Download presentation
Presentation is loading. Please wait.

1
Chronic Kidney Disease

3
Coresh J, Astor BC, Greene T, Eknoyan G, Levey AS
Coresh J, Astor BC, Greene T, Eknoyan G, Levey AS. Prevalence of chronic kidney disease in the adult US population: Third National Health and Nutrition Examination Survey. Am J Kidney Dis 2002;41:1-12

4
CKD stage GFR (ml/min/1.73m2) Description 1 >90 2 60-89 3 30-59 4
Normal renal function but other evidence of organ damage* 2 60-89 Mild reduction in renal function with other evidence of organ damage* 3 30-59 Moderately reduced GFR 4 15-29 Severely reduced GFR 5 <15 End stage, or approaching, end stage renal failure * Structural (eg APCKD), functional (eg proteinuria) or biopsy proven GN
, functional (eg proteinuria) or biopsy proven GN.")
6
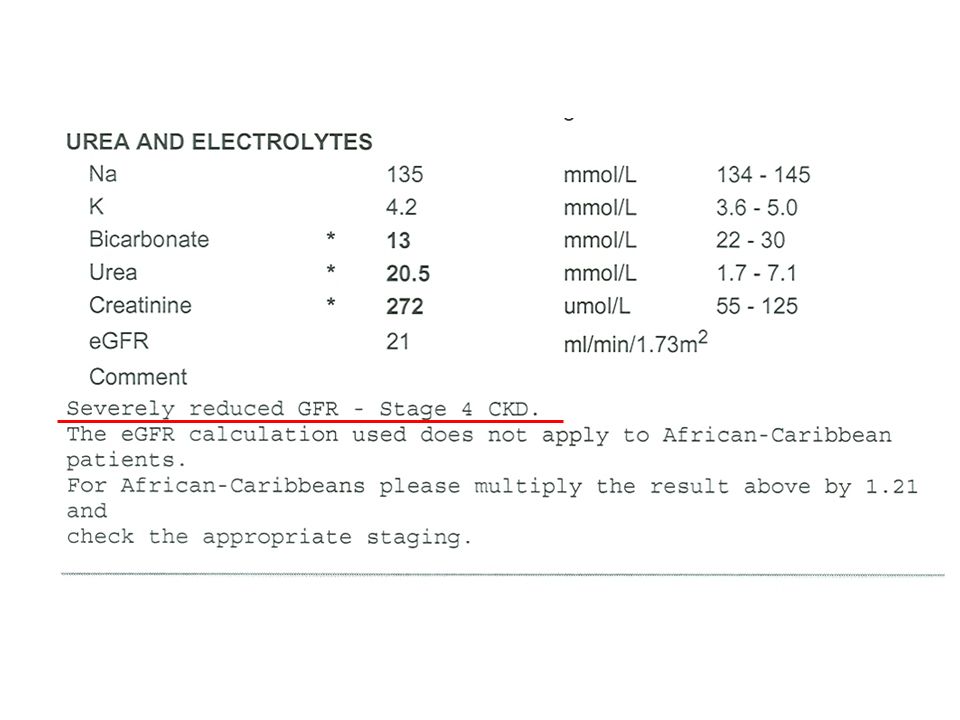
Creatinine 120 eGFR 31-40 eGFR

7
Fig 2 Commonly used formulas for estimating renal function
Fig 2 Commonly used formulas for estimating renal function. MDRD=modification of diet in renal disease Traynor, J. et al. BMJ 2006;333: Copyright ©2006 BMJ Publishing Group Ltd.

8
Association of estimated glomerular filtration rate (GFR) with GFR measured by an isotopic reference method. Below 60 ml/min/1.73 m2 the two methods are tightly associated, with limited scatter of the points. At higher filtration rates scatter becomes progressively worse, and in kidney donors estimated GFR underestimates renal function compared with reference measurements. Adapted from Poggio et al. Giles, P. D et al. BMJ 2007;334:

9
Caveats Only an estimate
Inaccurate at extremes of body habitus, pregnant, amputees Only validated in Caucasians and Afro-Caribbeans Underestimates function in kidney donors MDRD underestimates renal function, C-G overestimates it Only valid in steady state

10
GFR > 60 Estimated GFR not very accurate
If GFR > 60, use increase in serum creatinine > 20% as indicator of renal deterioration

11
2% of NHS budget spent on RRT
Coresh J, Astor BC, Greene T, Eknoyan G, Levey AS. Prevalence of chronic kidney disease in the adult US population: Third National Health and Nutrition Examination Survey. Am J Kidney Dis 2002;41:1-12

12
CKD stage GFR (ml/min/1.73m2) Description 1 >90 2 60-89 3 30-59 4
Normal renal function but other evidence of organ damage* 2 60-89 Mild reduction in renal function with other evidence of organ damage* 3 30-59 Moderately reduced GFR 4 15-29 Severely reduced GFR 5 <15 End stage, or approaching, end stage renal failure Insert p for proteinuria Insert p for proteinuria Insert p for proteinuria 3a and 3b 3a and 3b 3a and 3b 45-49 and 30-44 45-49 and 30-44 * Structural (eg APCKD), functional (eg proteinuria) or biopsy proven GN
, functional (eg proteinuria) or biopsy proven GN.")
13
NICE guidelines Sept 2008 People who have or are at risk of developing CKD Those who need intervention to minimise cardiovascular risk and what that intervention should be Those who will develop progressive kidney disease and how they can be managed Those who need referral for specialist kidney care

14
Offer testing for CKD Diabetes HTN CV disease: IHD, CHF, PVD, CVD
Structural disease, calculi or BPH Multisystem eg SLE FHx CKD 5 or hereditary kidney disease Nephrotoxins (CNIs or ACE inhibitors) Opportunistic detection of h’turia or p’uria
 Opportunistic detection of h’turia or p’uria.")
15
Proteinuria Use albumin: creatinine ratio (ACR) (more sensitive at low levels) ACR in diabetes PCR may be used for quanitification and monitoring

16
Don’t offer testing… On basis of Age Gender Ethnicity
Obesity without metabolic syndrome, diabetes or HTN

17
Who needs a renal ultrasound?
All people with CKD with Progressive CKD Haematuria Obstructive symptoms > 20 yrs with FHx polycystic kidneys CKD 4-5 Prior to biopsy

18
Who should be referred? CKD 4 and 5 (with or without diabetes)
ACR > 70 unless diabetic and already treated ACR > 30 and haematuria GFR declining > 5 /yr or 10 in 5 yr Uncontrolled HTN despite 4 agents Suspect rare or genetic cause CKD Suspect renal artery stenosis

19
Consider discussion with nephrologist by phone or letter if you feel clinic referral may not be necessary Single clinic visit with agreed management plan and specified criteria for re-referral may be all that is necessary

20
Identify progressive CKD
Obtain minimum 3 GFRs over not less than 90 days If new finding low GFR, repeat within 2 weeks to exclude ARF

22
Case history Mr RB, 69 years old, Type II diabetes
“Please see this man with CKD 4…” PMHx: DM, ileal conduit and pyelonephritis, dyspepsia DHx: Atenolol, gliclazide, metformin, simvastatin, lansoprazole, GTN spray

23
Started lansoprazole

24
Tubulo-interstitial nephritis

25
Identify progressive CKD
Obtain minimum 3 GFRs over not less than 90 days If new finding low GFR, repeat within 2 weeks to exclude ARF Define progression as GFR fall > 5 /yr or 10 in 5 yrs Extrapolate current rate of decline: will pt need RRT in their life time?

26
Will their kidneys fail in their lifetime?
Extrapolate current rate of decline: will pt need RRT in their life time? Will their kidneys fail in their lifetime? Will they die of something else first?

27
45 yrs old eGFR 50 Type II diabetes BP 160/90 P’uria 2.6g/day 80 yrs old eGFR 50 No PMHx BP 120/60 P’uria 0.3g/day RENAL RISK

28
Manage cardiovascular risk factors
CKD stage 3p Progressive Do refer CKD stage 3a Manage cardiovascular risk factors Don’t refer

29
In people aged over 70 years, eGFR 45-59, if stable over time and without any other evidence of kidney damage, unlikely to be associated with CKD related complications

30
Will they die of something else first?
Extrapolate current rate of decline: will pt need RRT in their life time? Will their kidneys fail in their lifetime? Will they die of something else first?

31
100 patients with eGFR < 60 (Tuesday morning in Outpatients)
")
32
Tuesday morning 1 year later: 1 patient needs RRT, 10 patients have died (> 50% CV death)
")
33
Tuesday morning 10 years later: 8 patients need RRT, 65 patients have died, 27 have ongoing CKD

34
The majority of patients with CKD 1-3 do not progress to ESRF.
Their risk of cardiovascular death is higher than their risk of progression.

35
O’Hare et al JASN 2007

36
Optimise risk factors Cardiovascular disease Proteinuria Hypertension
Diabetes Smoking Obesity Exercise tolerance

37
ACE inhibitor/ ARBs Offer to: Diabetes and ACR > 2.5 ± HTN/CKD
Non-diabetic with CKD and high BP and ACR 30+ mg/mmol (0.5g/24 hrs) Non-diabetic with CKD and ACR > 70 regardless of blood pressure or risk factors Titrate to maximum tolerated dose before add in second agent
 Non-diabetic with CKD and ACR > 70 regardless of blood pressure or risk factors. Titrate to maximum tolerated dose before add in second agent.")
38
What is an acceptable rise in creatinine?
Primary renal damage Loss of nephrons Hyperfiltration of remaining nephrons Focal sclerosis Hyperfiltration theory Mesangial cell proliferation and matrix expansion Increased glomerular pressure Mesangial cell and endothelial cell injury

39
What is acceptable? 25% increase eGFR 30% increase creatinine K up to 6.0

40
check U and Es 1-2 weeks after starting ACE inhibitor
Always check U and Es 1-2 weeks after starting ACE inhibitor Recheck after dose increase Advise stopping ACEI with dehydrating illness Counsel women of child bearing age

41
Blood pressure control
Systolic < 140 (aim mm Hg) Diastolic < 90 mm Hg If diabetes or proteinuria, aim 130/80 mm Hg
 Diastolic < 90 mm Hg. If diabetes or proteinuria, aim 130/80 mm Hg.")
42
What do we do in CKD clinic?

44
Mr KH “Please see this well 73 year old with diabetes..”
PMHx: DM, IHD, cerebrovascular disease, SCC DHx: gliclazide, lansoprazole, metformin, quinine, sildenafil, simvastatin, valsartan, clopidogrel BMI 33, BP 132/80 Ur 8.0, Cr 129, PCR 125 mg/l, HbA1C 8.3%

45
Mr KH (cont’d) Address proteinuria Maximise ACE/ RAS inhibition
 Address proteinuria Maximise ACE/ RAS inhibition")
46
Mr KH (cont’d) Risk factor modification: Address proteinuria
Maximise ACE/ RAS inhibition Risk factor modification: Lifestyle Meticulous BP control Lipid management Glycaemic control

47
Sound familiar?

48
CKD 3 management in primary care
Diabetes, ischaemic heart disease, hypertension Risk factor management Not much specialist renal medicine involved in majority of CKD 3 Refer if refractory hypertension, complications of renal failire, renal artery stenosis etc… Identify those with progressive CKD and refer

49
The metabolic complications of CKD
Uraemia Hypertriglyceridaemia Hyperphosphataemia Metabolic acidosis Hyperkalaemia Ca absorption and lipoprotein activity reduced Malnutrition, LVH, anaemia PTH increases at GFR 50-60

50
“Patients receiving comprehensive care by the renal team have shown:
slower rates of decline in renal function greater probability of starting dialysis with higher haemoglobin, better calcium control and permanent access a greater likelihood of choosing peritoneal dialysis.” Lewis EJ, Hunsicker LG, Clarke WR, Berl T, Pohl MA, Lewis JB, et al. for the Collaborative Study Group. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes N Engl J Med :851–860.

51
Why bother? Manage risk factors
Further investigations (? reversibility) Delay progression to ESRF Identify and treat complications Bone Anaemia Malnutrition
 Delay progression to ESRF. Identify and treat complications. Bone. Anaemia. Malnutrition.")
52
Secondary care Primary care
Coresh J, Astor BC, Greene T, Eknoyan G, Levey AS. Prevalence of chronic kidney disease in the adult US population: Third National Health and Nutrition Examination Survey. Am J Kidney Dis 2002;41:1-12

53
“Since the introduction of eGFR reporting (together with a programme of education in primary care), the proportion of new dialysis patients referred late (defined as within 90 days) has fallen from 38% to 25% (p<0.01).” BMJ 2007;334:1287 (23 June), doi: /bmj A
, doi: /bmj A.")
54
Any questions?

Similar presentations




















 in General Practice>")
