Download presentation
Presentation is loading. Please wait.

2
A Year 2010 Milestone Summit
New Frontiers and Evolving Paradigms in Cancer and Thrombosis Optimizing Prevention, Risk Assessment, and Management of Thrombotic Complications in Malignancy: What Do the Trials Teach Us? How Should the Science Guide Us? Program Chairman Samuel Z. Goldhaber, MD Cardiovascular Division Brigham and Women’s Hospital Professor of Medicine Harvard Medical School

3
Program Faculty Program Chairman Alok A. Khorana, MD, FACP
Samuel Z. Goldhaber, MD Cardiovascular Division Brigham and Women’s Hospital Professor of Medicine Harvard Medical School Craig Kessler, MD Department of Hematology Anticoagulation Services Georgetown University Medical Center Washington, DC Alok A. Khorana, MD, FACP Vice-Chief, Division of Hematology/Oncology Associate Professor of Medicine and Oncology James P. Wilmot Cancer Center University of Rochester Rochester, NY Frederick R. Rickles, MD Clinical Professor of Medicine, Pediatrics, Pharmacology and Physiology Division of Hematology-Oncology Department of Medicine The George Washington University School of Medicine and Health Sciences Washington, DC

4
Program Agenda 8:15 PM — 8:30 PM Program Chairman’s Concluding Vision Statement: Current and Near Future Perspectives of VTE Management in the Setting of Malignancy Translating Scientific Advances into Clinical Practice Program Chairman Samuel Z. Goldhaber, MD Cardiovascular Division │ Brigham and Women’s Hospital │ Professor of Medicine │ Harvard Medical School 8:30 PM — 8:45 PM Interactive Q&A and Discussion Session 4

5
Disclosures Research Support BMS; Boehringer-Ingelheim; Eisai; Johnson & Johnson, Sanofi-Aventis Consultant Boehringer-Ingelheim; BMS; Eisai; EKOS: Medscape; Merck; Pfizer; Sanofi-Aventis

6
A Year 2010 Milestone Summit
New Frontiers and Evolving Paradigms in Cancer And Thrombosis Epidemiology, Trials, Guidelines Program Chairman Samuel Z. Goldhaber, MD Cardiovascular Division Brigham and Women’s Hospital Professor of Medicine Harvard Medical School

7
New Frontiers and Evolving Paradigms in Cancer and Thrombosis
Epidemiology

8
As Number of Cancer Survivors Increase, VTE Rates Increase
Stein PD, et al. Am J Med 2006; 119: 60-68

9
VTE Risk and Cancer Type: “Solid and Liquid”
Relative Risk of VTE Ranged From 1.02 to 4.34 4.5 4 3.5 3 2.5 2 1.5 1 0.5 Pancreas Brain Myeloprol Stomach Lymphoma Uterus Lung Esophagus Prostate Rectal Kidney Colon Ovary Liver Leukemia Breast Cervix Bladder Relative Risk of VTE in Cancer Patients Stein PD, et al. Am J Med 2006; 119: 60-68

10
Rate of PE Diagnosis is Increasing in the USA
250,000 200,000 150,000 100,000 50,000 229,637 Total cohort Surgical patients Non-surgical patients 163,096 126,546 90,468 66,541 36,078 CHEST 2009; 136:

11
Hospital Costs are Skyrocketing
CHEST 2009; 136:

12
DVT: Ominous Sequellae
30% recur over 10 years (after anticoagulation is discontinued) More than ½ of DVTs result in chronic venous insufficiency Leads to PE, potentially fatal 1% to 4% of PEs evolve chronic thromboembolic pulmonary hypertension (CTEPH)
 More than ½ of DVTs result in chronic venous insufficiency. Leads to PE, potentially fatal. 1% to 4% of PEs evolve chronic thromboembolic pulmonary hypertension (CTEPH)")
13
Recurrent VTE is Common After A First Episode of Symptomatic DVT
355 patients followed for 8 years 1 2 3 4 5 6 7 8 10 15 20 25 30 Cumulative Incidence (%) Years Prandoni et al, Ann Intern Med 1996;125:1-7
 Years. Prandoni et al, Ann Intern Med 1996;125:1-7.")
14
Stages of Chronic Venous Insufficiency
Varicose veins Ankle/ leg edema Stasis dermatitis Lipodermatosclerosis Venous stasis ulcer

15
Chronic Venous Insufficiency
Progression of Chronic Venous Insufficiency From UpToDate 2006

16
U.S.A. SURGEON GENERAL: CALL TO ACTION TO PREVENT DVT AND PE September 15, 2008
100, ,000 Deaths/year in USA

17
CTEPH RECURRENT ACUTE PE
Figure 1. Pulmonary Thromboendarterectomy Specimen and Acute Pulmonary Thromboembolus. Panel A shows a whitish-yellow, fibrotic, organized thromboembolus with a thin layer of proximal red appositions, which formed a cast of the pulmonary arterial tree in a patient with CTPH. Image courtesy of Dr. Walter Klepetko. By way of contrast, Panel B shows fresh red thrombi that were recovered from a patient with acute pulmonary embolism. Lang, I. M. NEJM 2004;350:

18
5,451 patients enrolled prospectively
DVT FREE Registry 5,451 patients enrolled prospectively Consecutive acute DVT diagnosed by venous ultrasonography No exclusions 183 participating sites in the U.S. Goldhaber SZ, Tapson VF. Am J Cardiol 2004;93:

19
DVT FREE Registry (N=5,541): TOP 5 Medical Comorbidities
1. Hypertension 2. Immobility 3. Cancer 4. Obesity (BMI > 30) 5. Cigarette Smoking Am J Cardiol 2004; 93:
 5. Cigarette Smoking. Am J Cardiol 2004; 93:")
20
Primary Prevention Trials
New Frontiers and Evolving Paradigms in Cancer and Thrombosis Pivotal VTE Primary Prevention Trials

21
Trials of VTE Prophylaxis in Hospitalized Medical Patients
MEDENOX (enoxaparin 40 mg) Samama MM, et al. N Engl J Med. 1999;341: PREVENT (dalteparin 5000 IU) Leizorovicz A, et al. Circulation. 2004;110: ARTEMIS (fondaparinux 2.5 mg) Cohen AT, et al. BMJ 2006; 332: 325.
 Samama MM, et al. N Engl J Med. 1999;341: PREVENT (dalteparin 5000 IU) Leizorovicz A, et al. Circulation. 2004;110: ARTEMIS (fondaparinux 2.5 mg) Cohen AT, et al. BMJ 2006; 332: 325.")
22
PREVENT-Dalteparin Trial (N=3,681)
A multicenter, randomized, controlled study in acutely ill medical patients Compared the incidence in the dalteparin and placebo groups of: Any symptomatic VTE Asymptomatic proximal DVT Sudden death Circulation 2004; 110:

23
PREVENT Study Design (N=3,681)
Treatment period Follow-up period Dalteparin No study drug Randomization Placebo No study drug Day 14 Day 90 Day 21 Primary endpoint/ Bilateral leg U/S • Dalteparin 5000 Units SC once daily (12-14 d) • Placebo SC once daily (12-14 d)
 • Placebo SC once daily (12-14 d)")
24
Primary Efficacy Endpoint: VTE (Day 21)
Difference in Incidence (%) Risk Ratio Dalteparin N=1518 Placebo N=1473 42 2.77% 73 4.96% -2.19 0.55 -3.57 to -0.81 0.38 to 0.80 95% CI Analysis of the primary efficacy endpoint at Day 21 showed that compared with placebo, prophylactic treatment with dalteparin was associated with a clinically meaningful reduction in risk ratio of (45% decrease in the risk) of experiencing a symptomatic DVT (proximal or distal), nonsymptomatic proximal DVT and/or near fatal and fatal PE and sudden death. The incidence of events was 2.77%. Although the study was designed with an alpha of 0.001, the results provide strong statistical evidence of treatment effect (and reliable evidence that the null hypothesis can be rejected). Low probability that this is a chance finding. Single Studies P = Circulation 2004; 110:
 Risk. Ratio. Dalteparin. N=1518. Placebo. N= % % to to % CI. Analysis of the primary efficacy endpoint at Day 21 showed that compared with placebo, prophylactic treatment with dalteparin was associated with a clinically meaningful reduction in risk ratio of 0.55 (45% decrease in the risk) of experiencing a symptomatic DVT (proximal or distal), nonsymptomatic proximal DVT and/or near fatal and fatal PE and sudden death. The incidence of events was 2.77%. Although the study was designed with an alpha of 0.001, the results provide strong statistical evidence of treatment effect (and reliable evidence that the null hypothesis can be rejected). Low probability that this is a chance finding. Single Studies. P = Circulation 2004; 110:")
25
Dalteparin Benefit Similar Across Subgroups
Age Gender Cancer Obesity Previous DVT

26
Quality Improvement Initiative to Improve VTE Prophylaxis
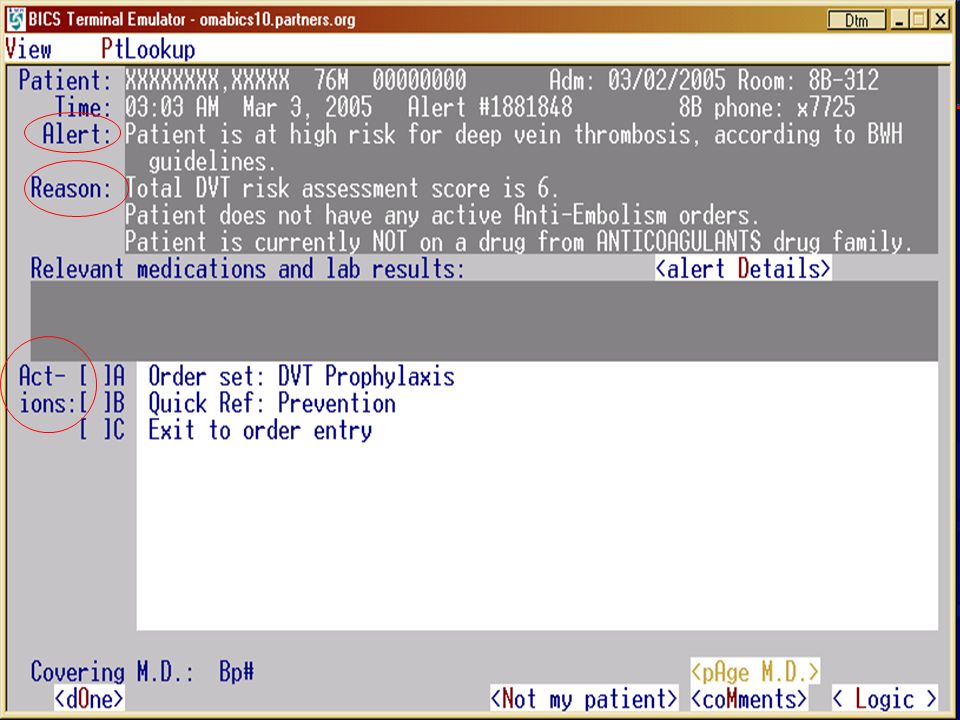
Randomized controlled trial to issue or withhold electronic alerts to MDs whose high-risk patients were not receiving VTE prophylaxis Kucher N et al. NEJM 2005; 352: 969

27
Computer Program We developed a computer program linked to the patient database that screened the system daily to identify high-risk patients. We included consecutive high-risk patients on medical and surgical services who were not receiving DVT prophylaxis. Kucher N et al. NEJM 2005; 352: 969

28
Definition: “High Risk”
VTE risk score ≥ 4 points: Cancer 3 (ICD codes) Prior VTE 3 (ICD codes) Hypercoagulability (Leiden, ACLA) Major surgery 2 (> 60 minutes) Bed rest 1 (“bed rest” order) Advanced age 1 (> 70 years) Obesity 1 (BMI > 29 kg/m2) HRT/OC 1 (order entry)
 Prior VTE 3 (ICD codes) Hypercoagulability 3 (Leiden, ACLA) Major surgery 2 (> 60 minutes) Bed rest 1 ( bed rest order) Advanced age 1 (> 70 years) Obesity 1 (BMI > 29 kg/m2) HRT/OC 1 (order entry)")
29
Randomization VTE risk score > 4 No prophylaxis N = 2,506
INTERVENTION: Single alert N = 1,255 CONTROL No computer alert N = 1,251 Kucher N, et al. NEJM 2005;352:

31
Baseline Characteristics
Median age: years Medical services: 83% Surgical services: 17% Comorbidities Cancer: 80% Hypertension: 34% Infection: 30% Prior VTE: % Kucher N, et al. NEJM 2005;352:

32
Primary End Point Intervention Control 100 98 96 94 92 90 30 60 90
%Freedom from DVT/ PE 94 Control 92 90 30 60 90 Time (days) Number at risk Intervention 1255 977 900 853 Control 1251 976 893 839 Kucher N, et al. NEJM 2005;352:
 Number at risk. Intervention Control Kucher N, et al. NEJM 2005;352:")
33
Pivotal VTE Treatment Trial in Patients with Cancer
New Frontiers and Evolving Paradigms in Cancer and Thrombosis Pivotal VTE Treatment Trial in Patients with Cancer

34
LMWH Monotherapy halves recurrence, compared with warfarin.
Cancer and VTE 3-fold higher recurrence and bleeding, when treating cancer patients (Prandoni. Blood 2002; 100: 3484) LMWH Monotherapy halves recurrence, compared with warfarin. FDA approved May 2007 Lee AYY. NEJM 2003; 349:146
 LMWH Monotherapy halves recurrence, compared with warfarin. FDA approved May Lee AYY. NEJM 2003; 349:146.")
35
Dalteparin dose: 200 u/kg daily 1st month, then 150 u/kg daily.
“CLOT Trial” Dalteparin monotherapy for 6 months was more effective (8.8% vs. 17% recurrence) than warfarin in 672 cancer patients with DVT. Dalteparin dose: 200 u/kg daily 1st month, then 150 u/kg daily. Agnes Lee, et al. NEJM 2003; 349: )
 than warfarin in 672 cancer patients with DVT. Dalteparin dose: 200 u/kg daily 1st month, then 150 u/kg daily. Agnes Lee, et al. NEJM 2003; 349: )")
36
Dalteparin Reduces VTE Recurrence in Cancer Patients (N = 676)
CLOT TRIAL NEJM 2003; 349:

37
Cancer patients with DVT/PE
LMWH Monotherapy Cancer patients with DVT/PE Any patient who fails warfarin (has recurrent DVT/PE) despite target INR Difficulty maintaining target INR Poor GI absorption of meds Alopecia or rash from Coumadin “Bridging”
 despite target INR. Difficulty maintaining target INR. Poor GI absorption of meds. Alopecia or rash from Coumadin. Bridging")
38
ACCP VTE Rx in Cancer: Guidelines 8th Edition
At least 3 months of LMWH. Then administer LMWH or warfarin as long as the cancer is active. Indefinite duration anticoagulation after 2nd unprovoked VTE. CHEST 2008; 133: 454S

39
Cancer and VTE are closely linked.
Conclusions Cancer and VTE are closely linked. Cancer increases VTE risk and may be occult when VTE is diagnosed. Cancer patients are at high risk for VTE but receive less prophylaxis than any other at-risk group of hospitalized patients. Dalteparin 5,000 U/d is effective for VTE prophylaxis in cancer patients.

40
Conclusions (Continued)
Dalteparin 200 U/kg/day is effective for treatment of acute VTE as monotherapy without warfarin. NCCN, ASCO, and ACCP guidelines endorse VTE prevention with LMWH and VTE treatment of cancer patients with LMWH alone (monotherapy without warfarin).
.")
41
The Role of the Coagulation Cascade in Malignant Transformation
New Frontiers and Evolving Paradigms in Cancer and Thrombosis The Role of the Coagulation Cascade in Malignant Transformation Can Anticoagulation Affect Cancer Survival? Frederick R. Rickles, MD Professor of Medicine, Pediatrics, Pharmacology and Physiology The George Washington University Washington, DC

42
Disclosures Consultant Genmab, Bayer/Ortho‐McNeil/J & J, Pharmacyclics, Leo Speaker’s Bureau Eisai

43
Interface of Coagulation and Cancer
Fibrinolytic activities: t-PA, u-PA, u-PAR, PAI-1, PAI-2 Procoagulant Activities FIBRIN Endothelial cells IL-1, TNF-a, VEGF Tumor cells Monocyte PMN leukocyte Activation of coagulation Platelets Angiogenesis, Basement matrix degradation. TF-rich MPs Falanga and Rickles, New Oncology:Thrombosis, 2005; Hematology, ASH Education Book, 2007

44
Mechanisms of Cancer-Induced Thrombosis: Clot and Cancer Interface
Pathogenesis? Biological significance? Anticoagulation and cancer survival?

45
Activation of Blood Coagulation in Cancer Biological Significance?
Epiphenomenon? Is this a generic secondary event where thrombosis is an incidental finding or, is clotting activation . . . A Primary Event? Linked to malignant transformation

46
Interface of Clotting Activation
and Tumor Biology FVII/FVIIa TF Blood Coagulation Activation Tumor Cell VEGF THROMBIN FIBRIN Angiogenesis IL-8 TF PAR-2 Endothelial cells Angiogenesis Falanga and Rickles, New Oncology:Thrombosis, 2005;1:9-16; Ruf. J Thromb Haemost 2007;5:1584

47
Coagulation Cascade and Tumor Biology
Clotting-dependent Clotting-dependent Fibrin TF Thrombin Xa VIIa Clotting-independent Clotting-independent Clotting-dependent PARs Angiogenesis, Tumor Growth and Metastasis Fernandez, Patierno and Rickles. Sem Hem Thromb 2004;30:31; Ruf. J Thromb Haemost 2007;5:1584

48
In Situ Localization of Tissue Factor in Vascular Endothelium of Human Lung Adenocarcinoma – co-localization with vWF Shoji et al, Amer J Pathol 1998;152:

49
In Situ localization of Tissue Factor in Tumor Vascular Endothelium in Invasive Human Breast Cancer
Contrino et al. Nature Med 1996;2:

50
In Situ Co-Localization of TF and VEGF mRNA in Lung Adenocarcinoma
H&E TF VEGF Shoji et al. Amer J Pathol 1998;152:

51
Human melanoma cell lines grown as xenogeneic tumors in SCID mice
TF high producer Human melanoma cell lines grown as xenogeneic tumors in SCID mice. RPMI-7951 melanoma cells (a high TF and VEGF producer) or WM-115 melanoma cells (a low TF and VEGF producer) were inoculated s.c. (3 × 106/mouse) on the same day. (A) The gross appearance of RPMI-7951 tumors was hemorrhagic, dark purplish in color, whereas the WM-115 tumors appeared pale and relatively avascular. The immunohistologic analysis of RPMI-7951 and WM-115 tumors from these SCID mice emphasized detection of VECs. (B) The RPMI-7951 tumor and (C) the WM-115 tumor were stained with rabbit anti-human von Willebrand factor, by using the standard immunoperoxidase method. The relative frequency of micro blood vessels is noted by arrow heads (magnifications: ×200 for B and C). The average number of blood vessels per a field for three RPMI-7951 tumors and five WM-115 tumors are 17.3 ± 4.0 (1 SD) and 3.2 ± 2.2, respectively. TF low producer Abe K et al. PNAS 1999;96: ©1999 by The National Academy of Sciences
 or WM-115 melanoma cells (a low TF and VEGF producer) were inoculated s.c. (3 × 106/mouse) on the same day. (A) The gross appearance of RPMI-7951 tumors was hemorrhagic, dark purplish in color, whereas the WM-115 tumors appeared pale and relatively avascular. The immunohistologic analysis of RPMI-7951 and WM-115 tumors from these SCID mice emphasized detection of VECs. (B) The RPMI-7951 tumor and (C) the WM-115 tumor were stained with rabbit anti-human von Willebrand factor, by using the standard immunoperoxidase method. The relative frequency of micro blood vessels is noted by arrow heads (magnifications: ×200 for B and C). The average number of blood vessels per a field for three RPMI-7951 tumors and five WM-115 tumors are 17.3 ± 4.0 (1 SD) and 3.2 ± 2.2, respectively. TF low producer. Abe K et al. PNAS 1999;96: ©1999 by The National Academy of Sciences.")
52
TF regulates VEGF expression in human cancer cell lines
Regulation of Vascular Endothelial Growth Factor Production and Angiogenesis by the Cytoplasmic Tail of Tissue Factor TF regulates VEGF expression in human cancer cell lines Human cancer cells with increased TF are more angiogenic (and, therefore, more “metastatic’) in vivo due to high VEGF production Abe et al Proc Nat Acad Sci 1999;96: ; Ruf et al Nature Med 2004;10:
 in vivo due to high VEGF production. Abe et al Proc Nat Acad Sci 1999;96: ; Ruf et al Nature Med 2004;10:")
53
Is this a paradigm shift?
Regulation of Vascular Endothelial Growth Factor Production and Angiogenesis by the Cytoplasmic Tail of Tissue Factor The cytoplasmic tail of TF, which contains three serine residues, appears to play a role in regulating VEGF expression in human cancer cells, perhaps by mediating signal transduction Thisa and other data on signaling pathways activated by TF/VIIa engagement of PAR-2b and/or thrombin engagement of PAR-1c suggest that clotting pathways are directly involved in regulating tumor growth, angiogenesis and metastasis Is this a paradigm shift? a Abe et al Proc Nat Acad Sci 1999;96: b Ruf et al Nature Med 2004;10:502-9 c Karpatkin et al Cancer Res 2009;69:

54
Activation of Blood Coagulation in Cancer and Malignant Transformation
Epiphenomenon vs. Malignant Transformation? Paradigm Shift (2005) 1. MET oncogene induction produces DIC in human liver carcinoma (Boccaccio lab) (Boccaccio et al Nature 2005;434: ) 2. Pten loss and EGFR amplification produce TF activation and pseudopalisading necrosis through JunD/Activator Protein-1 in human glioblastoma (Bratt lab) (Rong et al Cancer Res 2005;65: ; Cancer Res 2009;69:2540-9) 3. K-ras oncogene, p53 inactivation and TF induction in human colorectal carcinoma; TF and angiogenesis regulation in epithelial tumors by EGFR (ErbB1) – relationship to EMTs (Rak lab) (Yu et al Blood 2005;105: ; Milson et al Cancer Res 2008;68: )
 1. MET oncogene induction produces DIC in human liver carcinoma (Boccaccio lab) (Boccaccio et al Nature 2005;434: ) 2. Pten loss and EGFR amplification produce TF activation and pseudopalisading necrosis through JunD/Activator Protein-1 in human glioblastoma. (Bratt lab) (Rong et al Cancer Res 2005;65: ; Cancer Res 2009;69:2540-9) 3. K-ras oncogene, p53 inactivation and TF induction in human colorectal carcinoma; TF and angiogenesis regulation in epithelial tumors by EGFR (ErbB1) – relationship to EMTs (Rak lab) (Yu et al Blood 2005;105: ; Milson et al Cancer Res 2008;68: )")
55
Activation of Blood Coagulation in Cancer: Malignant Transformation
“1. MET Oncogene Drives a Genetic Programme Linking Cancer to Haemostasis” MET encodes a tyrosine kinase receptor for hepatocyte growth factor/scatter factor (HGF/SF) Drives physiological cellular program of “invasive growth” (tissue morphogenesis, angiogenesis and repair) Aberrant execution (e.g. hypoxia-induced transcription) is associated with neoplastic transformation, invasion, and metastasis Boccaccio et al Nature 2005;434:
 Drives physiological cellular program of invasive growth (tissue morphogenesis, angiogenesis and repair) Aberrant execution (e.g. hypoxia-induced transcription) is associated with neoplastic transformation, invasion, and metastasis. Boccaccio et al Nature 2005;434:")
56
Activation of Blood Coagulation in Cancer: Malignant Transformation
2. “Pten and Hypoxia Regulate Tissue Factor Expression and Plasma Coagulation By Glioblastoma” Pten = tumor suppressor with lipid and protein phosphatase activity Loss or inactivation of Pten (70-80% of glioblastomas) leads to Akt activation and upregulation of Ras/MEK/ERK signaling cascade Rong et al Ca Res 2005;65:
 leads to Akt activation and upregulation of Ras/MEK/ERK signaling cascade. Rong et al Ca Res 2005;65:")
57
“Pten and Hypoxia Regulate Tissue Factor Expression and Plasma Coagulation By Glioblastoma”
Glioblastomas characterized histologically by “pseudopalisading necrosis” Thought to be wave of tumor cells migrating away from a central hypoxic zone, perhaps created by thrombosis Pseudopalisading cells produce VEGF and IL-8 and drive angiogenesis and rapid tumor growth TF expressed by >90% of grade 3 and 4 malignant astrocytomas (but only 10% of grades 1 and 2)
")
58
“Pten and Hypoxia Regulate Tissue Factor Expression and Plasma Coagulation By Glioblastoma”
Results: Hypoxia and PTEN loss TF (mRNA, Ag and procoagulant activity); partially reversed with induction of PTEN Both Akt and Ras pathways modulated TF in sequentially transformed astrocytes. 3. Ex vivo data: TF (by IH-chemical staining) in pseudopalisades of # 7 human glioblastoma specimens
; partially reversed with induction of PTEN. Both Akt and Ras pathways modulated TF in sequentially transformed astrocytes. 3. Ex vivo data: TF (by IH-chemical staining) in pseudopalisades of # 7 human glioblastoma specimens.")
59
“Pten and Hypoxia Regulate Tissue Factor Expression and Plasma Coagulation By Glioblastoma”
Pseudopalisading necrosis H&E TF IHC Vascular Endothelium

60
Activation of Blood Coagulation in Cancer: Malignant Transformation
3. “Oncogenic Events Regulate Tissue Factor Expression In Colorectal Cancer Cells: Implications For Tumor Progression And Angiogenesis” Activation of K-ras oncogene and inactivation of p53 tumor suppressor TF expression in human colorectal cancer cells Transforming events dependent on MEK/MAPK and PI3K Cell-associated and MP-associated TF activity linked to genetic status of cancer cells TF siRNA reduced cell surface TF expression, tumor growth and angiogenesis TF may be required for K-ras-driven phenotype Yu et al Blood 2005;105:

61
Activation of Blood Coagulation in Cancer: Malignant Transformation
“Oncogenic Events Regulate Tissue Factor Expression In Colorectal Cancer Cells: Implications For Tumor Progression And Angiogenesis” Effect of TF si mRNA on tumor growth in vitro and in vivo Yu et al Blood 2005;105:

62
Activation of Blood Coagulation in Cancer: Malignant Transformation
“Oncogenic Events Regulate Tissue Factor Expression In Colorectal Cancer Cells: Implications For Tumor Progression And Angiogenesis” Matrigel Assay: (D) HCT 116; (E) SI-3 cells – vWF immunohistology Similar amplification of TF with upregulated VEGF induced by mutated EGFR in glioblastoma and lung cancer cells; accompanied by epithelial-to-mesenchymal transition (EMT) Milsom et al CA Res 2008;68: Yu et al Blood 2005;105:
 HCT 116; (E) SI-3 cells – vWF immunohistology. Similar amplification of TF with upregulated VEGF induced by mutated EGFR in glioblastoma and lung cancer cells; accompanied by epithelial-to-mesenchymal transition (EMT) Milsom et al CA Res 2008;68: Yu et al Blood 2005;105:")
63
Microparticles Originate directly from membrane surface of activated or apoptotic cell Express surface antigens derived from parent cell Anucleate <1 µm in diameter Procoagulant activity mediated by TF and/or PS Upon cellular activation, calcium is released from the endoplasmic reticulum. Calcium inactivates flippase and activates floppase and scramblase. This induces a loss of phospholipid asymmetry between the inner and outer leaflets of the membrane. Calcium also activates calpain which hydrolyzes actin binding proteins, severing the bilayer from the cytoskeleton. Burnier L et al. Thromb Haemost 2009;101: 63

64
Cumulative incidence of VTE in cancer patients with (--) /without ( ) circulating TF-bearing microparticles Zwicker et al. Clin Cancer Res 2009;15: 64

65
Microparticle TF PCA in Cancer Patients ± VTE
Manly DA, et al. Thromb Res 2010;125: 65

66
Activation of Blood Coagulation in Cancer: Malignant Transformation
Q: What do these experiments tell us? A: They suggest two things: Tumor cell-derived, TF-rich microparticles (MPs) may be important as a predictive test for VTE All patients with oncogene-driven cancer may need prophylactic anticoagulation
 may be important as a predictive test for VTE. All patients with oncogene-driven cancer may need prophylactic anticoagulation.")
67
Mechanisms of Cancer-Induced Thrombosis: Implications
Pathogenesis? Biological significance? Anticoagulation and cancer survival ?

68
Anticoagulants and Survival
Inconclusive evidence to date Experimental data supportive of antitumor effects but exact mechanisms not established Clinical trials provide supportive data for LMWH but are heterogeneous in design and methodology: Tumour types Stage or course of disease Treatment history or concurrent cancer therapies LMWH agents Doses and regimens of LMWHs A Lee ICTHIC, 2010

69
Survival Effect of Anticoagulants
Kuderer N et al. Cancer 2007;110:

70
PROTECHT Study Multicentre, double-blind, placebo-controlled RCT
Advanced lung, breast, GI, pancreas, ovary, H+N Nadroparin vs placebo for duration of chemo (up to 4m) Nadroparin Placebo P-value NNT/H No. Patients 769 381 1° endpoint: VTE + ATE 2.0% 3.9% 0.02* 54 Major bleeding 0.7% 0.18 154 Death 4.3% 4.2% 1-yr mortality 43% 41% *1-sided Agnelli et al. Lancet 2009;10:
 Nadroparin. Placebo. P-value. NNT/H. No. Patients ° endpoint: VTE + ATE. 2.0% 3.9% 0.02* 54. Major bleeding. 0.7% Death. 4.3% 4.2% 1-yr mortality. 43% 41% *1-sided. Agnelli et al. Lancet 2009;10:")
71
Prophylaxis in Pancreatic Cancer
CONKO FRAGEM P<0.02 P<0.01 No survival difference P=0.6 P=0.03 NS VTE bleeding VTE fatal PE Gr 3 bleed Riess et al. ASCO May 2009 and ISTH July Maraveyas et al. Presented at ESMO 2009.

72
Year 2010 State-of-the-Science Update
Cancer and Thrombosis Year 2010 State-of-the-Science Update Key Questions 1. Does activation of blood coagulation affect the biology of cancer positively or negatively? 2. Can we treat tumors more effectively using coagulation protein targets? 3. Can anticoagulation alter the biology of cancer?

73
Year 2010 State-of-the-Science Update
Cancer and Thrombosis Year 2010 State-of-the-Science Update Tentative Answers 1. Epidemiologic evidence is suggestive that VTE is a bad prognostic sign in cancer 2. Experimental evidence is supportive of the use of antithrombotic strategies for both prevention of thrombosis and inhibition of tumor growth 3. Results of recent, randomized clinical trials of LMWHs in cancer patients indicate superiority to oral agents in preventing recurrent VTE; increasing survival (not due to prevention of VTE) not clear
 not clear.")
74
LMWH in Cancer Survival Studies INPACT (NSCLC, prostate, pancreatic)
nadroparin + chemo vs. chemo ABEL (limited SCLC) bemiparin + chemo vs. chemo TILT (nonsmall cell lung cancer) tinzaparin + chemo vs chemo FRAGMATIC (newly diagnosed lung cancer) dalteparin + chemo vs chemo Stay tuned ! A Lee ICTHIC, 2010
 bemiparin + chemo vs. chemo. TILT (nonsmall cell lung cancer) tinzaparin + chemo vs chemo. FRAGMATIC (newly diagnosed lung cancer) dalteparin + chemo vs chemo. Stay tuned ! A Lee ICTHIC,")
75
New Frontiers and Evolving Paradigms in Cancer and Thrombosis
Optimizing Risk Assessment and Management of Cancer Patients at Risk for Venous Thromboembolism (VTE) Reducing DVT Recurrence and Related Complications Craig Kessler, MD Professor of Medicine Department of Hematology Anticoagulation Services Georgetown University Medical Center Washington, DC
 Reducing DVT Recurrence and Related Complications. Craig Kessler, MD. Professor of Medicine. Department of Hematology. Anticoagulation Services. Georgetown University Medical Center. Washington, DC.")
76
COI Financial Disclosures
Grant/Research Support: GlaxoSmithKline, sanofi-aventis, Eisai Consultant: sanofi-aventis, Eisai

77
Guidelines for VTE prevention in cancer patients
Outline Guidelines for VTE prevention in cancer patients Opportunities for improvement Guidelines for VTE Treatment LMWHs—What Do the Trials, NCCN and ASCO Guidelines Teach Us About Duration of Therapy and Patients at Risk?

78
ASCO Clinical Practice Guideline
Recommendations for Venous Thromboembolism Prophylaxis and Treatment in Patients with Cancer ASCO Clinical Practice Guideline NCCN Clinical Practice Guidelines in Oncology™ Guidelines for supportive care “…the panel of experts includes a medical and surgical oncologists, hematologists, cardiologists, internists, radiologists. And a pharmacist.”

79
Importance of Guidelines to Clinical Outcomes
“Clinicians armed with appropriate assessments and the best evidence-based practice guidelines can reduce some of the unpleasant and frequent side-effects that often accompany cancer and chemotherapy treatment, obtain the best possible clinical outcomes, and avoid unnecessary costs.” Statement from Centers for Medicare and Medicaid Services, August 2005 CMS, the Centers for Medicare and Medicaid Services

80
Incidence of VTE in US Patients with Cancer
Rate Has Risen Although the Overall Incidence of Cancer Has Not Changed [Stein.AmJMed. Jan.2006/ p62/c2/Figure 1] Highest incidence of VTE: pancreatic CA (4.3%) Lowest incidence of VTE: oral cavity, or pharynx This graph shows clearly that since the late 1980s, the incidence of venous thromboembolism (VTE) in patients with cancer has risen dramatically, from approximately 1.5% to greater than 3.5%, even as the incidence of cancers, overall, has remained relatively steady1 The graph is based on an analysis of the National Hospital Discharge Survey on the numbers of patients discharged with a diagnostic code for 19 types of malignancies, pulmonary embolism (PE), or deep vein thrombosis (DVT) from 1979 through 19991 Overall, in patients with any of the 19 malignancies covered, 827,000 of 40,787,000 (2.0%) had VTE, which was twice the incidence in patients without these malignancies, 6,854,000 of 662,309,000 (1.0%)1 The highest incidence of VTE was in patients with carcinoma of the pancreas (4.3%), and the lowest incidences were in patients with carcinoma of the bladder and carcinoma of the lip, oral cavity, or pharynx1 The overall incidences of PE and DVT in patients with cancer were double the rates in patients without cancer and were not age dependent1 [1/Stein.AmJMed. Jan.2006/ p62/c2/Figure 1] [1/Stein/p61/c1/ line 45-55, c2/line 15-50; p62/c1/line 1-6, Table; p63/c1/line 4-9] [1/Stein/ p63/c1/line 3-20] [1/Stein/ p64/c2/line 22-27; p63/c1/line 1-6] [1/Stein/ p60/line A15-A18] National Hospital Discharge Survey data from 19 types of malignancies from 1979 through 1999 (non-age dependent) Stein PD et al. Am J Med. 2006;119:60-68. Overall, in patients with any of the 19 malignancies covered, 827,000 of 40,787,000 (2.0%) had VTE, which was twice the incidence in patients without these malignancies, 6,854,000 of 662,309,000 (1.0%)1 The highest incidence of VTE was in patients with carcinoma of the pancreas (4.3%), and the lowest incidences were in patients with carcinoma of the bladder and carcinoma of the lip, oral cavity, or pharynx1 The overall incidences of PE and DVT in patients with cancer were double the rates in patients without cancer and were not age dependent1 1. Stein PD, Beemath A, Meyers FA, Skaf E, Sanchez J, Olson RE. Incidence of venous thromboembolism in patients hospitalized with cancer. Am J Med. 2006;119:60-68.
 Lowest incidence of VTE: oral cavity, or pharynx. This graph shows clearly that since the late 1980s, the incidence of venous thromboembolism (VTE) in patients with cancer has risen dramatically, from approximately 1.5% to greater than 3.5%, even as the incidence of cancers, overall, has remained relatively steady1. The graph is based on an analysis of the National Hospital Discharge Survey on the numbers of patients discharged with a diagnostic code for 19 types of malignancies, pulmonary embolism (PE), or deep vein thrombosis (DVT) from 1979 through Overall, in patients with any of the 19 malignancies covered, 827,000 of 40,787,000 (2.0%) had VTE, which was twice the incidence in patients without these malignancies, 6,854,000 of 662,309,000 (1.0%)1. The highest incidence of VTE was in patients with carcinoma of the pancreas (4.3%), and the lowest incidences were in patients with carcinoma of the bladder and carcinoma of the lip, oral cavity, or pharynx1. The overall incidences of PE and DVT in patients with cancer were double the rates in patients without cancer and were not age dependent1. [1/Stein.AmJMed. Jan.2006/ p62/c2/Figure 1] [1/Stein/p61/c1/ line 45-55, c2/line 15-50; p62/c1/line 1-6, Table; p63/c1/line 4-9] [1/Stein/ p63/c1/line 3-20] [1/Stein/ p64/c2/line 22-27; p63/c1/line 1-6] [1/Stein/ p60/line A15-A18] National Hospital Discharge Survey data from 19 types of malignancies from 1979 through 1999 (non-age dependent) Stein PD et al. Am J Med. 2006;119: Overall, in patients with any of the 19 malignancies covered, 827,000 of 40,787,000 (2.0%) had VTE, which was twice the incidence in patients without these malignancies, 6,854,000 of 662,309,000 (1.0%)1. The highest incidence of VTE was in patients with carcinoma of the pancreas (4.3%), and the lowest incidences were in patients with carcinoma of the bladder and carcinoma of the lip, oral cavity, or pharynx1. The overall incidences of PE and DVT in patients with cancer were double the rates in patients without cancer and were not age dependent1. 1. Stein PD, Beemath A, Meyers FA, Skaf E, Sanchez J, Olson RE. Incidence of venous thromboembolism in patients hospitalized with cancer. Am J Med. 2006;119:")
81
Venous Thromboembolism in Cancer Patients
Of all cases of VTE: 20% occur in cancer patients Of all cancer patients: 0.5% will have symptomatic VTE As high as 50% have VTE at autopsy Compared to patients without cancer: Higher risk of first and recurrent VTE Higher risk of bleeding on anticoagulants Higher risk of dying VTE may be the presenting sign of occult malignancy 10% with idiopathic VTE develop cancer within 2 years 20% have recurrent idiopathic VTE 25% have bilateral DVT Lee & Levine. Circulation 2003;107:I17 – I21; Bura et. al., J Thromb Haemost 2004;2:445-51

82
Thrombosis and Survival: Likelihood of Death After Hospitalization
0.00 0.20 0.40 1.00 0.80 0.60 DVT/PE and Malignant Disease Malignant Disease DVT/PE Only Nonmalignant Disease Number of Days Probability of Death Levitan N, et al. Medicine 1999;78:285

83
Cancer and Venous Thromboembolism The Need for Risk Stratification
0.5 1 1.5 2 2.5 3 3.5 4 4.5 5 6 Diagnosis Chemotherapy Hospitalization Remission End of Life Metastasis Relative Risk Average Risk Time

84
VTE in Hospitalized Cancer Patients
7.0 VTE patients on chemotherapy VTE all patients 6.0 DVT all patients PE all patients 5.0 4.0 Rate of VTE (%) 3.0 2.0 1.0 0.0 1995 1996 1997 1998 1999 2000 2001 2002 2003 Years Cancer 2007 84
 Years. Cancer")
85
Effect of Malignancy on Risk of VTE
Population-based case-control (MEGA) study N=3220 consecutive patients with 1st VTE vs. n=2131 control subjects CA patients = OR 7x VTE risk vs. non-CA patients 10 20 30 40 50 Hematological Lung Gastrointestinal Breast Distant metastases 0 to 3 months 3 to 12 months 1 to 3 years 5 to 10 years > 15 years 28 22.2 20.3 4.9 19.8 53.5 14.3 2.6 1.1 3.6 Type of cancer Time since cancer diagnosis Adjusted odds ratio MEGA = Multiple Environmental and Genetic Assessment case- control study VTE = venous thromboembolism; CA = cancer; OR = odds ratio. Silver In: The Hematologist - modified from Blom JW, et. al. JAMA. 2005;293: 85
 study. N=3220 consecutive patients with 1st VTE vs. n=2131 control subjects. CA patients = OR 7x VTE risk vs. non-CA patients Hematological. Lung. Gastrointestinal. Breast. Distant. metastases. 0 to 3 months. 3 to 12 months. 1 to 3 years. 5 to 10 years. > 15 years Type of cancer. Time since cancer diagnosis. Adjusted odds ratio. MEGA = Multiple Environmental. and Genetic Assessment case- control study. VTE = venous thromboembolism; CA = cancer; OR = odds ratio. Silver In: The Hematologist - modified from Blom JW, et. al. JAMA. 2005;293:")
86
"Meeting the Challenges of VTV: Strategies for Implementing Guideline-based Recommendations"
The Importance of DVT Prophylaxis in Patients With Cancer: ASCO Guidelines VTE is a leading causes of death in CA, occurring in 4% to 20% patients Hospitalized CA pt and those on chemo tx have greatest VTE risk Cancer increased the risk of VTE 4.1-fold Chemotherapy increased the risk 6.5-fold Major risk factors: older age, comorbid conditions, recent surgery or hospitalization, active chemotherapy or hormonal therapy All hospitalized CA patients should be considered for prophylaxis Patients with cancer undergoing surgery should be considered for prophylaxis LMWH is the preferred drug The American Society of Clinical Oncology (ASCO) issued guidelines for prophylaxis and treatment of VTE in cancer patients. Among the recommendations are that all cancer patients who are hospitalized or are undergoing cancer surgery should be considered for prophylaxis, and the preferred drug is low-molecular-weight heparin (LMWH). Lyman GH, et al. J Clin Oncol. 2007;25: Lyman GH, Khorana AA, Falanga A, et al. American Society of Clinical Oncology Guideline: Recommendations for Venous Thromboembolism Prophylaxis and Treatment in Patients With Cancer. J Clin Oncol. 2007;25: Charles L Bennett, MD, PhD, MPP Northwestern University Chicago
 issued guidelines for prophylaxis and treatment of VTE in cancer patients. Among the recommendations are that all cancer patients who are hospitalized or are undergoing cancer surgery should be considered for prophylaxis, and the preferred drug is low-molecular-weight heparin (LMWH). Lyman GH, et al. J Clin Oncol. 2007;25: Lyman GH, Khorana AA, Falanga A, et al. American Society of Clinical Oncology Guideline: Recommendations for Venous Thromboembolism Prophylaxis and Treatment in Patients With Cancer. J Clin Oncol. 2007;25: Charles L Bennett, MD, PhD, MPP Northwestern University Chicago.")
87
Updated ASCO Guidelines Hospitalized Patients with Cancer
Role of VTE Prophylaxis Evidence Patients with cancer should be considered candidates for VTE prophylaxis with anticoagulants (UFH, LMWH, or fondaparinux) in the absence of bleeding or other contraindications to anticoagulation Multiple RCTs of hospitalized medical patients with subgroups of patients with cancer. The 8th ACCP guidelines strongly recommend (1A) prophylaxis with either low-dose heparin or LMWH for bedridden patients with active cancer. VOLUME 25 NUMBER 34 DECEMBER
 in the absence of bleeding or other contraindications to anticoagulation. Multiple RCTs of hospitalized medical patients with subgroups of patients with cancer. The 8th ACCP guidelines strongly recommend (1A) prophylaxis with either low-dose heparin or LMWH for bedridden patients with active cancer. VOLUME 25 NUMBER 34 DECEMBER")
88
Prophylaxis in Cancer Patients
"Meeting the Challenges of VTV: Strategies for Implementing Guideline-based Recommendations" Prophylaxis in Cancer Patients Cancer patients undergoing surgical procedures: routine thromboprophylaxis that is appropriate for the type of surgery (Grade 1A) Cancer patients who are bedridden with an acute medical illness: routine thromboprophylaxis as for other high-risk medical patients (Grade 1A) Cancer patients receiving chemotherapy or hormonal therapy: recommend against the routine use of thromboprophylaxis for the primary prevention of VTE (Grade 1C) Cancer patients overall: recommend against the routine use of primary thromboprophylaxis to try to improve survival (Grade 1B) Current ACCP guidelines note that the use of appropriate thromboprophylaxis in hospitalized cancer patients with additional VTE risk factors provides an important opportunity to reduce the substantial burden of this complication. Prevention of VTE is important not only because VTE may be more difficult to diagnose in cancer patients, but also because the treatment of VTE in these patients may be less effective and associated with more bleeding complications. Cancer patients undergoing surgery should receive aggressive thromboprophylaxis appropriate for the type of surgery. Cancer patients with an acute medical illness who are bedridden should receive thromboprophylaxis as recommended for medical patients. Thromboprophylaxis is also indicated in selected palliative care patients in order to prevent further reduction in quality of life, but cancer patients who are fully ambulatory should not routinely be given thromboprophylaxis. 2008 ACCP Prevention of Venous Thromboembolism Practice Guidelines Geerts WH, et al. Chest. 2008;133(6 suppl):381S-453S. Geerts WH, Bergqvist D, Pineo GF, et al. Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th edition). Chest. 2008;133(6 suppl):381S-453S. Charles L Bennett, MD, PhD, MPP Northwestern University Chicago
 Cancer patients who are bedridden with an acute medical illness: routine thromboprophylaxis as for other high-risk medical patients (Grade 1A) Cancer patients receiving chemotherapy or hormonal therapy: recommend against the routine use of thromboprophylaxis for the primary prevention of VTE (Grade 1C) Cancer patients overall: recommend against the routine use of primary thromboprophylaxis to try to improve survival (Grade 1B) Current ACCP guidelines note that the use of appropriate thromboprophylaxis in hospitalized cancer patients with additional VTE risk factors provides an important opportunity to reduce the substantial burden of this complication. Prevention of VTE is important not only because VTE may be more difficult to diagnose in cancer patients, but also because the treatment of VTE in these patients may be less effective and associated with more bleeding complications. Cancer patients undergoing surgery should receive aggressive thromboprophylaxis appropriate for the type of surgery. Cancer patients with an acute medical illness who are bedridden should receive thromboprophylaxis as recommended for medical patients. Thromboprophylaxis is also indicated in selected palliative care patients in order to prevent further reduction in quality of life, but cancer patients who are fully ambulatory should not routinely be given thromboprophylaxis ACCP Prevention of Venous Thromboembolism Practice Guidelines. Geerts WH, et al. Chest. 2008;133(6 suppl):381S-453S. Geerts WH, Bergqvist D, Pineo GF, et al. Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th edition). Chest. 2008;133(6 suppl):381S-453S. Charles L Bennett, MD, PhD, MPP Northwestern University Chicago.")
89
Therapeutic Anticoagulation Treatment for VenousThromboembolism
The NCCN panel recommends VTE thromboprophylaxis for all hospitalized patients with cancer who do not have contraindications to such therapy Panel also emphasized that an increased level of clinical suspicion of VTE should be maintained for cancer patients. Following hospital discharge, it is recommended that patients at high-risk of VTE (e.g. cancer surgery patients) continue to receive VTE prophylaxis for up to 4 weeks post-operation.
 continue to receive VTE prophylaxis for up to 4 weeks post-operation.")
90
Caveats No randomized controlled trials (RCTs) designed ad hoc for hospitalized medical cancer patients are available Recommendations are based on RCTs of acutely ill medical patients, involving a small proportion of patients with cancer No bleeding data are reported specifically in the subgroup of patients with cancer

91
Screening for asymptomatic DVT with venography or ultrasound
Anticoagulant Prophylaxis to Prevent Screen-Detected VTE High Risk Hospitalized Medical Patients 3 large, randomized, placebo-controlled, double-blind trials in medical patients at high risk including cancer MEDENOX (enoxaparin)1 ~ 15% PREVENT (dalteparin)2 ~5% ARTEMIS (fondaparinux)3 ~15% Screening for asymptomatic DVT with venography or ultrasound Samama MM, et al. N Engl J Med. 1999;341: Leizorovicz A, et al. Circulation. 2004;110: Cohen AT, et al. BMJ. 2006;332:
1 ~ 15% PREVENT (dalteparin)2 ~5% ARTEMIS (fondaparinux)3 ~15% Screening for asymptomatic DVT with venography or ultrasound. Samama MM, et al. N Engl J Med. 1999;341: Leizorovicz A, et al. Circulation. 2004;110: Cohen AT, et al. BMJ. 2006;332:")
92
Anticoagulant Prophylaxis to Prevent Screen-Detected VTE
High Risk Hospitalized Medical Patients RRR 63% 45% 47% Study RRR Thromboprophylaxis Patients with VTE (%) MEDENOX1 Placebo 14.9 P < 0.001 Enoxaparin 40 mg 5.5 PREVENT2 Placebo 5.0 P = Dalteparin 5,000 units 2.8 Data NOT specific to cancer patients Placebo 10.5 ARTEMIS3 Fondaparinux 2.5 mg 5.6 1Samama MM, et al. N Engl J Med. 1999;341: Leizorovicz A, et al. Circulation. 2004;110:874-9. 3Cohen AT, et al. BMJ 2006; 332: 92
 MEDENOX1. Placebo P < Enoxaparin 40 mg PREVENT2. Placebo P = Dalteparin 5,000 units Data NOT specific to cancer patients. Placebo ARTEMIS3. Fondaparinux 2.5 mg Samama MM, et al. N Engl J Med. 1999;341: Leizorovicz A, et al. Circulation. 2004;110: Cohen AT, et al. BMJ 2006; 332:")
93
Anticoagulant Prophylaxis to Prevent Screen-Detected VTE
High Risk Hospitalized Medical Patients: Major Bleeding 1.7% 1.1% Incidence of Major Bleeding (%) 0.49% Data NOT specific to cancer patients 0.16% 0.2% Study Samama MM, et al. N Engl J Med. 1999;341: Leizorovicz A, et al. Circulation. 2004;110:874-9. Cohen AT, et al. BMJ 2006; 332: 93
 0.49% Data NOT specific to cancer patients. 0.16% 0.2% Study. Samama MM, et al. N Engl J Med. 1999;341: Leizorovicz A, et al. Circulation. 2004;110: Cohen AT, et al. BMJ 2006; 332:")
94
Outcome, extended prophylaxis, n=2052 (%)
EXCLAIM: Extended-duration Enoxaparin Prophylaxis in High-risk Medical Patients (Most benefit seen in Level 1 Disability Patients with bedrest or sedentary without BRP-some with CA) End points Outcome, extended prophylaxis, n=2052 (%) Outcome, placebo, n=2062(%) RR reduction (%) p Major bleeding 0.8% 0.3% VTE events 2.5 4.0 38% 0.001 Symptomatic 0.3 1.1 73% 0.004 No Sxs 3.7 34% 0.032 (Hull RD et al. Ann Intern Med 2010; 153:8)
 End points. Outcome, extended prophylaxis, n=2052 (%) Outcome, placebo, n=2062(%) RR reduction (%) p. Major bleeding. 0.8% 0.3% VTE events % Symptomatic % No Sxs % (Hull RD et al. Ann Intern Med 2010; 153:8)")
95
Increased ICH: 5.1% vs 1.2% for placebo Both NS significant
PRODIGE: Dalteparin for Primary VTE Prophylaxis in Newly Diagnosed Malignant Glioma Reduced VTE for dalteparin 5,000 anti-Xa units qd for 6 mos: 11% vs 17% for placebo Increased ICH: 5.1% vs 1.2% for placebo Both NS significant Perry JR et al. JTH 2010;8;1959

96
2009 NCCN Guidelines: DVT Prophylaxis
Pharmacologic Prophylaxis UFH LMWH Pentasaccharide [nccn.org.VTE guidelines.2006/ p4 (VTE-1)] No Adult Cancer Inpatient Contraindication to Anticoagulation Treatment Yes Mechanical Prophylaxis Sequential Compression Devices Compression Stockings For adult patients with a diagnosis of cancer or suspicion of cancer, the National Comprehensive Cancer Network 2006 guidelines recommend pharmacologic prophylaxis with unfractionated heparin (UFH), low-molecular-weight heparin (LMWH), or pentasaccaride1 For patients with a contraindication to pharmacologic anticoagulation treatment, mechanical prophylaxis (sequential compression devices or compression stockings) is recommended1 [1/nccn.org.VTE guidelines.2006/ p 4 (VTE-1); p12/Table (VTE-C)] [1/nccn/ p4 (VTE-1)] NCCN, National Comprehensive Cancer Network. NCCN. Venous Thromboembolic Disease: Version Available at: physician_gls/PDF/vte.pdf. 1. National Comprehensive Cancer Network. Venous Thromboembolic Disease: Version Available at: Accessed May 9, 2006.
] No. Adult Cancer. Inpatient. Contraindication to Anticoagulation Treatment. Yes. Mechanical Prophylaxis. Sequential Compression Devices. Compression Stockings. For adult patients with a diagnosis of cancer or suspicion of cancer, the National Comprehensive Cancer Network 2006 guidelines recommend pharmacologic prophylaxis with unfractionated heparin (UFH), low-molecular-weight heparin (LMWH), or pentasaccaride1. For patients with a contraindication to pharmacologic anticoagulation treatment, mechanical prophylaxis (sequential compression devices or compression stockings) is recommended1. [1/nccn.org.VTE guidelines.2006/ p 4 (VTE-1); p12/Table (VTE-C)] [1/nccn/ p4 (VTE-1)] NCCN, National Comprehensive Cancer Network. NCCN. Venous Thromboembolic Disease: Version Available at: physician_gls/PDF/vte.pdf. 1. National Comprehensive Cancer Network. Venous Thromboembolic Disease: Version Available at: Accessed May 9,")
97
Mechanical thromboprophylaxis in critically ill patients: a systematic review and meta-analysis
RESULTS: 21 relevant studies (5 randomized controlled trials, 13 observational studies, and 3 surveys) were found. A total of 811 patients were randomized in the 5 randomized controlled trials; 3421 patients participated in the observational studies. Trauma patients only were enrolled in 4 randomized controlled trials and 4 observational studies. Meta-analysis of 2 randomized controlled trials with similar populations and outcomes revealed that use of compression and pneumatic devices did not reduce the incidence of venous thromboembolism. The pooled risk ratio was 2.37 (CI,95% ). A range of methodological issues, including bias and confounding variables, make meaningful interpretation of the observational studies difficult. CONCLUSIONS: The role of mechanical approaches to thromboprophylaxis for intensive care patients remains uncertain. The beneficial role for mechanical thromboprophylaxis in cancer pts is empiric and derived from benefits seen in surgical studies; No controlled studies in cancer patients Limbus A et al. Am J Crit Care, 2006;15:402-10
 were found. A total of 811 patients were randomized in the 5 randomized controlled trials; 3421 patients participated in the observational studies. Trauma patients only were enrolled in 4 randomized controlled trials and 4 observational studies. Meta-analysis of 2 randomized controlled trials with similar populations and outcomes revealed that use of compression and pneumatic devices did not reduce the incidence of venous thromboembolism. The pooled risk ratio was 2.37 (CI,95% ). A range of methodological issues, including bias and confounding variables, make meaningful interpretation of the observational studies difficult. CONCLUSIONS: The role of mechanical approaches to thromboprophylaxis for intensive care patients remains uncertain. The beneficial role for mechanical thromboprophylaxis in cancer pts is empiric and derived from benefits seen in surgical studies; No controlled studies in cancer patients. Limbus A et al. Am J Crit Care, 2006;15:")
98
VTE Prophylaxis Is Underused in Patients With Cancer
[1/Kakkar. Oncologist.2003/ p381/c1/line A1-A24; p383/c1/line 44-46, c2/line 1-3] [2/Stratton. ArchInternMed. Feb.2000/ p336/c2/line 7-11] [3/Bratzler. ArchInternMed. Sept.1998/ p1909/c1/line A10-A15, c2/line A1-A3] [4/Rahim.ThrmbRes. 2003/p3/c2/line 1-5] [5/Goldhaber. AmJCardiol.Jan.2004/ p261/c2/line 6-8] Cancer: FRONTLINE Survey1— 3891 Clinician Respondents Major Surgery2 Cancer: Surgical Major Abdominothoracic Surgery (Elderly)3 Confirmed DVT (Inpatients)5 52 Rate of Appropriate Prophylaxis, % Medical Inpatients4 Cancer: Medical VTE prophylaxis is underused in patients with cancer The Fundamental Research in Oncology and Thrombosis (FRONTLINE) survey was a questionnaire distributed globally to clinicians involved in cancer care and accessible on a dedicated Web site1 Data from 3891 completed questionnaires were available for analysis1 The results indicated that 52% of respondents would routinely utilize thromboprophylaxis for surgical oncology patients, and that most respondents only considered thromboprophlyaxis in approximately 5% of their medical oncology patients1 These results can be compared with prophylaxis rates in other patient groups as determined by other recent studies A retrospective record review in 10 US teaching or community-based hospitals of patients undergoing major surgeries (major abdominal surgery, total hip replacement, hip fracture repair, or total knee replacement) showed VTE prophylaxis was used in 89% of patients2 A retrospective record review of patients aged 65 and older in 20 Oklahoma hospitals undergoing major abdominothoracic surgery indicated that prophylaxis was used in 38% of patients3 A retrospective record review at 2 Canadian hospitals of medical inpatients indicated that prophylaxis was used in 33% of patients4 In the DVT-FREE prospective registry of patients with ultrasound-confirmed DVT, among 5451 patients, 42% had received prophylaxis5 [1/Kakkar.Oncologist. 2003/p381/c1/ line A5-A22] [1/Kakkar/p381/c1/ line A23-A24] [1/Kakkar/p383/c1/ line 44-46, c2/line 1-3] [2/Stratton.ArchIntern Med.Feb.2000/ p334/c1/line A14-A19, c2/line A1-A2; p336/c2/line 7-11] [3/Bratzler.ArchIntern Med.Sept.1998/ p1909/c1/line A10-A15, c2/line A1-A3] [4/Rahim.ThrmbRes. 2003/p1/line A1-A12; p3/c2/line 1-5] [5/Goldhaber.AmJ Cardiol.Jan.2004/ p259/c1/line A1-A10; p261/c2/line 6-8] 5 1. Kakkar AK et al. Oncologist. 2003;8: 2. Stratton MA et al. Arch Intern Med. 2000;160: 3. Bratzler DW et al. Arch Intern Med. 1998;158: 4. Rahim SA et al. Thromb Res. 2003;111: 5. Goldhaber SZ et al. Am J Cardiol. 2004;93: 1. Kakkar AK, Levine M, Pinedo HM, Wolff R, Wong J. Venous thrombosis in cancer patients: insights from the FRONTLINE survey. Oncologist. 2003;8: 2. Stratton MA, Anderson FA, Bussey HI, et al. Prevention of venous thromboembolism: adherence to the 1995 American College of Chest Physicians consensus guidelines for surgical patients. Arch Intern Med. 2000;160: 3. Bratzler DW, Raskob GE, Murray CK, Bumpus LJ, Piatt DS. Underuse of venous thromboembolism prophylaxis for general surgery patients: physician practices in the community hospital setting. Arch Intern Med. 1998;158: 4. Rahim SA, Panju A, Pai M, Ginsberg J. Venous thromboembolism prophylaxis in medical inpatients: a retrospective chart review. Thromb Res. 2003;111: 5. Goldhaber SZ, Tapson VF, for the DVT FREE Steering Committee. A prospective registry of 5,451 patients with ultrasound-confirmed deep vein thrombosis. Am J Cardiol. 2004;93:
3. Confirmed DVT (Inpatients) Rate of Appropriate Prophylaxis, % Medical Inpatients4. Cancer: Medical. VTE prophylaxis is underused in patients with cancer. The Fundamental Research in Oncology and Thrombosis (FRONTLINE) survey was a questionnaire distributed globally to clinicians involved in cancer care and accessible on a dedicated Web site1. Data from 3891 completed questionnaires were available for analysis1. The results indicated that 52% of respondents would routinely utilize thromboprophylaxis for surgical oncology patients, and that most respondents only considered thromboprophlyaxis in approximately 5% of their medical oncology patients1. These results can be compared with prophylaxis rates in other patient groups as determined by other recent studies. A retrospective record review in 10 US teaching or community-based hospitals of patients undergoing major surgeries (major abdominal surgery, total hip replacement, hip fracture repair, or total knee replacement) showed VTE prophylaxis was used in 89% of patients2. A retrospective record review of patients aged 65 and older in 20 Oklahoma hospitals undergoing major abdominothoracic surgery indicated that prophylaxis was used in 38% of patients3. A retrospective record review at 2 Canadian hospitals of medical inpatients indicated that prophylaxis was used in 33% of patients4. In the DVT-FREE prospective registry of patients with ultrasound-confirmed DVT, among 5451 patients, 42% had received prophylaxis5. [1/Kakkar.Oncologist. 2003/p381/c1/ line A5-A22] [1/Kakkar/p381/c1/ line A23-A24] [1/Kakkar/p383/c1/ line 44-46, c2/line 1-3] [2/Stratton.ArchIntern Med.Feb.2000/ p334/c1/line A14-A19, c2/line A1-A2; p336/c2/line 7-11] [3/Bratzler.ArchIntern Med.Sept.1998/ p1909/c1/line A10-A15, c2/line A1-A3] [4/Rahim.ThrmbRes. 2003/p1/line A1-A12; p3/c2/line 1-5] [5/Goldhaber.AmJ Cardiol.Jan.2004/ p259/c1/line A1-A10; p261/c2/line 6-8] Kakkar AK et al. Oncologist. 2003;8: Stratton MA et al. Arch Intern Med. 2000;160: Bratzler DW et al. Arch Intern Med. 1998;158: Rahim SA et al. Thromb Res. 2003;111: Goldhaber SZ et al. Am J Cardiol. 2004;93: Kakkar AK, Levine M, Pinedo HM, Wolff R, Wong J. Venous thrombosis in cancer patients: insights from the FRONTLINE survey. Oncologist. 2003;8: Stratton MA, Anderson FA, Bussey HI, et al. Prevention of venous thromboembolism: adherence to the 1995 American College of Chest Physicians consensus guidelines for surgical patients. Arch Intern Med. 2000;160: Bratzler DW, Raskob GE, Murray CK, Bumpus LJ, Piatt DS. Underuse of venous thromboembolism prophylaxis for general surgery patients: physician practices in the community hospital setting. Arch Intern Med. 1998;158: Rahim SA, Panju A, Pai M, Ginsberg J. Venous thromboembolism prophylaxis in medical inpatients: a retrospective chart review. Thromb Res. 2003;111: Goldhaber SZ, Tapson VF, for the DVT FREE Steering Committee. A prospective registry of 5,451 patients with ultrasound-confirmed deep vein thrombosis. Am J Cardiol. 2004;93:")
99
Despite Evidence, Medical Patients at Risk Remain Unprotected
"Meeting the Challenges of VTV: Strategies for Implementing Guideline-based Recommendations" Despite Evidence, Medical Patients at Risk Remain Unprotected ENDORSE1 IMPROVE2 Medical Surgical No. of patients 37,356 30,827 At risk for VTE 42% 64% Receiving ACCP Tx 40% 59% United States Other Countries No. of patients 3,410 11,746 VTE prophylaxis 1852 (54%) 5788 (49%) LMWH 476 (14%) 4657 (40%) UFH 717 (21%) 1014 (9%) The ENDORSE (Epidemiologic International Day for the Evaluation of Patients at Risk for Venous Thromboembolism in the Acute Hospital Care Setting) study evaluated the proportion of medical and surgical patients at risk for VTE who received prophylaxis.1 Patients were enrolled from 358 randomly selected hospitals in 32 countries. Of the 68,183 patients enrolled, a mean of 52% were at risk for VTE, including 64% of surgical and 42% of medical patients. However, only 59% of surgical and 40% of medical patients were receiving prophylaxis. The IMPROVE (International Medical Prevention Registry on Venous Thromboembolism) study evaluated risk and prophylaxis use in the United States compared with other countries.2 From July 2002 to September 30, 2006, 15,156 patients were enrolled from 52 hospitals in 12 countries. Only 54% of at-risk US patients and 49% of at-risk patients outside the United States received VTE prophylaxis. Intermittent pneumatic compression was the most common form of medical prophylaxis used in the United States, although it was used very rarely in other countries (22% vs 0.2%, respectively). Unfractionated heparin was the most frequent pharmacological approach used in the United States (21% of patients), with low-molecular–weight heparin used most frequently in other participating countries (40%). Cohen AT, et al. Presented at: 2007 Congress of the International Society on Thrombosis and Haemostasis; July 6-12, 2007; Geneva, Switzerland. Tapson VF, et al. Chest. 2007;132(3): Cohen AT, Tapson VF, Bergmann JF, et al. A large-scale, global observational study of venous thromboembolism risk and prophylaxis in the acute hospital care setting: the ENDORSE study. Presented at: 2007 Congress of the International Society on Thrombosis and Haemostasis; July 6-12, 2007; Geneva, Switzerland. Abstract ISTH 2007 O-S-002. Tapson VF, Decoucus H, Pini M, et al. Venous thromboembolism prophylaxis in acutely ill hospitalized medical patients. Findings from the International Medical Prevention Registry on Venous Thromboembolism. Chest. 2007;132(3): Charles L Bennett, MD, PhD, MPP Northwestern University Chicago
 5788 (49%) LMWH. 476 (14%) 4657 (40%) UFH. 717 (21%) 1014 (9%) The ENDORSE (Epidemiologic International Day for the Evaluation of Patients at Risk for Venous Thromboembolism in the Acute Hospital Care Setting) study evaluated the proportion of medical and surgical patients at risk for VTE who received prophylaxis.1 Patients were enrolled from 358 randomly selected hospitals in 32 countries. Of the 68,183 patients enrolled, a mean of 52% were at risk for VTE, including 64% of surgical and 42% of medical patients. However, only 59% of surgical and 40% of medical patients were receiving prophylaxis. The IMPROVE (International Medical Prevention Registry on Venous Thromboembolism) study evaluated risk and prophylaxis use in the United States compared with other countries.2 From July 2002 to September 30, 2006, 15,156 patients were enrolled from 52 hospitals in 12 countries. Only 54% of at-risk US patients and 49% of at-risk patients outside the United States received VTE prophylaxis. Intermittent pneumatic compression was the most common form of medical prophylaxis used in the United States, although it was used very rarely in other countries (22% vs 0.2%, respectively). Unfractionated heparin was the most frequent pharmacological approach used in the United States (21% of patients), with low-molecular–weight heparin used most frequently in other participating countries (40%). Cohen AT, et al. Presented at: 2007 Congress of the International Society on Thrombosis and Haemostasis; July 6-12, 2007; Geneva, Switzerland. Tapson VF, et al. Chest. 2007;132(3): Cohen AT, Tapson VF, Bergmann JF, et al. A large-scale, global observational study of venous thromboembolism risk and prophylaxis in the acute hospital care setting: the ENDORSE study. Presented at: 2007 Congress of the International Society on Thrombosis and Haemostasis; July 6-12, 2007; Geneva, Switzerland. Abstract ISTH 2007 O-S-002. Tapson VF, Decoucus H, Pini M, et al. Venous thromboembolism prophylaxis in acutely ill hospitalized medical patients. Findings from the International Medical Prevention Registry on Venous Thromboembolism. Chest. 2007;132(3): Charles L Bennett, MD, PhD, MPP Northwestern University Chicago.")
100
Electronic Alerts to Prevent VTE in Hospitalized Patients
"Meeting the Challenges of VTV: Strategies for Implementing Guideline-based Recommendations" Electronic Alerts to Prevent VTE in Hospitalized Patients 100 98 96 Intervention group Freedom From DVT or PE (%) 94 92 Control group 90 P<.001 Kuchler and colleagues evaluated a computer linked to a patient database and designed to identify consecutive hospitalized patients at increased risk for VTE. The program used eight common risk factors to determine each patient’s risk profile for VTE, each factor weighted according to a point scale: cancer, prior VTE, and hypercoagulability were assigned a score of 3; major surgery was assigned a score of 2; advanced age, obesity, bed rest, and use of hormone therapy or oral contraceptives were assigned a score of 1. An increased risk of VTE was defined as a cumulative risk score of at least 4. The primary end point was clinically diagnosed DVT or PE at 90 days. A total of 1255 patients were randomly assigned to the intervention group, in which the responsible physician was alerted to a patient’s risk of DVT; 1251 patients were assigned to a control group, in which no alert was issued. Kaplan-Meier estimates of the absence of VTE at 90 days (shown in figure) were 94.1% and 90.6%, respectively for the intervention group vs control group (P<.001). More patients in the intervention group than in the control group received mechanical prophylaxis or pharmacologic prophylaxis. The primary end point occurred in 4.9% of the intervention group vs 8.2% of the control group. The computer alert reduced the risk of DVT or PE at 90 days by 41% (P=.001). 300 600 90 Days No. at Risk Intervention group 1255 977 900 853 Control group 1251 976 893 839 P<.001 by the log-rank test for the comparison of the outcome between groups at 90 days. Reprinted with permission from Kucher N, et al. N Engl J Med. 2005;352: Kucher N, Koo S, Quiroz R, et al. Electronic alerts to prevent venous thromboembolism among hospitalized patients. N Engl J Med. 2005;352: Charles L Bennett, MD, PhD, MPP Northwestern University Chicago
 Control group. 90. P<.001. Kuchler and colleagues evaluated a computer linked to a patient database and designed to identify consecutive hospitalized patients at increased risk for VTE. The program used eight common risk factors to determine each patient’s risk profile for VTE, each factor weighted according to a point scale: cancer, prior VTE, and hypercoagulability were assigned a score of 3; major surgery was assigned a score of 2; advanced age, obesity, bed rest, and use of hormone therapy or oral contraceptives were assigned a score of 1. An increased risk of VTE was defined as a cumulative risk score of at least 4. The primary end point was clinically diagnosed DVT or PE at 90 days. A total of 1255 patients were randomly assigned to the intervention group, in which the responsible physician was alerted to a patient’s risk of DVT; 1251 patients were assigned to a control group, in which no alert was issued. Kaplan-Meier estimates of the absence of VTE at 90 days (shown in figure) were 94.1% and 90.6%, respectively for the intervention group vs control group (P<.001). More patients in the intervention group than in the control group received mechanical prophylaxis or pharmacologic prophylaxis. The primary end point occurred in 4.9% of the intervention group vs 8.2% of the control group. The computer alert reduced the risk of DVT or PE at 90 days by 41% (P=.001) Days. No. at Risk. Intervention group Control group P<.001 by the log-rank test for the comparison of the outcome between groups at 90 days. Reprinted with permission from Kucher N, et al. N Engl J Med. 2005;352: Kucher N, Koo S, Quiroz R, et al. Electronic alerts to prevent venous thromboembolism among hospitalized patients. N Engl J Med. 2005;352: Charles L Bennett, MD, PhD, MPP Northwestern University Chicago.")
101
Role of VTE Prophylaxis
Ambulatory Patients with Cancer Without VTE Receiving Systemic Chemotherapy Updated ASCO Guidelines Role of VTE Prophylaxis Evidence Routine prophylaxis with an antithrombotic agents is not recommended except as noted below Routine prophylaxis in ambulatory patients receiving chemotherapy is not recommended due to conflicting trials, potential bleeding, the need for laboratory monitoring and dose adjustment, and the relatively low incidence of VTE. LMWH or adjusted dose warfarin (INR ~ 1.5) is recommended in myeloma patients on thalidomide or lenalidomide plus chemotherapy or dexamethasone This recommendation is based on nonrandomized trial data and extrapolation from studies of postoperative prophylaxis in orthopedic surgery and a trial of adjusted-dose warfarin in breast cancer
 is recommended in myeloma patients on thalidomide or lenalidomide plus chemotherapy or dexamethasone. This recommendation is based on nonrandomized trial data and extrapolation from studies of postoperative prophylaxis in orthopedic surgery and a trial of adjusted-dose warfarin in breast cancer.")
102
Prospective Study of Adult Cancer Patients Receiving Systemic Chemotherapy
Prospective observational study conducted at 117 randomly selected US practice sites. Data obtained on 4, consecutive adult patients initiating a new chemotherapy regimen between March and February 2006. There were no exclusions for age, prior history or comorbid ities with nearly 40% of patients age 65 and older. Kuderer NM et al; J Clin Oncol 2008 (ASCO 2008).
.")
103
Reported Cause of Early Mortality Cancer Patients Starting New Chemotherapy
Title Slide 103 Subtitle Cause of Death No VTE N=4,365 VTE N=93 All N=4,458 PD 2.1 2.2 Infection 0.3 PE 5.4 0.1 Pulmonary 0.2 Bleeding Other vascular Unknown All 3.2 7.6 3.3 [HR=5.48, 95%CI: ; P<.0001] No VTE Patients in the intermediate and high VT Risk Score Categories: have significantly greater cumulative risk of developing VTE during the first 4 months of chemotherapy VTE Kuderer NM et al; J Clin Oncol 2008 (ASCO 2008)
")
104
RCTs of Thromboprophylaxis in Ambulatory Cancer Patients: Warfarin
Double-blind, placebo-controlled RCT demonstrated the efficacy of low-intensity warfarin (INR ) in patients receiving chemotherapy for metastatic breast cancer 311 women with metastatic breast cancer on 1st- or 2nd-line chemotherapy Randomized to 1 mg warfarin for 6 weeks, then warfarin titrated to INR or placebo 1 VTE in warfarin group vs 7 in placebo arm 85% risk reduction, P = .03, with no increased bleeding INR=international normalized ratio Levine M, et al. Lancet. 1994;343:
 in patients receiving chemotherapy for metastatic breast cancer. 311 women with metastatic breast cancer on 1st- or 2nd-line chemotherapy. Randomized to 1 mg warfarin for 6 weeks, then warfarin titrated to INR or placebo. 1 VTE in warfarin group vs 7 in placebo arm. 85% risk reduction, P = .03, with no increased bleeding. INR=international normalized ratio. Levine M, et al. Lancet. 1994;343:")
105
Low Molecular Weight Heparin in RCTs of Thromboprophylaxis in Ambulatory Cancer Patients
Trial N Treatment Chemo Duration VTE Major Bleeding FAMOUS Solid tumors (Stage III/IV) 385 Dalteparin Placebo 64% 12 months 2.4% 3.3% 0.5% TOPIC-I Breast (Stage IV) 353 Certoparin 100% 6 months 4% 1.7% TOPIC-2 NSCLC 547 4.5%† 8.3% 3.7% 2.2% PRODIGE Glioma 186 - 6-12 months 11% 17% 5.1% 1.2% SIDERAS Solid Tumors 141 Placebo/Control 54% Indefinitely 5.9% 7.1% 2.9% PROTECHT 1166 Nadroparin 2:1 Placebo < 4 months with chemo 1.4% 0.7% 1. Kakkar AK, et al. J Clin Oncol. 2004;22: Haas SK, et al. J Thromb Haemost. 2005(suppl 1): abstract OR Perry JR et al. Proc ASCO Sideras K et al. Mayo Clin Proc 2006; 81: Agnelli G et al. Am Soc Hemat Sunday December 7, 2008
 385. Dalteparin. Placebo. 64% 12 months. 2.4% 3.3% 0.5% TOPIC-I. Breast. (Stage IV) 353. Certoparin. 100% 6 months. 4% 1.7% TOPIC-2. NSCLC %† 8.3% 3.7% 2.2% PRODIGE. Glioma months. 11% 17% 5.1% 1.2% SIDERAS. Solid Tumors Placebo/Control. 54% Indefinitely. 5.9% 7.1% 2.9% PROTECHT Nadroparin. 2:1 Placebo. < 4 months. with chemo. 1.4% 0.7% 1. Kakkar AK, et al. J Clin Oncol. 2004;22: Haas SK, et al. J Thromb Haemost. 2005(suppl 1): abstract OR Perry JR et al. Proc ASCO Sideras K et al. Mayo Clin Proc 2006; 81: Agnelli G et al. Am Soc Hemat Sunday December 7,")
106
The PROTECHT Study RCT of Thromboprophylaxis in Cancer Patients Receiving Chemotherapy DESIGN
Placebo-controlled, double blind, multicenter RCT Nadroparin 3,800 anti Xa IU daily vs placebo: 2:1 1150 patients receiving chemotherapy for locally advanced or metastatic cancer. Start with new CTX; continue for maximum of 4 mos Mean treatment duration: 90 days Primary outcome: clinically detected thrombotic events, i.e., composite of venous and arterial TE* Main safety outcome: Major bleeding * deep vein thrombosis of the lower and upper limbs, visceral and cerebral venous thrombosis, pulmonary embolism, acute myocardial infarction, ischemic stroke, acute peripheral arterial thromboembolism, unexplained death of possible thromboembolic origin Agnelli G et al: Lancet 2009;10, 930

107
Primary Efficacy Outcome: Any TE Event*
The PROTECHT Study RCT of Thromboprophylaxis in Cancer Patients Receiving Chemotherapy RESULTS Primary Efficacy Outcome: Any TE Event* Nadroparin: 16 of 769 (2.1%) Placebo: 15 of 381 (3.9%) Relative risk reduction: 47.2%, (interim-adjusted p=0.033) Absolute risk decrease: 1.8%; NNT = 53.8 Venous thromboembolism (VTE): Nadroparin: 11 of 769 (1.4%) Placebo: 11 of 381 (2.9%) NS Major Bleeding: Nadroparin: 5 (0.7%) Placebo: 0 (p= 0.177) Absolute risk increase: 0.7%; NNH = 153.8 33 patients in the nadroparin group and 16 in the placebo group had died; 48 of these deaths were due to disease progression. Agnelli G et al: Lancet 2009;10:930
 Placebo: 15 of 381 (3.9%) Relative risk reduction: 47.2%, (interim-adjusted p=0.033) Absolute risk decrease: 1.8%; NNT = Venous thromboembolism (VTE): Nadroparin: 11 of 769 (1.4%) Placebo: 11 of 381 (2.9%) NS. Major Bleeding: Nadroparin: 5 (0.7%) Placebo: 0 (p= 0.177) Absolute risk increase: 0.7%; NNH = patients in the nadroparin group and 16 in the placebo group had died; 48 of these deaths were due to disease progression. Agnelli G et al: Lancet 2009;10:930.")
108
2.1% DVT and 0.8% PE with placebo (N=381 pts)
LMWH “halves” VTE in ambulatory patients with metastatic or locally advanced cancer who are receiving chemotherapy PROTECHT All cause thrombo- embolic events: 2% LMWH vs 3.9% in placebo Major bleeding: 0.7% LMWH vs none in placebo (P=0.18) By the end of study treatment, 33 LMWH deaths vs 16 in placebo group; 48 of these deaths due to CA progression Benefits most apparent in those with lung or GI CA (not pancreatic) Agnelli G et al. Oct 2009 2.1% DVT and 0.8% PE with placebo (N=381 pts) p=0.02 NNT=53.8 1% DVT and 0.4% PE with LMWH (N=769 pts)
 By the end of study treatment, 33 LMWH deaths vs 16 in placebo group; 48 of these deaths due to CA progression. Benefits most apparent in those with lung or GI CA (not pancreatic) Agnelli G et al. Oct % DVT and 0.8% PE with placebo (N=381 pts) p=0.02. NNT= % DVT and 0.4% PE with LMWH (N=769 pts)")
109
VTE Incidence In Various Tumors
Oncology Setting VTE Incidence Breast cancer (Stage I & II) w/o further treatment 0.2% Breast cancer (Stage I & II) w/ chemo 2% Breast cancer (Stage IV) w/ chemo 8% Non-Hodgkin’s lymphomas w/ chemo 3% Hodgkin’s disease w/ chemo 6% Advanced cancer (1-year survival=12%) 9% High-grade glioma 26% Multiple myeloma (thalidomide + chemo) 28% Renal cell carcinoma 43% Solid tumors (anti-VEGF + chemo) 47% Wilms tumor (cavoatrial extension) 4% Otten, et al. Haemostasis 2000;30:72. Lee & Levine. Circulation 2003;107:I17
 w/o further treatment. 0.2% Breast cancer (Stage I & II) w/ chemo. 2% Breast cancer (Stage IV) w/ chemo. 8% Non-Hodgkin’s lymphomas w/ chemo. 3% Hodgkin’s disease w/ chemo. 6% Advanced cancer (1-year survival=12%) 9% High-grade glioma. 26% Multiple myeloma (thalidomide + chemo) 28% Renal cell carcinoma. 43% Solid tumors (anti-VEGF + chemo) 47% Wilms tumor (cavoatrial extension) 4% Otten, et al. Haemostasis 2000;30:72. Lee & Levine. Circulation 2003;107:I17.")
110
Arterial Thrombotic Complications of Myeloma
N=195 ATE=11 VAD (n 6, 5.9%) TAD (n 2, 4.5%) PAD (n 3, 6.4%) 5.6% 4 developed thrombosis while on VKAs; 2 on LMWH Libourel et al. Blood 2010;116:2
 TAD (n 2, 4.5%) PAD (n 3, 6.4%) 5.6% 4 developed thrombosis while on VKAs; 2 on LMWH. Libourel et al. Blood 2010;116:2.")
111
LMWH Warfarin ASA 9 3 9 14 18 15-24 31 (LDW) 3-14
(LDW) 3-14 Palumbo A et al. Leukemia 2008;22:414
 Palumbo A et al. Leukemia 2008;22:414.")
112
These VTE prophylaxis regimens have not been assessed in any prospective, randomized trial and are recommended based on anecdotal experience Palumbo A et al. Leukemia 2008;22:414

113
VTE Risk with Bevacizumab in Colorectal Cancer
Approaches Risk of Antiangiogenesis in Myeloma Naluri SR et al. JAMA. 2008;300:2277

114
Tamoxifen and Chemotherapy
705 postmenopeusal women with breast cancer CMF regimen Total thromboembolic events 39 of 54 events occurred during chemotherapy Rate of thrombosis (%) 16 p=0.0001 14 9.6% 12 10 8 6 1.4% 4 2 Tamoxifen Tamoxifen + CT (n=352) (n=353) Pritchard , J Clin Onc, 1996 (3x2).PFIZER.ARICEPT.COL 8 114
 16. p= % % Tamoxifen. Tamoxifen + CT. (n=352) (n=353) Pritchard , J Clin Onc, (3x2).PFIZER.ARICEPT.COL")
115
Role of VTE Prophylaxis
Treatment of Patients with Established VTE to Prevent Recurrence (continued) Role of VTE Prophylaxis Evidence Anticoagulation for an indefinite period should be considered for patients with active cancer (metastatic disease, continuing chemotherapy) In the absence of clinical trials, benefits and risks of continuing LMWH beyond 6 months is a clinical judgment in the individual patient. Caution is urged in elderly patients and those with intracranial malignancy. Inferior vena cava filters are reserved for those with contraindications to anticoagulation or PE despite adequate long-term LMWH. Consensus recommendations due to lack of date in cancer-specific populations
 Role of VTE Prophylaxis. Evidence. Anticoagulation for an indefinite period should be considered for patients with active cancer (metastatic disease, continuing chemotherapy) In the absence of clinical trials, benefits and risks of continuing LMWH beyond 6 months is a clinical judgment in the individual patient. Caution is urged in elderly patients and those with intracranial malignancy. Inferior vena cava filters are reserved for those with contraindications to anticoagulation or PE despite adequate long-term LMWH. Consensus recommendations due to lack of date in cancer-specific populations.")
116
Treatment of Patients with Established VTE to Prevent Recurrence
Role of VTE Prophylaxis Evidence LMWH is the preferred approach for the initial 5-10 days in cancer patient with established VTE. LMWH for 3-6 months is more effective than vitamin K antagonists given for a similar duration for preventing recurrent VTE. LMWH for at least 6 months is preferred for long-term anticoagulant therapy. Vitamin K antagonists with a targeted INR of 2-3 are acceptable when LMWH is not available. The CLOT study demonstrated a relative risk reduction of 49% with LMWH vs. a vitamin K antagonist. Dalteparin sodium approved by the FDA for extended treatment of symptomatic VTE to reduce the risk of recurrence of VTE in patients with cancer (FDA 2007)
")
117
The CLOT Trial Study Schema
Control Group Dalteparin 200 IU/kg OD Vitamin K antagonist (INR 2.0 to 3.0) x 6 mo Randomization Experimental Group Source: Protocol Dalteparin 200 IU/kg OD x 1 mo then ~150 IU/kg OD x 5 mo 5 to 7 days 1 month 6 months Lee AY, et al. N Engl J Med. 2003;349: Slide #6
 x 6 mo. Randomization. Experimental Group. Source: Protocol. Dalteparin 200 IU/kg OD x 1 mo then ~150 IU/kg OD x 5 mo. 5 to 7 days. 1 month. 6 months. Lee AY, et al. N Engl J Med. 2003;349: Slide #6.")
118
Results: Symptomatic Recurrent VTE
CLOT Trial: Results: Symptomatic Recurrent VTE 5 10 15 20 25 Days Post Randomization 30 60 90 120 150 180 210 Probability of Recurrent VTE, % dalteparin, 9% VKA, 17% risk reduction = 52% HR 0.48 (95% CI 0.30, 0.77) log-rank p = 0.002 Lee AY, et al. N Engl J Med. 2003;349:
 log-rank p = Lee AY, et al. N Engl J Med. 2003;349:")
119
CLOT Trial: Results: Bleeding Results Dalteparin N=338 VKA N=335
p-value Major bleed 19 (5.6%) 12 (3.6%) 0.27 Associated with death 1 Critical site* 4 3 Transfusion of > 2 units of RBC or drop in Hb > 20 g/L 14 9 Any bleed 46 (13.6%) 62 (18.5%) 0.09 *intracranial, intraspinal, pericardial, retroperitoneal, intra-ocular, intra- articular Lee AY, et al. N Engl J Med. 2003;349:
 12 (3.6%) Associated with death. 1. Critical site* Transfusion of > 2 units of RBC. or drop in Hb > 20 g/L Any bleed. 46 (13.6%) 62 (18.5%) *intracranial, intraspinal, pericardial, retroperitoneal, intra-ocular, intra- articular. Lee AY, et al. N Engl J Med. 2003;349:")
120
Overall, these meta-analyses and clinical trials do not conclusively establish the need for prophylaxis of CVC-related thrombosis in cancer patients Chaukiyal P et al. Thromb Haemost 2008;99:38

121
Influence of Thrombophilia on Thrombotic Complications of CVADs in Cancer
In 10 studies involving more than 1250 cancer patients with CVADs vs CA controls: CA + FVL OR=5.18 (95% confidence interval: ) CA + G20210A OR=3.95 (95% confidence interval: ) The attributable risk of catheter associated thrombosis conferred by: FVL % G20210A % CAVD = central venous access devices Dentali F, et al. JTH. 2007;5(Suppl 2):P-S-564.
 CA + G20210A OR=3.95 (95% confidence interval: ) The attributable risk of catheter associated thrombosis conferred by: FVL 13.5% G20210A 3.6% CAVD = central venous access devices. Dentali F, et al. JTH. 2007;5(Suppl 2):P-S-564.")
122
ASCO Recommendations for VTE Prophylaxis in Patients with Cancer
Summary Patient Group Recommended Not Recommended Hospitalized patients with cancer VTE prophylaxis with anticoagulants If bleeding or contraindication to anticoagulation Ambulatory patients with cancer receiving chemotherapy Myeloma patients receiving thalidomide or lenalidomide + chemotherapy/ dexamethasone. LMWH or adjusted dose warfarin. Otherwise, no routine prophylaxis Patients with cancer undergoing surgery Prophylaxis with low-dose UFH or LMWH Prophylaxis with mechanical methods for patients with contraindications to pharmacologic methods Consider mechanical methods when contraindications to anticoagulation. Patients with cancer with established VTE Pharmacologic treatment for at least 6 months. Consider continued anticoagulation beyond 6 months in those with active cancer. - To improve survival Not recommended Lyman GH et al: J Clin Oncol 2007; 25: 122

123
What the ASCO/NCCN Guidelines Do Not Tell Us
What is the role for emerging novel anticoagulant medications? No comparisons with LMWH Is there equivalent safety and efficacy between m-enoxaparin and Lovenox? Is there a survival advantage to the use of LMWH in cancer patients? Is there a role for adjunctive statins with anticoagulation in cancer patients? Is there a role for monitoring hypercoagulability markers in cancer patients? How does palliative care influence the survival and VTE incidence data in cancer patients? How should incidental VTE be anticoagulated? What is the role for retrievable IVC filters in CA patients

124
New Frontiers and Evolving Paradigms in Cancer and Thrombosis
Risk Stratification Tools to Identify Patients for Primary and Secondary Prevention of VTE in the Setting of Malignancy Screening and VTE Risk Assessment Across the Complex Spectrum of Malignant Disorders—What Works? What Doesn’t? Alok A. Khorana, MD, FACP Vice-Chief, Division of Hematology/Oncology Associate Professor of Medicine and Oncology James P. Wilmot Cancer Center University of Rochester Rochester, New York

125
Disclosures Consultant sanofi‐aventis, Eisai, Leo Pharma Speaker’s Bureau sanofi‐aventis, Leo Pharma Grant/Research Support sanofi‐aventis

126
VTE in Cancer Patients Risk assessment for VTE in cancer patients
Clinical risk factors Biomarkers Risk assessment tools Implications for thromboprophylaxis studies Secondary prophylaxis

127
Risk Factors for VTE Patient-related factors Treatment-related factors
Older age Race, gender Comorbidities Treatment-related factors Hospitalization Chemotherapy Anti-angiogenics Major surgery Erythropoiesis-stimulating agents Transfusions Cancer-related factors Site of cancer Advanced stage Initial period after diagnosis Rao et al., in Cancer-Associated Thrombosis. (Khorana and Francis, Eds) 2007
")
128
VTE and Site of Cancer Adjusted OR Type of cancer (95% CI) Hematologic
28 ( ) Lung 22.2 ( ) GI 20.3 (4.9-83) Breast 4.9 ( ) Prostate 2.2 ( ) Blom JW et al. JAMA 2005
 Lung ( ) GI (4.9-83) Breast. 4.9 ( ) Prostate. 2.2 ( ) Blom JW et al. JAMA")
129
VTE With Bevacizumab However, when corrected for exposure time,
RR=1.29 (95% CI, ) 13% 9.9% Rate of VTE (%) RR=1.38 (95% CI, ) 6.2% 4.2% Bevacizumab (n=1,196) Control (n=1,083) Bevacizumab (n=3,795) Control (n=3,167) However, when corrected for exposure time, RR =1.1 (95% CI, ) All-Grade VTE (6 studies) High-Grade VTE (13 studies) Nalluri SR, et al. JAMA. 2008;300: Chu D. and Wu S. JAMA 2009; In reply
 13% 9.9% Rate of VTE (%) RR=1.38 (95% CI, ) 6.2% 4.2% Bevacizumab (n=1,196) Control (n=1,083) Bevacizumab (n=3,795) Control (n=3,167) However, when. corrected for. exposure time, RR =1.1. (95% CI, ) All-Grade VTE (6 studies) High-Grade VTE (13 studies) Nalluri SR, et al. JAMA. 2008;300: Chu D. and Wu S. JAMA 2009; In reply.")
130
Biomarkers for Cancer-Associated VTE
Blood counts Platelet count Leukocyte count Hemoglobin D-dimer Soluble P-selectin Tissue factor C-reactive protein Factor VIII

131
Incidence of VTE By Quartiles Of Pre-Chemotherapy Platelet Count
0% 1% 2% 3% 4% 5% 6% <250 >350 Pre-chemotherapy Platelet Counts (x1000) Incidence Of VTE Over 2.5 Months(%) P =0.005 This figure depicts the incidence of venous thromboembolism by quartiles of pre-chemotherapy platelet count. As can be seen, elevated platelet counts were associated with an increased risk of venous thromboembolism. Patients in the highest quartile of pre-chemotherapy platelet count with a count of > 337,000/ cu mm, had a 3.6% risk of VTE, and this was significantly greater than the 1.1 % risk observed with patients in the lowest quartile, with a pre-chemotherapy platelet count of < 217,000/ cu mm. The p value for trend was highly significant at 0.005, and the difference between the highest and lowest quartile was also significant at Khorana AA et al. Cancer 2005
 Incidence Of VTE Over 2.5 Months(%) P = This figure depicts the incidence of venous thromboembolism by quartiles of pre-chemotherapy platelet count. As can be seen, elevated platelet counts were associated with an increased risk of venous thromboembolism. Patients in the highest quartile of pre-chemotherapy platelet count with a count of > 337,000/ cu mm, had a 3.6% risk of VTE, and this was significantly greater than the 1.1 % risk observed with patients in the lowest quartile, with a pre-chemotherapy platelet count of < 217,000/ cu mm. The p value for trend was highly significant at 0.005, and the difference between the highest and lowest quartile was also significant at Khorana AA et al. Cancer")
132
Incidence of VTE by Pre-Chemotherapy Leukocyte Count
0% 1% 2% 3% 4% 5% 6% <4.5 (n=342) (n=3202) >11 (n=513) Pre-chemotherapy WBC Counts (x1000/mm 3 ) Incidence Of VTE Over 2.4 Months (%) P =0.0008 Khorana AA et al. Blood 2008
 (n=3202) >11 (n=513) Pre-chemotherapy WBC Counts (x1000/mm. 3. ) Incidence Of VTE Over 2.4 Months (%) P = Khorana AA et al. Blood")
133
Incidence of VTE by Type of Leukocyte
Absolute Neutrophil Count Absolute Monocyte P=0.0001 P<0.0001 Proportion with VTE This bar graph demonstrates that elevation of both absolute neutrophil count and absolute monocyte count prior to initiation of chemotherapy was associated with higher rates of VTE. Absolute lymphocytosis was not associated with increased risk of VTE. Connolly et al ISTH 2009 Abs 1573

134
Effect of Leukocyte and Platelet Counts on VTE Risk
In the Vienna CATS registry, platelet count >443,000 was associated with VTE (HR3.5) Simanek et al, J Thromb Hemost 2009 In the REAL-2 study of advanced GEJ/gastric cancers, leukocytosis was associated with VTE during chemotherapy (HR 2.0) Starling et al, J Clin Oncol 2009
 Simanek et al, J Thromb Hemost In the REAL-2 study of advanced GEJ/gastric cancers, leukocytosis was associated with VTE during chemotherapy (HR 2.0) Starling et al, J Clin Oncol")
135
Mortality by Pre-chemotherapy Leukocyte Count
0.20 0.18 0.16 0.14 0.12 0.10 0.08 0.06 0.04 0.02 0.00 WBC>11x109/L 14.0% (8.9%-21.6%) Proportion Died WBC<11x109/L 4.4% (3.2%-6.1%) Pre-chemotherapy leukocytosis in this cohort was also associated with increased mortality as demonstarted by this survival curve. The mortality rate at 150 days after initiating chemotherapy as estimated by kaplan meier method is 14% in the group with baseline leukocytosis (depicted in red) and 4.4% in the group with normal baseline wbc (depicted in black). This difference was highly significant with p value of < A multivariate survival analysis presented by Dr. Kuderer at ASH in 2008 revealed that leukocytosis was independently predictive of increased mortality with HR 2 and p value of P <0.0001 Time (Days) MVA for early mortality: HR 2.0, p = 0.001 Kuderer et al ASH 2008 Connolly et al ISTH 2009, Throm Res 2010
 Proportion Died. WBC<11x109/L. 4.4% (3.2%-6.1%) Pre-chemotherapy leukocytosis in this cohort was also associated with increased mortality as demonstarted by this survival curve. The mortality rate at 150 days after initiating chemotherapy as estimated by kaplan meier method is 14% in the group with baseline leukocytosis (depicted in red) and 4.4% in the group with normal baseline wbc (depicted in black). This difference was highly significant with p value of < A multivariate survival analysis presented by Dr. Kuderer at ASH in 2008 revealed that leukocytosis was independently predictive of increased mortality with HR 2 and p value of P < Time (Days) MVA for early mortality: HR 2.0, p = Kuderer et al ASH Connolly et al ISTH 2009, Throm Res")
136
Tissue Factor in Cancer: Lack of Standardized Assays
Immunohistochemistry of tumor specimens TF ELISA TF MP procoagulant activity assay Impedance-based flow cytometry

137
Tissue Factor Expression and VTE
Rate of VTE (%) Khorana AA, et al. Clin Cancer Res. 2007;13:
 Khorana AA, et al. Clin Cancer Res. 2007;13:")
138
Cumulative Incidence of VTE for Cancer Patients According to TF–bearing Microparticles
0.6 0.5 0.4 0.3 0.2 0.1 0.0 Log Rank P=0.002 Cumulative Incidence of VTE Cumulative incidence of VTE for cancer patients initially without VTE according to the presence of tissue factor–bearing microparticles. Tissue factor–bearing microparticle–positive (dashed line; n = 16) and tissue factor–bearing microparticle–negative (solid line; n = 44) cancer patients were assessed for radiographic evidence of thromboembolic disease. In the year following enrollment, thromboembolic disease only developed in a subset of patients who had detectable tissue factor–bearing microparticles. Median follow up was 8.9 mo (range, mo), and 75% of the patients were followed for ≥5 mo. There were 11 deaths on record, at a median of 4 mo after study entry (range, 4 d to 23 mo). Dashed line, cancer patients with high levels of tissue factor bearing microparticles (TFMP+); solid line, those with undetectable levels (TFMP-). Months Zwicker J I et al. Clin Cancer Res 2009;15:
 and tissue factor–bearing microparticle–negative (solid line; n = 44) cancer patients were assessed for radiographic evidence of thromboembolic disease. In the year following enrollment, thromboembolic disease only developed in a subset of patients who had detectable tissue factor–bearing microparticles. Median follow up was 8.9 mo (range, mo), and 75% of the patients were followed for ≥5 mo. There were 11 deaths on record, at a median of 4 mo after study entry (range, 4 d to 23 mo). Dashed line, cancer patients with high levels of tissue factor bearing microparticles (TFMP+); solid line, those with undetectable levels (TFMP-) Months. Zwicker J I et al. Clin Cancer Res 2009;15:")
139
FRAGEM and TF Biomarker Data
Boxplot of the percentage change of tissue factor antigen in the sera of pancreatic cancer patients in both the control and dalteparin groups Control Dalteparin 250 200 150 100 50 -50 Maraveyas, et al. Blood Coagul Fibrinolysis 2010

140
TF and Survival In Pancreatic Cancer
Median Survival in pts with TF MP-PCA >2.5 and </=2.5pg/ml. 10 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 Median survival was 98.5 days for TF >2.5 pg/mL vs. 231 days for TF </= 2.5 pg/mL p=< N=117 patients with pancreaticobiliary cancers Proportion surviving Days on study TF (pg/mL) < >=2.5 Bharthuar et al ASCO GI 2010
 <2.5 >=2.5. Bharthuar et al ASCO GI")
141
D-dimer, F1/2 and VTE in Cancer
Elevated D-d + F1/2 Elevated F1/2 Elevated D-dimer Nonelevated D-dimer and F1/2 Observation Time (Days) Cumulative Risk (probability) 0.25 0.20 0.15 0.10 0.05 Ay, C. et al. J Clin Oncol; 27:
 Cumulative Risk (probability) Ay, C. et al. J Clin Oncol; 27:")
142
VTE in Cancer Patients Risk assessment for VTE in cancer patients
Clinical risk factors Biomarkers Risk assessment tools Implications for thromboprophylaxis studies Secondary prophylaxis

143
VTE in Cancer Outpatients
The overwhelming majority of cancer patients are treated in the outpatient/ambulatory setting Which patients are most at risk? Which patients will benefit most from prophylaxis? How do you define “high” risk? Level of risk for which prophylaxis is considered acceptable by both patients and oncologists

144
Patient Characteristic
Risk Model Patient Characteristic Score Site of Cancer Very high risk (stomach, pancreas) High risk (lung, lymphoma, gynecologic, GU excluding prostate) 2 1 Platelet count > 350,000/mm3 Hb < 10g/dL or use of ESA Leukocyte count > 11,000/mm3 BMI > 35 kg/m2 Based on the multivariate analysis, we developed a predictive risk model for identifying patients at high risk for development of VTE at time of initiation of chemotherapy. Risk scores were developed based on the beta-coefficient for each variable in the multivariate model shown on the prior slide, rounded to the nearest integer to make the model clinically usable. A patient with a very high risk site of cancer (such as stomach or pancreas) would be assigned a score of 2; patients with high risk sites of cancer (such as lung, lymphoma, gynecologic or GU cancers) as well as elevated pre-chemotherapy platelet count, anemia with a Hgb < 10 g/dL or use of erythropoiesis-stimulating agent, elevated leukocyte count or a BMI >=35 would all be assigned scores of 1. Khorana AA et al. Blood 2008
 High risk (lung, lymphoma, gynecologic, GU excluding prostate) Platelet count > 350,000/mm3. Hb < 10g/dL or use of ESA. Leukocyte count > 11,000/mm3. BMI > 35 kg/m2. Based on the multivariate analysis, we developed a predictive risk model for identifying patients at high risk for development of VTE at time of initiation of chemotherapy. Risk scores were developed based on the beta-coefficient for each variable in the multivariate model shown on the prior slide, rounded to the nearest integer to make the model clinically usable. A patient with a very high risk site of cancer (such as stomach or pancreas) would be assigned a score of 2; patients with high risk sites of cancer (such as lung, lymphoma, gynecologic or GU cancers) as well as elevated pre-chemotherapy platelet count, anemia with a Hgb < 10 g/dL or use of erythropoiesis-stimulating agent, elevated leukocyte count or a BMI >=35 would all be assigned scores of 1. Khorana AA et al. Blood")
145
Risk Model Validation Rate of VTE over 2.5 mos (%) 8% n=734 n=1627
0.8% 1.8% 7.1% Development cohort 7% 0.3% 2.0% 6.7% Validation cohort n=374 n=842 n=149 6% 5% 4% Rate of VTE over 2.5 mos (%) 3% 2% 1% 0% Risk Low (0) Intermediate(1-2) High(>3) Khorana AA et al. Blood 2008
 3% 2% 1% 0% Risk Low (0) Intermediate(1-2) High(>3) Khorana AA et al. Blood")
146
Vienna CATS Validation
Full data available in 839 patients Median observation time/follow-up: 643 days Score 0 Score 1 Score 2 Score ≥3 6 months 1.5% 3.8% 9.4% 17.7% Number of Patients Events n n (%) Score ≥3 96 16 (17%) Score 2 231 25 (11%) Score 1 233 14 (6%) Score 0 279 7 (3%) Ay et al ISTH 2009 Abs
 Score ≥ (17%) Score (11%) Score (6%) Score (3%) Ay et al ISTH 2009 Abs.")
147
Expanded Risk Score with D-Dimer and sP-selectin
30.3% 1.0% 6 months Number of Patients Events n n (%) Score ≥5 31 9 (29%) Score 4 52 10 (19%) Score 3 137 15 (11%) Score 2 226 11 (5%) Score 1 192 13 (7%) Score 0 201 4 (2%) Ay et al ISTH 2009 Abs
 Score ≥ (29%) Score (19%) Score (11%) Score (5%) Score (7%) Score (2%) Ay et al ISTH 2009 Abs.")
148
Risk Score and Short-Term Mortality by VTE Risk Score Categories
Low Intermediate High P < Kuderer NM et al. ASH 2008

149
International Myeloma Working Group Thromboprophylaxis Recommendations
Individual risk factors: obesity (BMI ≥ 30), prior VTE, central venous catheter Comorbid risk factors: cardiac disease, chronic renal disease, diabetes, acute infection, immobilization Surgery risk factors: trauma, general surgery or any anesthesia Medications: erythropoietin Myeloma-related risk factors: diagnosis, hyperviscosity Myeloma therapy risk factors: multiagent chemotherapy, doxorubicin, high-dose steroids Patients with ≤ 1 VTE risk factor: Aspirin ( mg daily) Patients with ≥ 2 VTE risk factors: LMWH (enoxaparin 40 mg/d) or full-dose warfarin, although less existing supporting data for the latter Patients receiving thalidomide/lenalidomide concurrently with high-dose dexamethasone or doxorubicin should receive LMWH thromboprophylaxis Anticoagulant treatment can continue for 4 to 6 months or longer if additional risk factors are present Palumbo A, Rajkumar SV, Dimopoulos MA, et al. Prevention of thalidomide- and lenalidomide associated thrombosis in myeloma. Leukemia Feb;22(2):
, prior VTE, central venous catheter. Comorbid risk factors: cardiac disease, chronic renal disease, diabetes, acute infection, immobilization. Surgery risk factors: trauma, general surgery or any anesthesia. Medications: erythropoietin. Myeloma-related risk factors: diagnosis, hyperviscosity. Myeloma therapy risk factors: multiagent chemotherapy, doxorubicin, high-dose steroids. Patients with ≤ 1 VTE risk factor: Aspirin ( mg daily) Patients with ≥ 2 VTE risk factors: LMWH (enoxaparin 40 mg/d) or full-dose warfarin, although less existing supporting data for the latter. Patients receiving thalidomide/lenalidomide concurrently with high-dose dexamethasone or doxorubicin should receive LMWH thromboprophylaxis. Anticoagulant treatment can continue for 4 to 6 months or longer if additional risk factors are present. Palumbo A, Rajkumar SV, Dimopoulos MA, et al. Prevention of thalidomide- and lenalidomide associated thrombosis in myeloma. Leukemia Feb;22(2):")
150
VTE in Cancer Patients Risk assessment for VTE in cancer patients
Clinical risk factors Biomarkers Risk assessment tools Implications for thromboprophylaxis studies Secondary prophylaxis

151
Rates of VTE in Recent Prophylaxis Studies
Agnelli et al Lancet Onc 2009 Palumbo et al ASH 2009 Riess et al ISTH 2009 Maraveyas et al ESMO 2009

152
VTE in Lung Cancer: PROTECHT and TOPIC studies
sVTE LMWH sVTE Placebo All VTE LMWH All VTE Placebo PROTECHT 3.5% 5% 4% 6.2% TOPIC-2 3% 5.7% 4.5% 8.3% All 3.2% 5.5% 4.3% 7.8% Major Bleeding LMWH Major Bleeding Placebo PROTECHT 1% 0% TOPIC-2 3.7% 2.2% All 2.5% 1.7% NNT=50 (sVTE) NNT=28 (allVTE) RRR=46% NNH=125 Verso et al. JTH 2010 online
 NNT=28 (allVTE) RRR=46% NNH=125. Verso et al. JTH 2010 online.")
153
Ongoing Clinical Trials
Study (Agent) Criteria for inclusion* N Endpoints PHACS (dalteparin x 12 wks) -Risk score >=3 404 Asymptomatic and symptomatic VTE SAVE-ONCO (semuloparin up to 4 mos) -Lung, bladder, GI, ovary -Metastatic or locally advanced 3200 DVT, PE, VTE-related death MicroTEC (enoxaparin x 6 mos) -Lung, colon, pancreas -Metastatic or unresectable -Elevated TF MPs 227 VTE * All studies enroll patients initiating a new chemotherapy regimen
 Criteria for inclusion* N. Endpoints. PHACS. (dalteparin x 12 wks) -Risk score >= Asymptomatic and symptomatic VTE. SAVE-ONCO (semuloparin up. to 4 mos) -Lung, bladder, GI, ovary. -Metastatic or locally advanced DVT, PE, VTE-related death. MicroTEC (enoxaparin x 6 mos) -Lung, colon, pancreas. -Metastatic or unresectable. -Elevated TF MPs VTE. * All studies enroll patients initiating a new chemotherapy regimen.")
154
VTE in Cancer Patients Risk assessment for VTE in cancer patients
Clinical risk factors Biomarkers Risk assessment tools Implications for thromboprophylaxis studies Secondary prophylaxis

155
Predictors of Recurrent VTE: Findings from the RIETE Registry
Recurrent PE Age < 65 (OR 3.0) PE at entry (OR 1.9) < 3 months from diagnosis of cancer (OR 2.0) Recurrent DVT Age < 65 (OR 1.6) < 3 months from diagnosis of cancer (OR 2.4) Patients with leukocytosis had increased risk of recurrent VTE and death (OR 2.7) Trujillo-Santos et al Thromb Haem 2008
 PE at entry (OR 1.9) < 3 months from diagnosis of cancer (OR 2.0) Recurrent DVT. Age < 65 (OR 1.6) < 3 months from diagnosis of cancer (OR 2.4) Patients with leukocytosis had increased risk of recurrent VTE and death (OR 2.7) Trujillo-Santos et al Thromb Haem")
156
Reduction in Recurrent VTE
CLOT Study: Reduction in Recurrent VTE 5 10 15 20 25 Days Post Randomization 30 60 90 120 150 180 210 Probability of Recurrent VTE, % Risk reduction = 52% p-value = Dalteparin OAC Recurrent VTE Lee et.al. N Engl J Med, 2003;349:146

157
Treatment of Cancer-Associated VTE
Study Design Length of Therapy (Months) N Recurrent VTE (%) Major Bleeding (%) Death CLOT Trial (Lee 2003) Dalteparin OAC 6 336 9 17 4 39 41 CANTHENOX (Meyer 2002) Enoxaparin 3 67 71 11 21 7 16 23 LITE (Hull ISTH 2003) Tinzaparin 80 87 8 22 ONCENOX (Deitcher ISTH 2003) Enox (Low) Enox (High) 32 36 34 3.4 3.1 6.7 NS 0.002 NS 0.09 0.09 0.03 NS NS 0.03 NR NS NS
 N. Recurrent VTE (%) Major Bleeding. (%) Death. CLOT Trial. (Lee 2003) Dalteparin. OAC CANTHENOX. (Meyer 2002) Enoxaparin LITE. (Hull ISTH 2003) Tinzaparin ONCENOX. (Deitcher ISTH 2003) Enox (Low) Enox (High) NS NS NS. NS NR. NS. NS.")
158
Conclusions Cancer patients are clearly at increased risk for VTE but risk varies widely Yet, 53% of cancer patients are unaware that they are at high risk for VTE Sousou et al, Ca Inv 2010 High-risk subgroups can be identified based on clinical risk factors and biomarkers A recently validated risk model can predict risk of VTE (and mortality) using 5 simple clinical and laboratory variables
 using 5 simple clinical and laboratory variables.")
159
Conclusions LMWH-based prophylaxis is safe and effective in certain high-risk settings Hospitalized and surgical patients Highly selected cancer outpatients (myeloma, ?pancreas, ?? lung) Ongoing studies are adopting novel approaches to selecting patients for prophylaxis Clinicians need to conduct baseline and ongoing risk assessment for VTE in cancer patients receiving chemotherapy
 Ongoing studies are adopting novel approaches to selecting patients for prophylaxis. Clinicians need to conduct baseline and ongoing risk assessment for VTE in cancer patients receiving chemotherapy.")
160
VISION STATEMENT VTE in the Setting of Malignancy
New Frontiers and Evolving Paradigms in Cancer and Thrombosis VISION STATEMENT VTE in the Setting of Malignancy Samuel Z. Goldhaber, MD Cardiovascular Division Brigham and Women’s Hospital Professor of Medicine Harvard Medical School

161
Disclosures Research Support: BMS; Boehringer-Ingelheim; Eisai; Johnson & Johnson, Sanofi-Aventis Consultant: Boehringer-Ingelheim; BMS; Eisai; EKOS: Medscape; Merck; Pfizer; Sanofi-Aventis

162
New Frontiers and Evolving Paradigms in Cancer and Thrombosis
Toward Eradication of In-Hospital VTE: The Promise of Prophylaxis “VITAE” Studies

163
VTE Prophylaxis in 19,958 Medical Patients/9 Studies (Meta-analysis)
62% reduction in fatal PE 57% reduction in fatal or nonfatal PE 53% reduction in DVT Dentali F, et al. Ann Intern Med 2007; 146:

164
2 of every 100 hospitalized Medical Service patients suffer VTE.
VITAE I VITAE I uses a Federal database to model Hospitalized Medical Patients with VTE. 2 of every 100 hospitalized Medical Service patients suffer VTE. With universal in-hospital prophylaxis, the VTE rate would be cut by 58%. Thromb Haemost 2009; 102:

165
58% Reduction in VTE with Universal Prophylaxis in Hospitalized Medical Patients
Thromb Haemostas 2009; 102:

166
VITAE II VITAE II models the 5-year aftermath of initial VTE among these same Hospitalized Medical Patients who were initially stricken. If universal prophylaxis had been utilized initially, the 5-year VTE complication rates of death, recurrence, PTS, and CTEPH would have been reduced by 60%. Thromb Haemost 2009; 102:

167
VITAE II Status Quo 100% VTE Prophylaxis
Thromb Haemost 2009; 102:

168
Conclusions Electronic alerts can identify hospitalized cancer patients at risk for VTE. Optimal prophylaxis for hospitalized cancer patients is LMWH. When VTE is diagnosed in cancer patients, the only FDA-approved LMWH for Rx as monotherapy without warfarin is dalteparin.

169
Conclusions (Continued)
ACCP guidelines state that “every hospital should develop a formal strategy to prevent VTE.” As cancer therapies improve, quality life- years will be extended. DVT and PE will be mostly prevented in cancer patients, and when necessary to treat, will be managed will LMWH monotherapy.

Similar presentations