Download presentation
Presentation is loading. Please wait.

1
Drugs for the MAU Clive Roberts

2
Which drugs am I expected to know about??
Extract from 5th year handbook

3
So what are drugs good at treating (or preventing)?
Pain Inflammation Infection Fluid retention Heart problems High blood pressure Epilepsy Parkinsonism Asthma / COPD Peptic ulcer disease Diarrhoea/constipation Depression Anxiety/sleeplessness Psychosis Metabolic /endocrine diseases Malignant disease Degenerative disease Haematological problems Etc Etc

4
A 45 year old lady presents with increasing wheeze over the previous 6 months. No past history of asthma. She is wheezy throughout both lungs and has a tachycardia. Her peak flow is 150 l/min. What immediate investigations are indicated? What immediate measures should be taken?

5
Acute asthma and COPD - available approaches
Oxygen Bronchodilators Salbutamol Ipratropium Aminophylline Anti-inflammatories Corticosteroids Intravenous Oral Anti-biotics

6
Severe asthma Sit patient up and give high flow O2
Check PEFR & O2 sats Nebulised bronchodilators salbutamol 5mg + ipratropium 500mcg (repeat after 15 min if needed) Prednisolone 40-50mg po stat Consider IV Magnesium sulphate 1.2-2g over 20 mins ABGs, CXR, FBC, U&Es
 Prednisolone 40-50mg po stat. Consider IV Magnesium sulphate 1.2-2g over 20 mins. ABGs, CXR, FBC, U&Es.")
8
General rules about Oxygen therapy
Correct hypoxia with an appropriate delivery device Check ABGs if SaO2 <93% or suspicion of ventilatory impairment or acidosis Some patients (esp. COPD) with chronic hypoxia rely on hypoxic drive and will hypoventilate on high flow O2
 with chronic hypoxia rely on hypoxic drive and will hypoventilate on high flow O2.")
9
Oxygen delivery devices

10
Hudson mask: variable performance

11
Nasal cannulae

12
Venturi devices: fixed performance

13
Key drug features Salbutamol – beta 2 stimulant
Easy to administer Watch for tremor and potassium level Ipratropium – muscarinic blocker Nebuliser and inhaler Few side effects Aminphylline – phosphodiesterase inhibitor Major dosing problems Severe adverse effects on CNS and heart Great caution needed

14
Key drug features Corticosteroids Safe in acute situations
IV hydrocortisone or oral prednisolone Avoid long term or rapidly repeated courses because lead to BP+, fluid retention, hypokalaemia, weight gain, Diabetes, osteoporosis, myopathy, skin fragility, gastric ulcer, reduced host defence, risk of hypocorticism

15
Infective Exacerbation of COPD Community Acquired Pneumonia
Antibiotic guidance Infection Antibiotic Treatment Duration of Treatment Comments Infective Exacerbation of COPD Amoxicillin 500mg po tds 5-7 days Penicillin allergic Doxycycline 100mg po bd 5 -7days Community Acquired Pneumonia Risk Factors in CAP (CURB-65) C = Confusion MTS 8 or less U = Urea > 7mmol/l R = Resp. Rate >/= 30/min B = BP Systolic < 90 mmHg +/- Diastolic </= 60 mmHg 65 = age >/= 65 yrs 3 or more of the above risk factors (CURB-65 Score >/=3) = Severe Community Acquired Pneumonia Non-severe Amoxicillin 500mg–1gram po tds plus* Clarithromycin 500mg po bd Amoxicillin 500mg-1gram IV tds plus* Clarithromycin 500mg IV bd can be used if a patient is unable to swallow or is not absorbing. *Amoxicillin monotherapy may be considered for (i) those previously untreated in the community or (ii) those admitted to hospital for non-clinical reasons who would otherwise be treated in the community. Non-severe Penicillin allergic Moxifloxacin 400mg po od Severe Co-amoxiclav 1.2grams IV tds plus Clarithromycin 500mg IV bd (Switching to Co-amoxiclav 625mg po tds plus Clarithromycin 500mg po bd) 7-10 days If systemic sepsis add Gentamicin 5mg/kg IV stat pending culture results Levofloxacin 500mg IV bd (Switching to Moxifloxacin 400mg po od)
 C = Confusion MTS 8 or less. U = Urea > 7mmol/l. R = Resp. Rate >/= 30/min. B = BP Systolic < 90 mmHg. +/- Diastolic </= 60 mmHg. 65 = age >/= 65 yrs. 3 or more of the above risk factors (CURB-65 Score >/=3) = Severe Community Acquired Pneumonia. Non-severe. Amoxicillin 500mg–1gram po tds. plus* Clarithromycin 500mg po bd. Amoxicillin 500mg-1gram IV tds. plus* Clarithromycin 500mg IV bd. can be used if a patient is unable to swallow or is not absorbing. *Amoxicillin monotherapy may be considered for (i) those previously untreated in the community or (ii) those admitted to hospital for non-clinical reasons who would otherwise be treated in the community. Non-severe Penicillin allergic. Moxifloxacin 400mg po od. Severe. Co-amoxiclav 1.2grams IV tds. plus Clarithromycin 500mg IV bd. (Switching to Co-amoxiclav 625mg po tds plus Clarithromycin 500mg po bd) 7-10 days. If systemic sepsis add Gentamicin 5mg/kg IV stat pending culture results. Levofloxacin 500mg IV bd. (Switching to Moxifloxacin 400mg po od)")
16
What might be the possible causes?
A 45 year old man known to be alcoholic and addicted to Valium is admitted following three tonic clonic seizures What might be the possible causes? Effect of alcohol on brain Metabolic abnormality 2ndry to alcohol Alcohol withdrawal Drug withdrawal Head injury Overdose of something

17
What specific urgent investigations are indicated?
CT scan Glucose and electrolytes, serum Calcium Toxicology

18
What will you prescribe?
Correct electrolytes, dehydration, hypoglycaemia Oxygen Treat alcohol withdrawal Vit B complex (Pabrinex) Give anti-epileptic treatment
 Give anti-epileptic treatment.")
19
Urgent anti-epileptic treatment for repeated fits
Lorazepam 4mg iv (repeat once after 10 mins if fits again) If no control after 30 mins Phenytoin 15mg/kg iv (1g for 70kg person over 20 mins), monitor BP & ECG, then maintenance dose of 100mg every 6-8hrs Consideration of ITU at 60 mins Subsequently:- Consider need for maintenance treatment Carbamazepine Valproate Phenytoin Lamotrigine Advise not to drive
 If no control after 30 mins Phenytoin 15mg/kg iv (1g for 70kg person over 20 mins), monitor BP & ECG, then maintenance dose of 100mg every 6-8hrs. Consideration of ITU at 60 mins. Subsequently:- Consider need for maintenance treatment. Carbamazepine. Valproate. Phenytoin. Lamotrigine. Advise not to drive.")
20
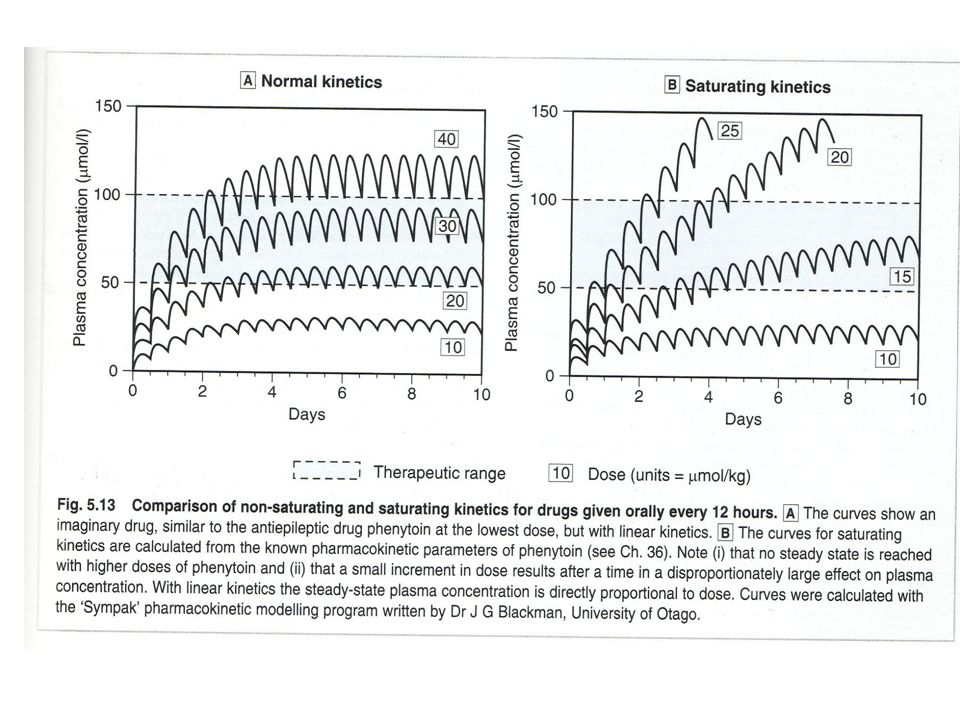
Key features of drugs Lorazepam – potent benzodiazepine with short half life Phenytoin – highly effective in controlling status epilepticus / repeated fits Low therapeutic ratio / complex pharmacokinetics / many adverse effects / precautions / drug interactions

26
Key features of drugs Carbamazepine Valproate
Effective prophylactic in most common epilepsies Powerful enzyme inducer Toxicity includes hepatic and blood disorders and hyponatraemia (SIADH) Valproate Also widely effective including absence seizures Possibly less problematic
 Valproate. Also widely effective including absence seizures. Possibly less problematic.")
27
A 60 year old man presents with severe shortness of breath at rest and orthopnoea. He has been waking at night with frightening episodes of dyspnoea. He is distressed and sweaty. Examination reveals elevated JVP some oedema of ankles. Crepitations throughout the lungs. Gallop rhythm at 120/min. BP 140/90. He had suffered an anterior myocardial infarction 3 years previously and has been on tablets for blood pressure.

28
Heart failure - approaches
Improve oxygenation Reduce pre-load Reduce blood volume – Diuretics Increase vascular capacity – Nitrates and other vasodilators Reduce afterload ACE inhibitors / AII blockers Reduce demands on myocardium Beta blockers (calcium channel blockers) Increase force of contraction Digoxin Reducedistress Morphine Avoid fluid overload, sodium retaining drugs, negative inotropes, arrhythmogenic
 Increase force of contraction. Digoxin. Reducedistress. Morphine. Avoid fluid overload, sodium retaining drugs, negative inotropes, arrhythmogenic.")
29
`

30
Severe heart failure Acute SOB, frothy sputum, tachypnoea, course crackles, hypoxia. May be cardiac history, ECG usually abnormal. Is there a precipitating cause? Need to exclude acute MI or arrhythmia Urgent ECG, CXR, bloods (inc TnI), ABGs Pay close attention to BP
, ABGs. Pay close attention to BP.")
31
Severe heart failure - treatment
Sit patient up, give high flow O2 (60-100%) Furosemide mg iv Diamorphine 2.5-5mg iv Metaclopramide 10mg iv GTN spray s/l then GTN (isoket) infusion 1-10mg/hr (monitor bp)
 Furosemide mg iv. Diamorphine 2.5-5mg iv. Metaclopramide 10mg iv. GTN spray s/l then GTN (isoket) infusion 1-10mg/hr (monitor bp)")
32
Key drug features Furosemide – loop/high ceiling dose diuretic
Safe for rapid IV injection, rapid diuresis but depends on renal function Risk of over-diuresis, hypokalaemia, and in longer term gout and hyponatraemia ACE inhibitors Risk of early drop in BP and renal function Minor hyperkalaemia and cough in long term

33
Digoxin – NA/K ATPase inhibitor
Key drug features Digoxin – NA/K ATPase inhibitor Negative chronotrope/positive inotrope Most useful in atrial fibrillation / limited in SR (except in children) Risk of AV block / supraventricular and ventricular tachyarrhythmias esp if low K+ Elderly and renal impairment predispose to toxicity which starts with nausea and progresses to CNS effects. Morphine – CNS effects – also venodilator
 Risk of AV block / supraventricular and ventricular tachyarrhythmias esp if low K+ Elderly and renal impairment predispose to toxicity which starts with nausea and progresses to CNS effects. Morphine – CNS effects – also venodilator.")
34
Key drug features Nitrates – venodilators Beta blockers
Reduce pre-load therefore good in LVF with preserved cardiac output Sublingual / iv infusion Risk to BP Beta blockers Reduce mortality in heart failure in long term by decreasing sympathetic drive but use only when stable or if severe tachycardia

35
Acute Pain Paracetamol Codeine NSAIDs
Effective as aspirin, antipyretic but not anti-inflammatory, not GI adverse effect, dangerous in o/d Codeine Opioid so causes drowsiness and constipation NSAIDs Effective in somatic pain but risk of/in GI, renal, heart failure, hypertension, hypersensitivity, hepatic damage, alveolitis, skin diseases, pancreatitis. Drug interactions ++ Opiates, Morphine and diamorphine Vary in potency for somatic and visceral pain and adverse effect but all tend to affect mood, respiration, GI motility. Risk of addiction

36
A 90 year old lady is admitted coughing up blood and with pleuritic pain in her R side
She had had bilateral ankle swelling CXR clear, D dimer raised, S1Q3T3 on ECG Current treatment amoxycillin –just started, carbamazepine for trigeminal neuralgia, aspirin prophylactic, diclofenac for shoulder pain.

37
Outline of treatment regime
Low molecular weight heparin for 5 days Load with warfarin Daily INR Adjust warfarin according to recommendation on chart Deal with over anti-coagulation according to BNF

38
Key features of anticoagulants
Warfarin suppresses synthesis of Vit K dependent clotting factors in liver (II,VII,IX and X). Therefore slow onset and offset. Effect easily monitored by prothrombin time (INR) Dose requirement highly susceptible to pharmacokinetic and pharmacodynamic variation from disease states, drug interaction and compliance. Many people die from over anti-coagulation each year
. Therefore slow onset and offset. Effect easily monitored by prothrombin time (INR) Dose requirement highly susceptible to pharmacokinetic and pharmacodynamic variation from disease states, drug interaction and compliance. Many people die from over anti-coagulation each year.")
39
WARFARIN- Indications
Long-term anti-thrombotic treatment Treatment of DVT or PE Prevention of arterial thrombosis in…… Atrial fibrillation Mechanical or bio-prosthetic valves Peripheral vascular disease Cerebrovascular disease Ischaemic heart disease

40
WARFARIN- Important interactions
Assume all co-prescriptions will alter warfarin dose response Cause over-anticoagulation Amiodarone PPI’s Statins Fluconazole Erythromycin Cause under-anticoagulation Barbiturates Carbemazepine Rifampicin Cholestyramine Anti-platelet agents increase bleeding risk

41
Description & action- HEPARIN
Parenteral anticoagulant Naturally occurring glycosaminoglycan Mixture of different length molecules (UFH av LMWH av ) How it works Increases activity of plasma Antithrombin Inhibits active clotting factors esp. factors IIa and Xa (LMWH inhibits Xa better)
 How it works. Increases activity of plasma Antithrombin. Inhibits active clotting factors esp. factors IIa and Xa. (LMWH inhibits Xa better)")
42
PHARMACOLOGY OF HEPARINS
UF HEPARIN LMW HEPARIN Route IV SC Bioavailability Variable, poor Predictable, good Metabolism Complex, mostly renal Predictable renal T1/2 (hours) 1-2 4-6
")
43
Presentation- UF Heparin
Vials containing.. 25,000 IU/ml (sc) 5, IU/ml 1, IU/ml (flush) IU/ml (flush) Typical dose 5000 IU loading then 30,000 IU by iv infusion / 24 hrs
 5,000 IU/ml. 1,000 IU/ml (flush) IU/ml (flush) Typical dose IU loading then. 30,000 IU by iv infusion / 24 hrs.")
44
Presentation- LMW heparin
4 generic preparations eg Tinzaparin (Innohep) Enoxaparin (Clexane) Pre-filled syringes Clexane 100 mg/ml; 20, 40, 60, 80, 100, 120, 150 mg syringes Typical doses 40mg sc once daily ‘prophylactic’ 100 mg sc once daily ‘treatment’
 Enoxaparin (Clexane) Pre-filled syringes. Clexane 100 mg/ml; 20, 40, 60, 80, 100, 120, 150 mg syringes. Typical doses. 40mg sc once daily ‘prophylactic’ 100 mg sc once daily ‘treatment’")
45
HEPARINS- Indications
Anti-thrombotic activity with rapid onset /offset Initial treatment of DVT or PE LMWH Acute coronary syndromes LMWH Cardiothoracic surgery UFH Other extra-corporeal circuits UFH Warfarin unsuitable esp pregnancy LMWH Prophylaxis against venous thrombosis LMWH

Similar presentations










? Pain Inflammation Infection Fluid retention Heart problems High.>")













