Download presentation
Presentation is loading. Please wait.

1
NOEL J STAUNTON (BSc, MRPharmS, MBA, Dip H.Econ)
Pharmaceutical Consultant-3i consultancy ltd Work with Pharma companies (Pfizer, GSK, BI, Novartis, Flynn, Shire, Galderma, Stiefel, Solvay, Takeda, Lundbeck etc, etc) Mob E mail
 Mob E mail")
2
TODAY NHS reorganisation –Why? PBR PBC WCC

3
TODAY Darzi Polyclinics Pharmacy White Paper PCO levers

4
Remember, people interpret things differently.
In July 2002 the WHO asked the UN Security Council: “What, in your honest opinion, can we do to solve the problem of the shortage of food in the rest of the world?”

5
Didn’t work because: East Europeans didn’t understand the word “honest” Chinese didn’t understand – “opinion” Middle Easterners didn’t understand – “solve” South Americans didn’t understand – “problem” Western Europeans didn’t understand – “shortage” Africans didn’t understand – “food” Americans didn’t understand – “rest of the world”

6
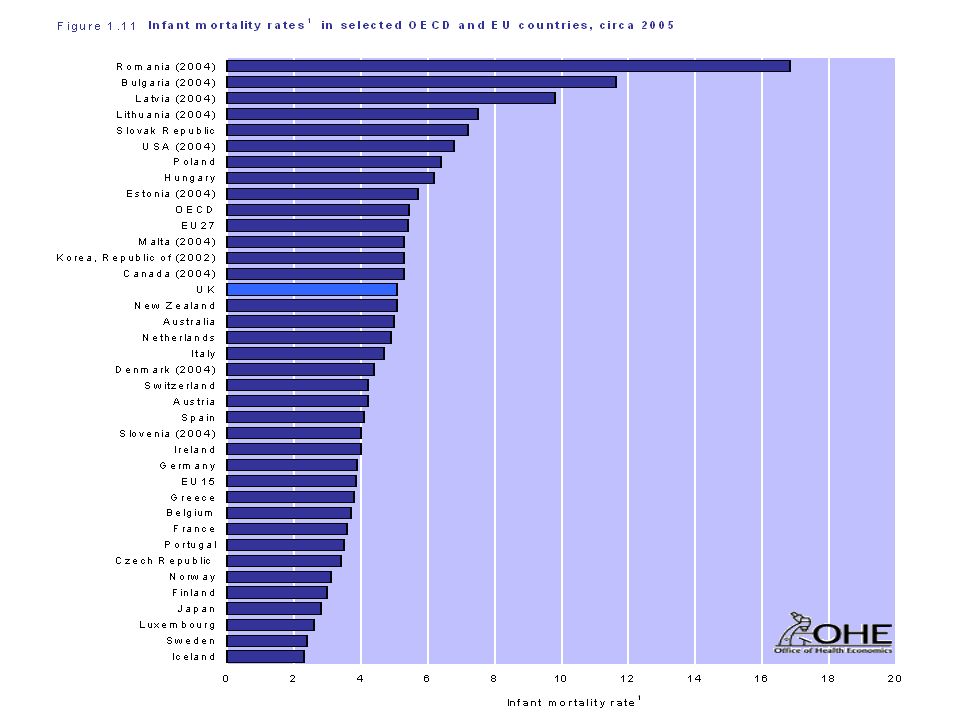
NHS REORGANISATION - WHY?
We’re spending more £s per head on health than EU15 and EU27 countries but our outcomes are poor

13
MOST (ALL?) NHS CHANGES REVOLVE AROUND SPENDING MORE IN PRIMARY CARE AND LESS IN SECONDARY CARE
PBR PBC World Class Commissioning GP contract, Community Pharmacy contract, Consultants contract Nurse and Pharmacist Prescribing Managing long term conditions Etc, Etc, Etc

14
PBR Old system - block contracts New system - PBR
PAY FOR WHOLE POPULATION Don’t know how much hospital care costs Can’t disinvest from secondary care New system - PBR PAY FOR EACH INDIVIDUAL PATIENT National tariff CAN DISINVEST FROM HOSPITALS

15
PBR England only (but Celtic nations eventually)
Copy of US system which DOES reduce hospital stay (Ref HSJ, 9th Dec 04, P 16) International phenomenon DRGs first in the USA -Medicare France uses US DRGs Italy uses modified version of US DRG system Germany & Netherlands from 2003 England, Australia, Norway, Austria, Finland, Sweden, Japan and Canada have own case mix tools
 International phenomenon DRGs first in the USA -Medicare. France uses US DRGs. Italy uses modified version of US DRG system. Germany & Netherlands from England, Australia, Norway, Austria, Finland, Sweden, Japan and Canada have own case mix tools.")
16
PBR - example acute MI A 55 year old man with a history of heart disease is admitted to coronary care with an MI. His condition is complicated by heart failure. He is discharged after 32 days. Consider a handout with this on.

17
PBR - example acute MI Patient is discharged from hospital.
Hospital finance clerk reads patient’s notes and types into her computer: Primary diagnosis – MI Secondary diagnosis -CHF PBR software spews out a code – HRG E11

18
PBR - example acute MI HRG E11 - non-elective spell = £4,787
Step 3 - Calculation of tariff price The tariff price for this patients admission (or ‘spell’) is calculated (by software applications) based on lists which map HRGs to tariff prices. The tariff for HRG D22 is listed as £1108 for an elective spell or £1,166 for a non-elective (emergency) spell. (See table 2 ). The length of stay was 3 days. Had this exceeded 11 days, then ‘trim points’ would have been applied, with an additional £196 per day being applied to the tariff. (The length of stay above which trim points are applied is specific to HRGs). Similarly, if the length of the emergency stay had been less than 2 days, the short stay tariff of £398 would have applied. For this patient the PCT will pay £1,138. A market forces factor (MFF) will also apply, taking into account the differences in fixed costs between providers (analogous to ‘London weighting’), though this is provided directly to Trusts for all PBR activity and so does not affect the transaction directly. HRG E11 - non-elective spell = £4,787 2 extra £183 =£366 Total charged to PCT =£5,153
 is calculated (by software applications) based on lists which map HRGs to tariff prices. The tariff for HRG D22 is listed as £1108 for an elective spell or £1,166 for a non-elective (emergency) spell. (See table 2 ). The length of stay was 3 days. Had this exceeded 11 days, then ‘trim points’ would have been applied, with an additional £196 per day being applied to the tariff. (The length of stay above which trim points are applied is specific to HRGs). Similarly, if the length of the emergency stay had been less than 2 days, the short stay tariff of £398 would have applied. For this patient the PCT will pay £1,138. A market forces factor (MFF) will also apply, taking into account the differences in fixed costs between providers (analogous to ‘London weighting’), though this is provided directly to Trusts for all PBR activity and so does not affect the transaction directly. HRG E11 - non-elective spell = £4, extra £183 =£366. Total charged to PCT =£5,153.")
19
PBR PBR The tariff covers EVERYTHING that happens to the patient whilst in hospital (drugs, tests etc) Overseas PBR has stimulated primary care prescribing (in order to prevent expensive hospital tariffs) Overseas PBR has threatened secondary care prescribing (the hospital earns the same amount regardless of which drug they use) UNLESS the drug reduces length of stay Birth of real pharmaco economics in UK?
 Overseas PBR has threatened secondary care prescribing (the hospital earns the same amount regardless of which drug they use) UNLESS the drug reduces length of stay. Birth of real pharmaco economics in UK")
20
PBC Fund holding DID change how many patients went into hospital (unlike HAs, PCTs, and other NHS changes) (Ref Health Foundation, Oct 04) PBC born in England only (April ’05) and voluntary Resuscitated in April ’06 through the GMS contract
 and voluntary. Resuscitated in April ’06 through the GMS contract.")
21
PBC efficiency gains Practices meant to keep at least 70% of any freed up resources This wasn’t happening so BMA said don’t do PBC UNLESS you get a written agreement (HSJ 19th April 07, P8). Resources freed up may be spent on: Equipment; Training, clinical and non-clinical staff; Premises development with specific PCT board approval; Freed up resources can be shared across a wider group of practices Resources freed up must be used to fund services for the benefit of patients locally. Resources freed up may be spent on: Equipment; training, clinical and non-clinical staff; Premises development with specific PCT board approval; Freed up resources can be shared across a wider group of practices. Ref: Practice Based Commissioning: achieving universal coverage. London Jan 06. Practice Based Commissioning: achieving universal coverage Jan 06
. Resources freed up may be spent on: Equipment; Training, clinical and non-clinical staff; Premises development with specific PCT board approval; Freed up resources can be shared across a wider group of practices. Resources freed up must be used to fund services for the benefit of patients locally. Resources freed up may be spent on: Equipment; training, clinical and non-clinical staff; Premises development with specific PCT board approval; Freed up resources can be shared across a wider group of practices. Ref: Practice Based Commissioning: achieving universal coverage. London Jan 06. Practice Based Commissioning: achieving universal coverage Jan 06.")
22
PBC Currently – results aren’t great
Audit Commission said: “We’ve not yet seen any real evidence of it (PBC) leading to the redesign and transformation of services that was hoped”. They blame PCTs and the way they have set PBC budgets. (Ref HSJ 22 Nov ’07, P 7). However PBC is here for medium term at least NHS to use private firms to assist PC clusters with business cases (Ref HSJ 24 July 08, P 6)
 leading to the redesign and transformation of services that was hoped . They blame PCTs and the way they have set PBC budgets. (Ref HSJ 22 Nov ’07, P 7). However PBC is here for medium term at least. NHS to use private firms to assist PC clusters with business cases (Ref HSJ 24 July 08, P 6)")
23
World Class Commissioning
“Adding life to years and years to life”. Commissioning Assurance Handbook, dated 4 June PCTs will be assessed against three elements – Outcomes, Competencies and Governance. PCTs need to complete a self assessment and submit materials by end October 2008. PCTs to be ranked from 1 to 5 (5 = a WCC)
")
24
DARZI-Polyclinics Each PCT in England must have a new Polyclinic
Also over 100 new GP practices in “under-doctored” PCTs (mainly NE and NW England) Contracts will be awarded Dec ‘08 Real reason for doing this is to introduce some fat into the fire of change Many private companies bidding including Virgin, United Healthcare, BUPA. Virgin have had expressions of interest from 300 GP practices, Ref HSJ 22 May 08, P 11 but have now PULLED out of opening GP surgeries (Ref GP 26th Sep 08)
 Contracts will be awarded Dec ‘08. Real reason for doing this is to introduce some fat into the fire of change. Many private companies bidding including Virgin, United Healthcare, BUPA. Virgin have had expressions of interest from 300 GP practices, Ref HSJ 22 May 08, P 11 but have now PULLED out of opening GP surgeries (Ref GP 26th Sep 08)")
25
DARZI - Polyclinics Set-up costs met by DOH - £250-800m.
Winners will develop new services funded by start-up monies in competition with existing practices Some existing practices may go bust Practices will increasingly work in groups with shared approaches to medicines management Practices won by United Health, Care UK, Virgin, will restrict access, employ GPs and look to widespread formularies and prescribing policies

26
Pharmacy White Paper (Green paper, White Paper, Bill, Legislation)
White paper proposes that pharmacies will: prescribe certain common medicines, be first port of call for minor ailments, saving every GP the equivalent of around one hour per day; provide support for people with long-term conditions; be able to screen for vascular disease and certain STDs, such as Chlamydia; work much more closely with hospitals to provide seamless care; play a bigger role in vaccination.

27
Pharmacy White Paper Let’s not forget:
Pharmacies currently only doing 85 MURs each (*allowed to do 400) (Ref PJ 2 Aug 08, P 121) Lots of previous false dawns for pharmacy PWSI announced 2 years ago but only 2 (yes 2) in England
 (Ref PJ 2 Aug 08, P 121) Lots of previous false dawns for pharmacy. PWSI announced 2 years ago but only 2 (yes 2) in England.")
28
Some things are obvious

29
PCO LEVERS PCOs are proven to influence prescribing
National audit office survey of 2,000 GPs in ’07 Atorvastatin + Losartan in decline Prescribing incentive scheme is main lever PCOs reserve powerful levers for top priorities (normally big cost savings)
")
30
PCO LEVERS Prescribing incentive schemes Practice support pharmacists
5* lever, only for big savings (e.g. statins, sartans, antidepressants etc) Practice support pharmacists 5* lever, only for big savings ScriptSwitch 3* lever, smaller cost savings and quality issues Monthly Rx newsletters/Guidelines etc 2* lever, reinforce others Guidelines 1* lever, let someone else waste time on these
 Practice support pharmacists. 5* lever, only for big savings. ScriptSwitch. 3* lever, smaller cost savings and quality issues. Monthly Rx newsletters/Guidelines etc. 2* lever, reinforce others. Guidelines. 1* lever, let someone else waste time on these.")
31
NOEL J STAUNTON (BSc, MRPharmS, MBA, Dip H.Econ)
Pharmaceutical Consultant-3i consultancy ltd Work with Pharma companies (Pfizer, GSK, BI, Novartis, Flynn, Shire, Galderma, Stiefel, Solvay, Takeda, Lundbeck etc, etc) Mob E mail
 Mob E mail")
Similar presentations