Download presentation
Presentation is loading. Please wait.

1
Shoulder Objective Examination How to Interpret Special Tests

2
Special Tests Lots of test for different pathologies Some tests can be used for different pathologies Interpreting results can be confusing Statistics can be used to help ‘Guide’ us

3
Diagnostic Tests Tests can be positive Test can be negative BUT Test might be positive when the pathology may not be present Test might be negative when the pathology is present

4
Confused?

5
Diagnostic Tests Condition Present Condition Not Present Test PositiveTRUE POSITIVEFALSE POSITIVE Test NegativeFALSE NEGATIVE TRUE NEGATIVE

6
Time for some maths!!!

7
Diagnostic Tests Condition Present Condition Not Present Test PositiveTRUE POSITIVE A FALSE POSITIVE B Test NegativeFALSE NEGATIVE C TRUE NEGATIVE D Sensitivity A/(A+C) Specificity D/(B+D)
 Specificity D/(B+D)")
8
E.g 100 people have an ACL rupture confirmed through surgery Anterior Draw test was completed on all 100 It was positive 87 times It was therefore negative 13 times 50 people did not have an ACL rupture confirmed through surgery Anterior Draw test was completed on all 50 It was positive 20 times It was therefore negative 30 times N.B These figures are made up!!

9
Diagnostic Tests Condition Present Condition Not Present Test Positive8720 Test Negative1330 Sensitivity 87/(87+13) Specificity 30/(20+30)
 Specificity 30/(20+30)")
10
E.g In the example ACL case the anterior draw test gives the following properties Sensitivity – 87% Specificity – 60%

11
Sensitivity Proportion of patients with the condition who have a positive test result Tests with high sensitivity have few false negative, therefore a negative result RULES OUT the condition

12
Specificity Proportion of patients without the condition who have a negative test result Tests with high specificity have few false positive, therefore a positive results RULES IN the condition

13
Likelihood Ratios Likelihood ratios combine the sensitivity and specificity of a test By doing this you can compare with other test You can also work out the probability of tests being present when test RESULTS are COMBINED

14
Likelihood Ratios Positive Likelihood Ratios – The change in ODDS favouring the disorder given a positive test = ((Sensitivity/(1-Specificity)) Helpful for RULING IN The bigger the better Values > 5.0 are useful Negative Likelihood Ratio – The change in ODDS favouring the disorder given a negative test = ((1-Sensitivity)/Specificity) Helpful for RULING OUT The smaller the better Values < 0.30 are useful
) Helpful for RULING IN The bigger the better Values > 5.0 are useful Negative Likelihood Ratio – The change in ODDS favouring the disorder given a negative test = ((1-Sensitivity)/Specificity) Helpful for RULING OUT The smaller the better Values < 0.30 are useful")
15
E.G Anterior Draw Test – Sensitivity 87% – Specificity 60% Positive Likelihood Ratio 0.87/(1-0.6) 2.175 Negative Likelihood Ratio (1-0.87)/0.6 0.22 So from the example of the anterior draw it is a good test to rule OUT an ACL tear, but not so good at ruling IN a tear.
 Negative Likelihood Ratio (1-0.87)/0.6 0.22 So from the example of the anterior draw it is a good test to rule OUT an ACL tear, but not so good at ruling IN a tear.")
16
Probability and Odds To utilise Likelihood ratio we need to know the pre-test probability and odds E.G 25% of knee injuries in population aged 19-15 are ACL ruptures Therefore pre-test probability of an ACL rupture is an 25% Pretest odds= ((Pre test probability/ (1-pretest probability))
)")
17
Probability and Odds Pretest odds= ((Pre test probability/ (1-pretest probability)) Pretest odds = ((0.25/(1-0.25)) Pretest odds = 0.333 Posttest Odds = Pretest odds X Likelihood Ratio
) Pretest odds = ((0.25/(1-0.25)) Pretest odds = Posttest Odds = Pretest odds X Likelihood Ratio")
18
Likelihood Ratios Pre-Test Odds x Likelihood Ratio = Post Test Odds 0.3X2.18=0.654 0.3X0.22=0.066

19
Probability and Odds Posttest Probability = Posttest Odds/(Posttest odds + 1) Posttest Probability = 0.65/(0.65+1) Posttest Probability = 0.39 Posttest Probability = 39%
 Posttest Probability = 0.65/(0.65+1) Posttest Probability = 0.39 Posttest Probability = 39%")
20
E.G So from our example of the ACL injury and anterior draw A positive Anterior Draw – Increases chance of ACL rupture being present from 25% to 39% A negative Anterior Draw – Decreases change of ACL rupture being present from 25% to 5%

21
Likelihood Ratios By using likelihood ratios and pretest odds we can work out the probability of a pathology being present when multiple tests are combined More positive tests the more chance the pathology is present More negative test the more chance the pathology isn’t present

22
The Shoulder Special Tests

23
Subacromial Impingement TestSensitivitySpecificity+ LR- LR Neer’s 70.0052.553.950.84 Hawkins Kennedy 78.5855.082.230.39 Painful Arc 57.2066.512.050.69 Supraspinatus/ Empty Can 55.4058.311.920.89 Resisted External Rotation 47.6768.412.600.85

24
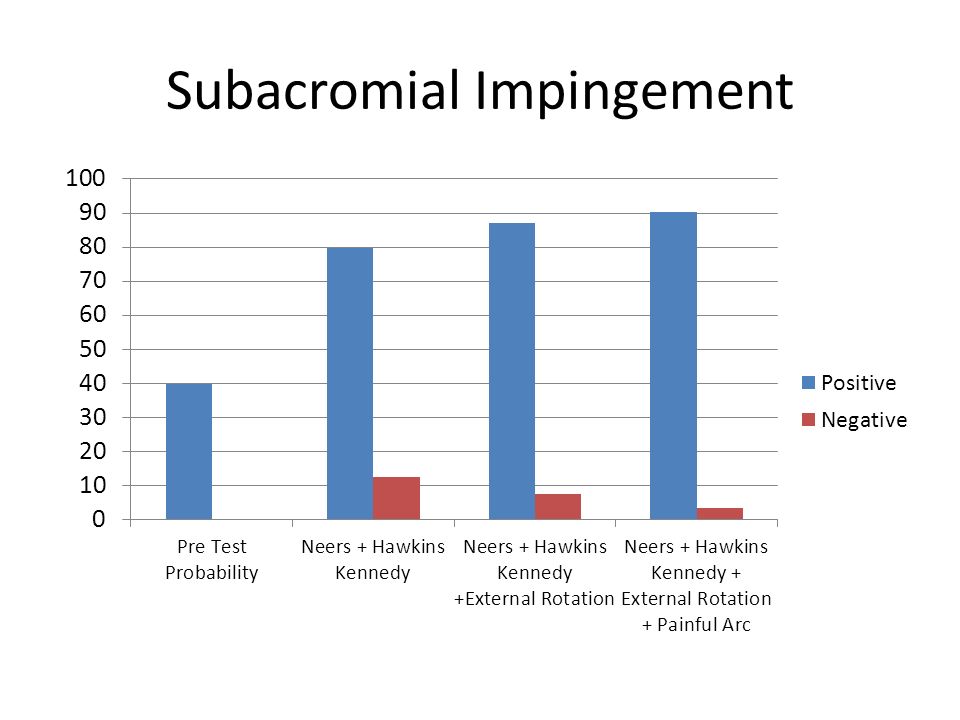
Subacromial Impingement

26
Published results – Positive Hawkins Kennedy – Painful Arc Sign – Resisted External Rotation – Positive Likelihood 5.03 (2+); 10.6 (3) – Post Test Probability 90% (2+); 95% (3) (Park et al., 2005)Park et al., 2005 Accumulation – Positive Neer’s – Positive Hawkins Kennedy – Positive External Rotation – Painful Arc – Post Test Probability 80% (2+) 87% (3+) 90% (4)
; 10.6 (3) – Post Test Probability 90% (2+); 95% (3) (Park et al., 2005)Park et al., 2005 Accumulation – Positive Neer’s – Positive Hawkins Kennedy – Positive External Rotation – Painful Arc – Post Test Probability 80% (2+) 87% (3+) 90% (4)")
27
Anterior Instability Apprehension AND Relocation Sensitivity – 81% Specificity – 98% + LR – 39.68 - LR – 0.19

28
Labral Tear Apprehension AND Relocation Sensitivity – 38% Specificity – 93% + LR – 5.43 - LR – 0.67

29
Rotator Cuff Tear Age > 65 AND Weakness in ER AND Night Pain Sensitivity – 49% Specificity – 95% + LR – 9.84 - LR – 0.54

30
SLAP Passive Distraction AND Active Compression Sensitivity – 70% Specificity – 90% + LR – 7.00 - LR – 0.11

31
Does this really help? Not really! The tests for the shoulder possess poor diagnostic properties Relies on an in depth knowledge of the properties and a flare with maths This only important when referring for further investigations (ESP Role or Consultant)
.")
32
Does this really help? 1.Special Tests of the shoulder can help to guide a diagnosis 2.Grouping of tests can lead to relatively accurate diagnosis 3.They DO NOT show us what to treat 4.They are inferior to MRI or Arthroscopic surgery

33
What should I do? Be aware of tests and how to perform them Use them in your exam to help differentially diagnosis if required Special Tests are an adjunct to a standard exam IMPORTANT Treat what you find from your exam. IMPORTANT Refer on if symptoms do not improve within 3-4 session for accurate diagnostic tests e.g MRI, Ultrasound etc

34
References Hegedus EJ, Goode A, Campbell S, et al. Physical examination tests of the shoulder: a systematic review with meta-analysis of individual tests. Br J Sports Med 2008; 42(2): 80-92; discussion Hegedus EJ, Goode AP, Cook CE, et al. Which physical examination tests provide clinicians with the most value when examining the shoulder? Update of a systematic review with meta-analysis of individual tests. Br J Sports Med 2012; 46(14): 964-78. Park HB, Yokota A, Gill HS, El Rassi G, McFarland EG. Diagnostic accuracy of clinical tests for the different degrees of subacromial impingement syndrome. J Bone Joint Surg Am 2005; 87(7): 1446-55. van der Windt DA, Koes BW, de Jong BA, Bouter LM. Shoulder disorders in general practice: incidence, patient characteristics, and management. Ann Rheum Dis 1995; 54(12): 959-64.
: 80-92; discussion Hegedus EJ, Goode AP, Cook CE, et al. Which physical examination tests provide clinicians with the most value when examining the shoulder. Update of a systematic review with meta-analysis of individual tests. Br J Sports Med 2012; 46(14): Park HB, Yokota A, Gill HS, El Rassi G, McFarland EG. Diagnostic accuracy of clinical tests for the different degrees of subacromial impingement syndrome. J Bone Joint Surg Am 2005; 87(7): van der Windt DA, Koes BW, de Jong BA, Bouter LM. Shoulder disorders in general practice: incidence, patient characteristics, and management. Ann Rheum Dis 1995; 54(12):")
Similar presentations



 Director of Evidence-Based Practice, Quality Management.>")















