking+if+%5Bthey+were+not%5D+a+pleasure+as+well+as+a+necessity.+Voltaire..jpg "When food and fluids are not desired by dying clients, administering them does not add to client comfort. Dehydration can aid the dying process by inducing fatigue.")
29
Role of SLT in dementia and palliative care
Parallels the role of all HSCP in palliative care Maintain and improve quality of life Optimize pts ability to express needs and concerns Affirm that reduced intake is due to declining clinical status-not the reverse (J Pall Med 7(5)) Appropriate management of eating and swallowing is integral to a comprehensive End of Life approach (Smith et al 2009). Professional Carers will never fully understand the light and shade, the hope and despair, and the frustration and joy of each family member’s relationship with a person who has dementia. The best that they can do is to develop, in partnership with families, a mutually agreed plan that includes the very best physical care, thoughtful and sensitive social support and emotional and spiritual space for each unique passing. Hudson (2003)
) Appropriate management of eating and swallowing is integral to a comprehensive End of Life approach (Smith et al 2009). Professional Carers will never fully understand the light and shade, the hope and despair, and the frustration and joy of each family member’s relationship with a person who has dementia. The best that they can do is to develop, in partnership with families, a mutually agreed plan that includes the very best physical care, thoughtful and sensitive social support and emotional and spiritual space for each unique passing. Hudson (2003)")
30
Role of SLT in eating and drinking problems associated with dementia and palliative care
1.Social e.g. embarrassment at mealtimes 2.Cultural e.g. Christmas dinner, birthday cake, jelly and ice cream 3.Religious e.g. taking communion Family members e.g. fear about starvation, frustration and anger and conflict. The focus is on minimising symptoms and maximising individual comfort.

31
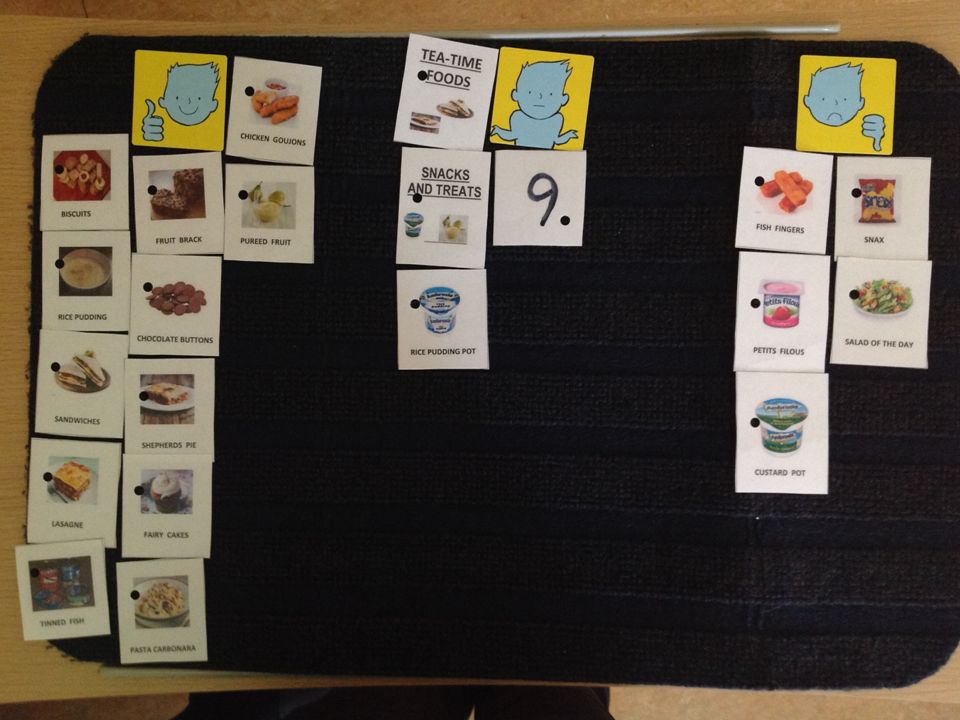
Example of approach to finding out patient preference
Preparatory stage: Care plan review Medical chart review: Communication review: Food and drink preferences and dislikes: review from multiple perspectives Staff questionnaires: Family questionnaires: Talking mats: Staff observation exercise:

34
Observation tools Food+Drinks preferences/ Dislikes G – Gesture;
V- Vocalisation; FE – Facial Expression; SL –Sleepy; Y/N – Response to yes/ no question C - Comment; Req - Request

35
Observation by staff; Daily Sheet Resident _______________; MRN_____
Date: ______; Signed: ________________ Breakfast Non-verbal G V FE SL Verbal Y/N C Req like OK Dislike Comment: Lunch + Dessert Comment Tea Snacks/ Treats

36
What might help with eating and drinking problems?
New seating Changing position Having more time Adapted cutlery Special cup Using a straw distractions Naso-gastric tube PEG Pureed food Timing of medication Extra nourishment Tablets in syrup form Avoiding difficult food Small meals Soft moist food Thickened drinks

38
Decision making for end of life
‘stealing’ high risk foods ‘best interest decision making’ meeting Not up to the carer/family, medical team have the ultimate say ‘ability to make decisions for yourself.’ Understand and Retain information long enough to make a decision People have the right to make an unwise decision weigh up all risks

40
Refusal of thickened fluids

41
Refusal of thickened fluids
Assessment of swallow function reveal X is at risk of aspiration on all consistencies particularly on large amounts of free fluids, however given current behaviours (physically declining thickened fluids), X is to take free fluids when sitting out in the chair and when alert and with close supervision of trained staff/carer (Lyndsey Collins 2013)
, X is to take free fluids when sitting out in the chair and when alert and with close supervision of trained staff/carer (Lyndsey Collins 2013)")
42
Case study- journey through dementia
3 years of decline needed Grade 3 and pureed diet to avoid LRTIs Wouldn’t accept assistive feeding and demonstrated preference for liquids Took grade 1 fluids (mainly milk) until end of life Met family, discussed NPO option after severe LRTI but agreeable to remain on oral diet and fluids.
 until end of life. Met family, discussed NPO option after severe LRTI but agreeable to remain on oral diet and fluids.")
43
Case Study-journey through dementia
Admitted to residential unit at Middle stage of dementia- was non verbal Took Full Pureed diet and grade 3 fluids for 3 years Ate only tspns of pureed as tolerated for another 18 months Needed to adapt mealtimes according to levels of alertness

44
Managing dysphagia in dementia- a timed snack protocol? – Boczko, 2004
2 pilot studies aimed at improving nutritional status and encouraging weight gain in patients with dysphagia and dementia MDT team involved include SLT, Clinical nutrition, nursing staff and catering staff. 1.residents' self-feeding leads to their increased awareness of food 2. snacks based on residents' preferences (e.g., for sweet or spicy foods) are better tolerated 3.consumption of discrete, small amounts of food may serve to satisfy appetite without overloading the system
 are better tolerated. 3.consumption of discrete, small amounts of food may serve to satisfy appetite without overloading the system.")
45
Method handheld, highly spiced or sweetened snacks treated as a "medication protocol" to ensure both regular delivery and consumption, for example, pureed salami and pickle on small pieces of bread

46
Method Group 1(6 clients)- take a snack three times a day, two hours after their main meals, as part of medication regieme Group 2(6 clients)- Snacks recommended however not included in medication regieme
- Snacks recommended however not included in medication regieme.")
47
Findings of study Group 1- 4 residents gained weight, 1 maintained weight and 1 lost weight Group 2- 4 residents actually never received the snacks, 3 of those residents lost weight.

49
‘When we are faced with tough management decisions related to end stage dementia that we should seek a Hospice consult which provides support for the family and critical documentation to address "comfort" issues. This individual will have an expected weight loss and staff need to be reassured that to "offer" food and liquid is the expectation. The definition of offer is NOT forced feeding. I view my role as a supportive professional who validates the HCA that it’s okay to attempt to feed, terminate the meal, provide oral care, report it to the charge nurse and know you’ve done the job expected. HCAs believe if they don't complete the meal with adequate intake that they’ve failed. These are random thoughts based on 13 years of dealing with the issue on a daily basis.’ Paula Leslie 2012

50
Dementia and palliative care
The last part of life may have importance out of all proportion to its length” Dame Cicely Saunders, 1990.

51
references Abbey,J (2006) Palliative Care and Dementia. Queensland University Brisbane Hughes, J. C. (2006) Palliative Care in Severe Dementia, Quay Books, London. Pollens R. (2004)Role of the speech-language pathologist in palliative hospice care Journal of Palliative Medicine. 7 (5) (pp ), Sullivan RJ. Accepting death without artificial nutrition or hydration. J Gen Intern Med 1993; 8:220–224. Royal College of Physicians and British Society of Gastroenterology (2010) Oral feeding difficulties and dilemmas: A guide to practical care, particularly towards the end of life. London: Royal College of Physicians Smith, H.A., Kindell J., Baldwin, R.C., Waterman, D. and Makin, A.J. (2009) Swallowing problems and dementia in acute hospital settings: practical guidance for the management of dysphagia. Clinical Medicine 2009, Vol 9, No 6: 544–8
 Palliative Care in Severe Dementia, Quay Books, London. Pollens R. (2004)Role of the speech-language pathologist in palliative hospice care Journal of Palliative Medicine. 7 (5) (pp ), Sullivan RJ. Accepting death without artificial nutrition or hydration. J Gen Intern Med 1993; 8:220–224. Royal College of Physicians and British Society of Gastroenterology (2010) Oral feeding difficulties and dilemmas: A guide to practical care, particularly towards the end of life. London: Royal College of Physicians. Smith, H.A., Kindell J., Baldwin, R.C., Waterman, D. and Makin, A.J. (2009) Swallowing problems and dementia in acute hospital settings: practical guidance for the management of dysphagia. Clinical Medicine 2009, Vol 9, No 6: 544–8.")
Similar presentations







>")

 Dr Oliver J Corrado, Consultant Geriatrician, Leeds Teaching Hospitals and LTHT ‘Dementia Champion’>")












