Download presentation
Presentation is loading. Please wait.

1
Cultural Competence and Risk Communication
Presented by Darci L. Graves, MA, MA University of Maryland-Baltimore County Cultural competence serves as a compliment to language access mandates. While federal and state requirements regarding language access are not new, many health care professionals lack training regarding how to go about putting these requirements into practice, as well as the knowledge of the language access laws themselves. Cultural competence training may serve to partially address the current barriers that affect language access programs while also addressing the needs of diverse populations. The field of health care access can benefit greatly from the collaboration and cooperation of these two areas.

2
Today’s Objectives Explain how preparedness messages are perceived across various cultures Discuss the significance of delivering culturally appropriate preparedness messages Describe strategies for culturally competent communications during a public health emergency

3
Cultural Competence & The Front Page
Terrorism/Violence 9/11 Iraq Virginia Tech Natural Disasters Tsunami Katrina Celebrity “Missteps” Michael Richards Isaiah Washington Don Imus Richard Gere Not to mention Health Insurance Immigration

4
People prepare, respond, and recover from disaster within the context of their culture.
Culture offers a protective system that is both comforting and reassuring. It defines appropriate behavior and furnishes a support system, and identifies a shared vision for recovery. Despite the strengths of culture, responses from some groups may make them more vulnerable than others.

6
; Mona Lisa, or La Gioconda (La Joconde), is a 16th century oil painting on poplar wood by Leonardo da Vinci
, is a 16th century oil painting on poplar wood by Leonardo da Vinci")
7
Impression Sunrise; 1873 – Radicals – Impressionists was coined as a satiric label

8
1889

9
1950; Lavender Mist

10
cross-cultural encounter.
Every encounter is a cross-cultural encounter. - Robert C. Like, MD, MS

11
Defining “Culture” Culture refers to integrated patterns of human behavior that include the language, thoughts, communications, actions, customs, beliefs, values, and institutions of racial, ethnic, religious, or social groups. [Based on Cross, T., Bazron, B., Dennis K., & Isaacs, M., (1998). Towards A Culturally Competent System of Care Volume I. Washington, D.C.: Georgetown University Child Development Center, CASSP Technical Assistance Center).
. Towards A Culturally Competent System of Care Volume I. Washington, D.C.: Georgetown University Child Development Center, CASSP Technical Assistance Center).")
12
Aspects of Culture that are also Health Determinants

13
Cultural Competence A historic progression in the U.S.:
Cultural awareness… Then cultural sensitivity… And now cultural competence.

14
Cultural Competence Cultural Competence is a set of congruent behaviors, attitudes, and policies that come together in a system, agency, or among professionals that enables effective work in cross-cultural situations. [1] HHS Office of Minority Health Culturally and Linguistically Appropriate Services Standards, at

15
Need for Cultural Competence
Respond to current and projected demographic changes in the United States Reduction of long-standing disparities in the physical and mental health - status of people from differing racial, ethnic and cultural backgrounds Improvement of the quality of services and primary care outcomes Compliance with legislative, regulatory and accreditation mandates Creation of a competitive edge in the market place Decrease in the likelihood of liability/malpractice claims A need for cultural competence is demonstrated by a 2003 Georgetown University, National Center for Cultural Competence policy brief. The brief identified several potential benefits that can be achieved through cultural competence. It may be important to include each of these rationales in the discussion at large as key reasons for emerging local, state and federal legislative efforts toward ensuring culturally competent care. In terms of policy making and legislation the reduction of health and healthcare disparities are by far the most common rationale as to why or at least how the issue is couched within the legislation. National Center for Cultural Competence

16
[1] Smedley, Stith and Nelson. 2003.
Health Disparities The Institute of Medicine, in its publication, “Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care,” determined that the “development and implementation of training programs for health care providers [around topics of cultural competence] offer promise as a key intervention strategy in reducing healthcare disparities”. [1] Recognition of health and health care disparities has contributed to a greater awareness that organizational and systemic interventions may be necessary to induce change. This perception has manifested itself in several arenas, including new legislation mandating the implementation of cultural competence training for health care professional development. The increased awareness of disparities has not been the only impetus for legislative efforts, but it has highlighted many initiatives. The legislative efforts are further discussed in subsequent sections. [1] Smedley, Stith and Nelson [1] Smedley, Stith and Nelson
![[1] Smedley, Stith and Nelson](http://slideplayer.com/slide/755030/2/images/16/%5B1%5D+Smedley%2C+Stith+and+Nelson.jpg "Health Disparities. The Institute of Medicine, in its publication, Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care, determined that the development and implementation of training programs for health care providers [around topics of cultural competence] offer promise as a key intervention strategy in reducing healthcare disparities . [1] Recognition of health and health care disparities has contributed to a greater awareness that organizational and systemic interventions may be necessary to induce change. This perception has manifested itself in several arenas, including new legislation mandating the implementation of cultural competence training for health care professional development. The increased awareness of disparities has not been the only impetus for legislative efforts, but it has highlighted many initiatives. The legislative efforts are further discussed in subsequent sections. [1] Smedley, Stith and Nelson [1] Smedley, Stith and Nelson")
17
Federal Legislation & Policies
Hill-Burton Act 1946 Civil Rights Act – Title VI 1964 Establishment of federal Office of Minority Health 1985 Hill-Burton Act – hospitals built with these designated funds agree to government oversight and to serve their respective communities Title 6 – dictates that no institution receiving federal funds may discriminate based on the grounds of race, color or national origin Executive Order – Improving Access to Services for Persons with Limited English Proficiency In 2001, the OMH issued the “Culturally and Linguistically Appropriate Services (CLAS) Standards” stating that every patient should receive respectful care that is culturally and linguistically appropriate[2]. The federal government furthered this commitment in its published report “Healthy People 2010” which unequivocally states that “every person in every community across the Nation deserves equal access to comprehensive, culturally competent, community-based health care systems that are committed to serving the needs of the individual and promoting community health”.[3] Healthy People 2000 1990 Healthy People 2010 2000 Executive Order 13166 2001 CLAS Standards Graves, D., Like, R., Hohensee, A. and Kelly, N
 Standards stating that every patient should receive respectful care that is culturally and linguistically appropriate[2]. The federal government furthered this commitment in its published report Healthy People 2010 which unequivocally states that every person in every community across the Nation deserves equal access to comprehensive, culturally competent, community-based health care systems that are committed to serving the needs of the individual and promoting community health .[3] Healthy People Healthy People Executive Order CLAS Standards. Graves, D., Like, R., Hohensee, A. and Kelly, N")
18
Cultural Competence Legislation
The proliferation of state legislation has garnered attention from a variety of sources. Some researchers have opined that institutional-level problems experienced in American health care must be addressed on the national rather than state level. This opinion is grounded in the fact that states lack the far-reaching power necessary to implement broad systemic change[1]. The debate of state versus federal powers falls outside of the scope of this article; but it is important to keep in mind that the boundaries between state and federal powers, and even between governmental agencies, may impact attempts at policy change.

19
National Standards on Culturally and Linguistically Appropriate Services (CLAS)
The CLAS standards are primarily directed at health care organizations; however, individual providers are also encouraged to use the standards to make their practices more culturally and linguistically accessible. The principles and activities of culturally and linguistically appropriate services should be integrated throughout an organization and undertaken in partnership with the communities being served. The 14 standards are organized by themes: Culturally Competent Care (Standards 1-3), Language Access Services (Standards 4-7), and Organizational Supports for Cultural Competence (Standards 8-14). Within this framework, there are three types of standards of varying stringency: mandates, guidelines, and recommendations as follows: CLAS mandates are current Federal requirements for all recipients of Federal funds (Standards 4, 5, 6, and 7). CLAS guidelines are activities recommended by OMH for adoption as mandates by Federal, State, and national accrediting agencies (Standards 1, 2, 3, 8, 9, 10, 11, 12, and 13). CLAS recommendations are suggested by OMH for voluntary adoption by health care organizations (Standard 14).
, Language Access Services (Standards 4-7), and Organizational Supports for Cultural Competence (Standards 8-14). Within this framework, there are three types of standards of varying stringency: mandates, guidelines, and recommendations as follows: CLAS mandates are current Federal requirements for all recipients of Federal funds (Standards 4, 5, 6, and 7). CLAS guidelines are activities recommended by OMH for adoption as mandates by Federal, State, and national accrediting agencies (Standards 1, 2, 3, 8, 9, 10, 11, 12, and 13). CLAS recommendations are suggested by OMH for voluntary adoption by health care organizations (Standard 14).")
20
Goal for Today’s Conference
The goal of the conference is to provide information and education on effective crisis communication principles using real-life examples as a guide.

21
What Is Risk Communication?
Risk communication has many definitions. Two basic ones are: 1) “An interactive process of exchange of information and opinion among individuals, groups and institutions. It involves…messages about the nature of risk and other messages not strictly about risk…that expresses concerns, opinions or reactions to risk messages…..” 2) "The exchange of information among interested parties about the nature, magnitude, significance or control of risk .”
 An interactive process of exchange of information and opinion among individuals, groups and institutions. It involves…messages about the nature of risk and other messages not strictly about risk…that expresses concerns, opinions or reactions to risk messages….. 2) The exchange of information among interested parties about the nature, magnitude, significance or control of risk .")
22
… there many goals of risk communication
"Enable individuals to "make informed… decisions for themselves and their community." "Dispel myths…reduce fears, and, in times of crisis, to alert the pubic and provide directions for urgent action."

23
Anticipate Community Needs Through OUTREACH
O - Outline Goals U - Understand Audience Beliefs & Bias T - Training & Team Building R - Resource Inventory E - Engage Community A - Adopt & Adapt Plan C - Communicate H - Hindsight Exchanging, Interacting, Preparing,

24
Outline Goals What is the threat you are trying to prevent?
What is the recommended response to avert the threat? Who is the target audience?

26
Understand Audience Beliefs and Bias
Gay/lesbian/bisexual/transgender Those in poverty Racial/ethnic minorities Religious/Spiritual minorities Persons with disabilities Patients with HIV/AIDS Children Older adults Cultural minorities (e.g., Amish, Appalachian) Military culture Migrant workers/homeless/displaced persons Persons with mental illness
 Military culture. Migrant workers/homeless/displaced persons. Persons with mental illness.")
27
Understand Audience Beliefs and Bias

28
Understand Audience Beliefs and Bias
Know Your Organization’s Reputation in the Community Recognize that some populations may have a distrust or fear of government and health institutions Refugees and immigrant populations Tuskegee Syphilis Study ( ) Conduct research to better understand your organization’s reputation Surveys and focus groups Meet with local leaders of community-based organizations Request feedback and input on how to improve or change reputation
 Conduct research to better understand your organization’s reputation. Surveys and focus groups. Meet with local leaders of community-based organizations. Request feedback and input on how to improve or change reputation.")
29
Understand Audience Beliefs and Bias
trust and credibility Center for Risk Communication

30
Understand Audience Beliefs and Bias
Who are the most vulnerable persons in the community? Where do they live? What is the range of family composition (i.e., single-parent households)? What cultural groups (ethnic, racial, and religious) live in the community? Where do they live, and what are their special needs? What are their values, beliefs, and primary languages? Who are the cultural brokers in the community?
 What cultural groups (ethnic, racial, and religious) live in the community Where do they live, and what are their special needs What are their values, beliefs, and primary languages Who are the cultural brokers in the community")
31
Understand Audience Beliefs and Bias
Does the community have any special economic considerations that might affect people’s vulnerability to disaster? Are there recognizable socioeconomic groups with special needs? How many live in rental property? How many own their own homes?

32
Training and Team Building
Training is perhaps the most important step. Once staff have taken a training program, their awareness is heightened, and they will be better equipped to design plans & programs that take into account the needs of culturally diverse & Limited English Proficient populations.

33
Training and Team Building
Training – have staff members received cultural competence training? “Champions” – are there any individuals who are committed to this cause, and if so, can they assist with the emergency preparedness plan? Form an Internal Team - Cultural Competence is an ongoing process and must be revisited through continual training and discussion.

34
Resource Inventory Representation – are any of your staff members of diverse communities who can serve as liaisons/advisors? Knowledge – Do existing staff members have a good understanding of the ethnic and linguistic composition of the community? Partners – Can vendors/suppliers support the plan?

35
Resource Inventory What services do you already utilize?
What partners do you already have? What experts do you have access to?

36
Resource Inventory Language Support
Translation Services (are written materials available in other languages?) Interpreting Services (can we communicate with members of the community via telephone and in person?) Bilingual Staff (how do I evaluate staff members’ language proficiency?)
 Interpreting Services (can we communicate with members of the community via telephone and in person ) Bilingual Staff (how do I evaluate staff members’ language proficiency )")
37
Resource Inventory Factors to Consider for TRANSLATION (written documents) Do we have a partner for translation services? If using in-house staff to translate, consider: Are these individuals truly qualified (ATA certified)? What are the indirect costs of taking this individual away from other work? What about errors and omissions insurance ($71 million lawsuit in Florida)? Does my staff have the tools and expertise necessary for industry standards related to professional translation (terminology management software, translation tools, desktop publishing, localization expertise, etc.)?
 What are the indirect costs of taking this individual away from other work What about errors and omissions insurance ($71 million lawsuit in Florida) Does my staff have the tools and expertise necessary for industry standards related to professional translation (terminology management software, translation tools, desktop publishing, localization expertise, etc.)")
38
Resource Inventory Questions to Ask for Quality Translation Services
Does the provider use translation memory tools? This is the industry standard. All professional providers should offer this as a feature to you. This results in cost savings due to economies of scale & translation terminology memory that is leveraged over time. Are there any hidden costs? Do not judge only on price per word. Ask for a clear list of all charges; if certain services are not offered (editing, proofreading, desktop publishing), where will these services be obtained? Does the provider offer culturally appropriate services? Ensure that your provider does cultural adaptation - not just simple linguistic transfer. Can the provider assist with literacy issues? If you know the average reading level of your target population, the translation provider should be able to adapt the reading level. Am I protected? The organization should provide qualified and certified translators only, and should offer comprehensive insurance.
, where will these services be obtained Does the provider offer culturally appropriate services Ensure that your provider does cultural adaptation - not just simple linguistic transfer. Can the provider assist with literacy issues If you know the average reading level of your target population, the translation provider should be able to adapt the reading level. Am I protected The organization should provide qualified and certified translators only, and should offer comprehensive insurance.")
39
Resource Inventory Factors to Consider for INTERPRETING (spoken language needs) Do we have a partner for interpreting services? What happens if the local area is affected (will the partner be affected as well?) Do we have access to an interpreting service that is available 24/7? Do we have access information readily available? Does the partner have a back-up/emergency redundancy plan? Do we have a list of volunteer interpreters/bilingual staff available for emergencies? Do we have a plan in place to notify/activate our back-up interpreters/volunteers?
 Do we have access to an interpreting service that is available 24/7 Do we have access information readily available Does the partner have a back-up/emergency redundancy plan Do we have a list of volunteer interpreters/bilingual staff available for emergencies Do we have a plan in place to notify/activate our back-up interpreters/volunteers")
40
Resource Inventory Factors to Consider for BILINGUAL STAFF (spoken language needs) Have staff members been tested for language proficiency? Written vs. oral Incentive or recognition program for testing Is there a roster of individuals with proven language proficiency? Proficiency does not equal interpreting or translation ability

41
Engage Community What resources and supports would community and cultural/ethnic groups provide during or following a disaster? Do the groups hold pre-existing mutual aid agreements with any State or county agencies? Who are the key informants/ gatekeepers of the impacted community? Has a directory of cultural resource groups, natural helpers, and community informants who have knowledge about diverse groups been developed? Are the community partners involved in all phases of disaster preparedness, response, and recovery operations?

42
Engage Community Ensure access to services and information
Consider teaming with other organizations Public safety / education resources / partnerships Identify Partners - Places of worship, other Government organizations, FBOs, CBOs, staff/volunteers, etc. Use all of these to share information.

43
Percent Distribution of NJ Population
Engage Community Percent Distribution of NJ Population 2004 Census Data New Jersey U.S. Population, percent change, April 1, 2000 to July 1, 2005 3.6% 5.3% 1990 to 2000 8.6% 13.1% Persons under 5 years old, percent, 2004 6.7% 6.8% Persons under 18 years old, percent, 2004 24.8% 25.0% Persons 65 years old and over, percent, 2004 12.9% 12.4% Female persons, percent, 2004 51.3% 50.8%

44
Percent Distribution of NJ Population
Engage Community Percent Distribution of NJ Population 2004 Census Data New Jersey U.S. White Persons 76.9% 80.4% Black Persons 14.5% 12.8% American Indian and Alaska Native Persons 0.3% 1.0% Asian Persons 7.0% 4.2% Native Hawaiian and Other Pacific Islander 0.1% 0.2% Persons Reporting Two or More Races 1.2% 1.5% Persons of Hispanic or Latino Origin 14.9% 14.1% White Person, not Hispanic 63.8% 67.4%

45
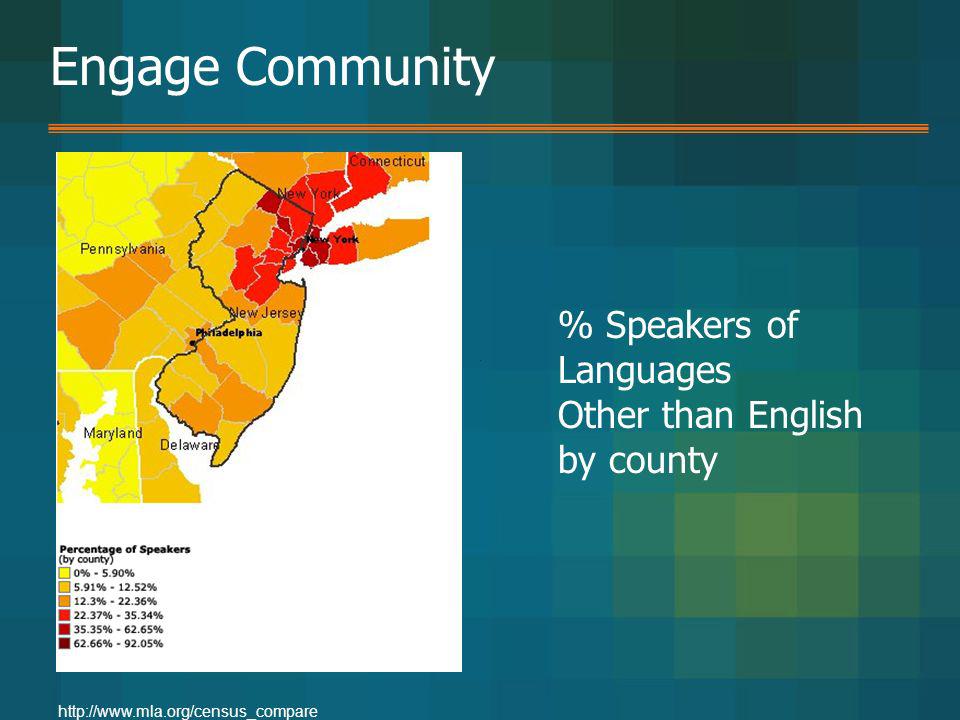
Engage Community Most spoken languages in New Jersey:
English is spoken by 74.53% of people over 5 years old in New Jersey. Languages other than English are spoken by 25.46%. Speakers of languages other than English are divided up as follows.

46
Engage Community % Speakers of Languages Other than English by county
47
Engage Community Mercer County Language Total % English 262,340 80.11%
All languages other than English combined 65, % Spanish 29, % Italian 4, % Polish 3, % Chinese 3, % French 2, % German 2, % French Creole 1, % Korean 1, % Russian 1, % Gujarathi 1, % Arabic 1, % Hindi 1, % Ukrainian 1, % Urdu % Tagalog % Greek % Japanese % Kru, Ibo, Yoruba % Hungarian % Mandarin % India % Tamil % Telugu % Hebrew % Formosan % Panjabi % Dutch % Turkish % Portuguese % Total: 327,457

48
Adopt & Adapt Plan What are the Federal, State, and local roles in disaster response? How do Federal, State, and local agencies relate to one another? Who would lead the response during different phases of a disaster? How can mental health services be integrated into the government agencies’ disaster response? What mutual aid agreements exist? Do any subgroups in the community harbor any historical or political concerns that affect their trust of government?

49
Adopt & Adapt Plan What are the roles of the American Red Cross, interfaith organizations, and other disaster relief organizations? What resources do non-government agencies offer, and how can local mental health services be integrated into their efforts? What mutual aid agreements exist? How can mental health providers collaborate with private disaster relief efforts?

50
Adopt & Adapt Plan Is there support for your plan from all participating parties? Internal staff External vendors / suppliers Organizational partners Community partners Public at large

51
Adopt & Adapt Plan Is the emergency preparedness plan appropriate from a cultural and linguistic standpoint? Communication – make sure that the communication channels in place are appropriate for reaching all affected populations Preparedness – have key messages (e.g. evacuation instructions, maps, emergency preparedness guides, etc.) translated in advance and distribute information to the community through channels Input – ask community leaders to provide insight for how to improve upon existing plans
 translated in advance and distribute information to the community through channels. Input – ask community leaders to provide insight for how to improve upon existing plans.")
52
Adopt & Adapt Plan Are policies and procedures in place to collect, maintain, and review current and emergent demographic data for any area that might be affected by a disaster? How could individuals be identified and reached in a disaster?

53
Communicate In your plan, identify communication channels and means of access, for example: Will printed copies of the information/resources be available? If so, at what locations (community centers, places of worship, other frequently visited sites within the community)? Will information be available in other media (web, telephone, etc.)? If so, will the access method be linguistically and culturally appropriate?
 Will information be available in other media (web, telephone, etc.) If so, will the access method be linguistically and culturally appropriate")
54
Communicate Is the emergency preparedness plan appropriate from a cultural and linguistic standpoint? Communication – make sure that the communication channels in place are appropriate for reaching all affected populations Preparedness – have key messages (e.g. evacuation instructions, maps, emergency preparedness guides, etc.) translated in advance and distribute information to the community through channels Input – ask community leaders to provide insight for how to improve upon existing plans
 translated in advance and distribute information to the community through channels. Input – ask community leaders to provide insight for how to improve upon existing plans.")
55
Hindsight What have we learned from the past? Katrina Anthrax
Pandemics

56
Hindsight Does the plan meet the goals?
Was the plan developed with the audience in mind? Are all the available resources being utilized? Are all stakeholders being trained? Has the community been engaged in developing the plan? Has the plan been adopted and adapted as necessary? Have past lessons been incorporated?

57
Considerations for Ongoing Evaluation
Can there be a task force dedicated to cultural and linguistic aspects of emergency preparedness in the state? If so, what other government entities might support this? (e.g. public safety) Can there be work teams within individual counties and cities that focus on these tasks? Will there be ongoing dialogue and sharing of best practices on this topic? If so, in what venue?
 Can there be work teams within individual counties and cities that focus on these tasks Will there be ongoing dialogue and sharing of best practices on this topic If so, in what venue")
58
Cultural Competence Should be a part of an organization’s overall mission and objectives as a component of all services (not just emergency preparedness). Cultural competence will aid in the establishment of trust and rapport which will be key when and if an emergency occurs.
. Cultural competence will aid in the establishment of trust and rapport which will be key when and if an emergency occurs.")
59
Keys to Implementation
Journey Mentality Training Collaboration Expert Partners Research Internal/External Policy Review Methodology Shared Understanding of Definition of “SUCCESS” To truly affect change, within our health institutions (public and private, academic and applied). We will need to evolve to reflect a culturally relevant and sensitive format. The key to this evolution will be ongoing and long term. For legislation to be effective and for health disparities to be reduced a myriad of variables will need to come together. Culturally competent healthcare may require support from various individuals, organizations and funding sources. But the legislation of such requirements goes a long way toward legitimizing them. Policymakers and practitioners will have to provide careful thought as to how best to teach adults, change behaviors and attitudes, curriculum content, implementation and other surrounding issues. Without such consideration a guarantee of culturally competent care could easily become an empty promise[3]. [1] Like, R. 2005 [2] Knowles, M [3] Beagin, B. 2003 Graves, D., Like, R., Kelly, N. and Hohensee, A
. We will need to evolve to reflect a culturally relevant and sensitive format. The key to this evolution will be ongoing and long term. For legislation to be effective and for health disparities to be reduced a myriad of variables will need to come together. Culturally competent healthcare may require support from various individuals, organizations and funding sources. But the legislation of such requirements goes a long way toward legitimizing them. Policymakers and practitioners will have to provide careful thought as to how best to teach adults, change behaviors and attitudes, curriculum content, implementation and other surrounding issues. Without such consideration a guarantee of culturally competent care could easily become an empty promise[3]. [1] Like, R [2] Knowles, M [3] Beagin, B Graves, D., Like, R., Kelly, N. and Hohensee, A")
60
Darci L. Graves darci.graves@gmail.com
Questions? Darci L. Graves

Similar presentations
















>")




