Download presentation
Presentation is loading. Please wait.

1
S.C. Fisiopatologia Respiratoria Ospedale-Università di Padova
QUANDO VENTILARE? CON COSA VENTILARE? Andrea Vianello S.C. Fisiopatologia Respiratoria Ospedale-Università di Padova

2
RESPIRATORY FAILURE HYPOXEMIA HYPERCAPNIA LUNG PUMP FAILURE FAILURE
GAS EXCHANGE FAILURE VENTILATORY FAILURE HYPOXEMIA HYPERCAPNIA

3
What’s the point of ventilation?
Deliver O2 to alveoli Hb binds O2 (small amount dissolved) CVS transports to tissues to make ATP - do work Remove CO2 from pulmonary vessels from tissues - metabolism
 CVS transports to tissues to make ATP - do work. Remove CO2 from pulmonary vessels. from tissues - metabolism.")
4
Why ventilate?- purposes
To maintain or improve ventilation, & tissue oxygenation. To decrease the work of breathing & improve patient’s comfort.

5
When ventilate?- indications
Failure of pulmonary gas exchange Hypoxaemia: low blood O2 “Mechanical” failure Hypercarbia: high blood CO2 Respiratory muscle fatigue Need to intubate eg patient unconscious Others eg need neuro-muscular paralysis to allow surgery cardiovascular reasons

6
Non-Invasive Ventilation
“a form of ventilatory support that avoids airway invasion” Hill et al Crit Care Med 2007; 35:2402-7

7
Terapia medica + O2 q.b. per SpO2 89-92%
Paziente con riacutizzazione acidotica di BPCO Terapia medica + O2 q.b. per SpO %

8
Airway Airway narrowing & Frictional Inflammation obstruction WOB
Shortened muscles curvature Auto- PEEP Elastic WOB Gas trapping muscle strength VCO2 VT VE VA PaCO2 pH PaO2

9
usa i farmaci e bene ! Airway Airway narrowing & Frictional
obstruction Airway Inflammation Steroids Frictional WOB Abx Shortened muscles curvature Auto- PEEP BDs Elastic WOB Gas trapping Teophylline muscle strength VCO2 VT VE VA PaCO2 pH PaO2

10
usa i farmaci e bene ! Airway Airway narrowing & Frictional
obstruction Airway Inflammation Steroids Frictional WOB Abx PEEP Shortened muscles curvature Auto- PEEP BDs Elastic WOB Gas trapping Teophylline MV MV muscle strength VCO2 VT VE MV VA PaCO2 pH PaO2

11
Ripetizione di EGA NIV non indicata
Paziente con riacutizzazione acidotica di BPCO Terapia medica + O2 q.b. per SpO % Ripetizione di EGA NIV non indicata pH > 7.35 >7.30 pH < 7.35 pH < 7.30 pH < 7.20

12
NIV altamente consigliata
NIV consigliata l’80% dei pazienti migliora comunque con terapia standard Ogni 10 pazienti trattati con NIV si evita 1 ETI; NIV migliora la dispnea >7.30 pH < 7.35 NIV altamente consigliata Senza NIV 1 paziente su 2 necessita di ETI NIV migliora la sopravvivenza pH < 7.30 NIV altamente consigliata 1 paziente su 2 fallisce NIV Tuttavia con NIV migliora outcome ospedaliero e sopravvivenza a 1 anno pH < 7.20

13
NIV VS TRATTAMENTO STANDARD
Questi vantaggi si sono tradotti in una riduzione significativa della permanenza in ospedale, ed in una riduzione della fR e miglioramento ad 1 ora degli scambi gassosi (riduzione della PaCO2) Keenan S et al
 Keenan S et al.")
14
NIV VS TRATTAMENTO STANDARD
Keenan S et al

15
NIV VS TRATTAMENTO STANDARD
Keenan S et al

16
The ICU studies Confirm the feasibility of NIV
Confirm the effectiveness of NIV Selected patients / enthusiastic Units Reduced complications - particularly infectious 16% v 48% 1 ,18 v 60% 2 Reduce ICU / Hospital stay 23 v 35 days 1 , 9 v 15 days 2 1. Brochard et al NEJM 1995; 333: Girou et al JAMA 2000; 284:2361-7

17
2005; 128 … ci sono alcune considerazioni su questo lavoro che riguardano: Il fatto di aver in qualche modo selezionato per la randomizzazione solo 64 pazienti su 256 facendo un po’ quello che gli inglesi chiamano “cherry picking” cioè la scelta delle ciliegie migliori dal cestino. In secondo luogo la miscellanea di cause di IRA con una lieve disproporzione tra i 2 gruppi a vantaggio del gruppo NIV per quanto riguarda i sottogruppi di patologie note per essere più responsive alla NIV (IRA da BPCO e edema polmonare). IN sostanza però questo studio ci deve ricordare che: La NIV non è un surrogato della VM per via invasiva e che la NIV rimane inappropriata per molti pazienti con IRA soprattutto quelli con ARDS e MOF Ma che tuttavia la NIV può essere usata con le opportune indicazioni con l’aspettativa di evitare l’intubazione in alcuni pazienti e le sue complicanze Che la NIV deve essere comunque applicata in centri selezionati con esperienza e con la possibilità di rapidamente accedere a strutture per la VM per via invasiva.
. IN sostanza però questo studio ci deve ricordare che: La NIV non è un surrogato della VM per via invasiva e che la NIV rimane inappropriata per molti pazienti con IRA soprattutto quelli con ARDS e MOF. Ma che tuttavia la NIV può essere usata con le opportune indicazioni con l’aspettativa di evitare l’intubazione in alcuni pazienti e le sue complicanze. Che la NIV deve essere comunque applicata in centri selezionati con esperienza e con la possibilità di rapidamente accedere a strutture per la VM per via invasiva.")
18
49 pazienti con IRA in BPCO dopo fallimento terapia medica, pH 7.2
Simili durata di permanenza in ICU, durata VM, complicanze generali, mortalità in ICU, e mortalità in ospedale con NIV 48% evitano ETI, sopravvivono con permanenza in ICU inferiore vs pazienti VM invasiva (P=0.02) A 1 anno: NIV inferiore riospedalizzazione (65% vs 100% P=0.016) e minor frequenza di riutilizzo supplemento di ossigeno (0% vs 36%)
 A 1 anno: NIV inferiore riospedalizzazione (65% vs 100% P=0.016) e minor frequenza di riutilizzo supplemento di ossigeno (0% vs 36%)")
19
Studio caso-controllo: 64 paz. con IRA trattati con NIV pH = 7.18
40/64 (62%) fallimento NIV (RR con NIV - 38%) Simili mortalità in ICU, e mortalità in ospedale; durata di permanenza in ICU e post ICU, ma: Inferiori complicanze (P=0.01) e probabilità di rimanenere in VM (P=0.056) Se NIV efficace (24/64 = 38%) migliore sopravvivenza e ridotta permanenza in ICU vs pazienti VM invasiva NIV riduce necessità di ETI e ospedalizzazione, migliora outcome a lungo termine
 fallimento NIV (RR con NIV - 38%) Simili mortalità in ICU, e mortalità in ospedale; durata di permanenza in ICU e post ICU, ma: Inferiori complicanze (P=0.01) e probabilità di rimanenere in VM (P=0.056) Se NIV efficace (24/64 = 38%) migliore sopravvivenza e ridotta permanenza in ICU vs pazienti VM invasiva. NIV riduce necessità di ETI e ospedalizzazione, migliora outcome a lungo termine.")
20
Definition: What is it? Mechanical Ventilation
=Machine to ventilate lungs = move air in (+ out) Several ways to..move air in (IPPV vs others) Intermittent Positive Pressure Ventilation
 Several ways to..move air in (IPPV vs others) Intermittent Positive Pressure Ventilation.")
22
Definition: What is it? Mechanical Ventilation
=Machine to ventilate lungs = move air in (+ out) Several ways to..move air in (IPPV vs others) Intermittent Positive Pressure Ventilation Several ways to connect the ventilator to the patient
 Several ways to..move air in (IPPV vs others) Intermittent Positive Pressure Ventilation. Several ways to connect the ventilator to. the patient.")
23
Several ways to connect the machine to patient
Oro-tracheal Intubation Tracheostomy Non-Invasive Ventilation

24
Normal breath Normal breath inspiration, awake Lung @ FRC= balance
Diaphragm contracts -2cm H20 Chest volume Pleural pressure -7cm H20 Alveolar pressure falls Air moves down pressure gradient to fill lungs

25
La pompa diaframmatica genera P garantendo la ventilazione polmonare, regolata da:
Equazione di moto del Sistema Respiratorio: Pmusc = V / C + V’ x R

26
Normal breath Normal breath expiration, awake -7cm H20
Diaphragm relaxes Pleural / Chest volume Pleural pressure rises -2cm H20 Alveolar pressure rises Air moves down pressure gradient out of lungs

27
Ventilator breath Portable ventilator ICU ventilator ICU ventilator

28
Ventilator breath Ventilator breath inspiration Air blown in 0 cm H20
lung pressure Air moves down pressure gradient to fill lungs +5 to+10 cm H20 Pleural pressure

29
Pappl (+ Pmusc) = V / C + V’ x R
Il ventilatore sostituisce totalmente o parzialmente la pompa muscolare: Equazione di moto del Sistema Respiratorio: Pappl (+ Pmusc) = V / C + V’ x R
 = V / C + V’ x R.")
30
Ventilator breath Ventilator breath expiration
Similar to spontaneous…ie passive Ventilator stops blowing air in Pressure gradient Alveolus-trachea Air moves out Down gradient Lung volume

31
Practicalities Ventilator settings: Pressure vs volume
‘Assist’ vs ‘Control’ Trigger sensitivity PEEP?

32
Details: Inspiration Pressure or Volume?
Do you push in.. A gas at a set pressure? = ‘pressure…..’ A set volume of gas? = ‘volume….’

33
Details: Inspiration Pressure or Volume?
Pressure cm H20 Time Pressure cm H20 Time

34
Pressure Ventilators The use of pressure ventilators is increasing in critical care units. A typical pressure mode delivers a selected gas pressure to the patient early in inspiration, and sustains the pressure throughout the inspiratory phase. By meeting the patient’s inspiratory flow demand throughout inspiration, patient effort is reduced and comfort increased.

35
Although pressure is consistent with these modes, volume is not.
Volume will change with changes in resistance or compliance Therefore, exhaled tidal volume is the variable to monitor closely. With pressure modes, the pressure level to be delivered is selected, and with some mode options, rate and inspiratory time are preset as well.

36
Details: Inspiration Pressure or Volume?

37
Volume Ventilators The volume ventilator has been historically used in critical care settings A respiratory rate, inspiratory time, and tidal volume are selected for the mechanical breaths. The basic principle of this ventilator is that a designated volume of air is delivered with each breath. The amount of pressure required to deliver the set volume depends on : - Patient’s lung compliance - Patient–ventilator resistance factors

38
Peak Inspiratory Pressure (PIP ) must be monitored in volume modes because it varies from breath to breath 30 Peak Inspiratory Pressure P aw cmH2O Time (s) 1 2 3 -10
")
39
Details: Pressure vs Volume
in the Acute Setting Secretions hypoventilation Vt preserved partial compensation hypoventilation sensitive insensitive Schönhofer ERS Monograph 2001; 16: , mod

40
Details: leak compensation
without leakage with leakage small leak huge leak Pre-set Pressure Vol Pressure Vol Mehta et al. Eur Respir J 2001; 17:

41
Interaction Ventilator Respiratory muscle pump

42
work of breathing Ventilator Respiratory muscle pump .
spontaneous assisted controlled

44
Noninvasive mechanical ventilation in acute exacerbation of restrictive thoracic disease
Eur Respir Mon 2001; 6:70-73

46
4 Phases Inspiratory triggering Inspiration Termination of inspiration
Pressure Flow Volume Time Inspiratory triggering Inspiration Termination of inspiration Expiration Nilsestuen et al. Respir Care 2005; 50:

47
Details: trigger sensitivity
asynchrony insensitive trigger sensitive trigger auto- triggering trigger sensitivity to low high level of PSV hypercapnic encephalopathy sedation sleep intrinsic PEEP (COPD) tubing obstruction trigger sensitivity to high resistance changes tubing leakage cardiac oscillation
 tubing obstruction. trigger sensitivity to high. resistance changes. tubing leakage. cardiac oscillation.")
48
Trigger poco sensibile: allo sforzo inspiratorio non segue l’atto meccanico del respiratore

49
Trigger troppo sensibile: l’atto meccanico si innesca spontaneamente

50
Pao Pes patient 1 patient 2 patient 3

51
Asynchrony between patient and ventilator
Problems: Increased work of breathing Need for sedation „Fighting the ventilator“ Ventilation-Perfusion-Mismatch Dynamic hyperinflation Consequences: Insufficient ventilation Withdrawal from NIV Weaning failure Prolonged ICU stay Costs Prognosis !

53
PSV L’operatore imposta: Caratteristiche: - pressione inspiratoria
- sensibilità trigger - eventuale “rampa” (tempo di raggiungimento PS) L’operatore imposta: - pressure-controlled flow-cycled patient-triggered Caratteristiche: - > sincronismo paziente-ventilatore > comfort - possibile graduazione sforzo inspiratorio
 L’operatore imposta: - pressure-controlled. flow-cycled. patient-triggered. Caratteristiche: - > sincronismo paziente-ventilatore > comfort. - possibile graduazione sforzo inspiratorio.")
54
lenta media rapida Diversi tipi di rampa

55
PSV Problemi: difficoltà di impostazione possibile sovrassistenza
livello PS VT: 6-8ml/Kg; RR: 20-35b/min P0.1: 2-4 cm H2O abolizione dissincronismi toraco addominali possibile sovrassistenza

56
A-CV L’operatore imposta: Caratteristiche: Problemi:
-volume corrente -frequenza respiratoria -rapporto I/E -sensibilità del trigger L’operatore imposta: volume-controlled time-cycled machine e/o patient-triggered (assistito) pressure-limited (eventuale) - volume corrente insufflato garantito - rapporto I/E variabile Caratteristiche: - possibile sovrassistenza alcalosi respiratoria - insorgenza di PEEP intrinseca Problemi:
 pressure-limited (eventuale) - volume corrente insufflato garantito. - rapporto I/E variabile. Caratteristiche: - possibile sovrassistenza alcalosi respiratoria. - insorgenza di PEEP intrinseca. Problemi:")
57
A-CV

58
Volume Assured Pressure Support
Hybrid modes combine the advantages of pressure pre-set and volume pre-set VAPS Volume Assured Pressure Support Automatic adjustment of inspiratory pressure (range setting) Target volume set Measurement of inspiratory pressure and expiratory volume Calculation of missing inspiratory volume Increase of inspiratory pressure Assurance of tidal volume + comfort of pressure pre-set
 Target volume set. Measurement of inspiratory pressure and expiratory volume. Calculation of missing inspiratory volume. Increase of inspiratory pressure. Assurance of tidal volume + comfort of pressure pre-set.")
59
Volume Assured Pressure Support
VAPS Volume Assured Pressure Support

60
Volume Assured Pressure Support
VAPS Volume Assured Pressure Support

61
Storre et al. Chest 2006;130:

62
AVAPS improves quality of ventilation
AVAPS provides elegant adjustments of inspiratory pressures according to a pre-set target volume AVAPS improves quality of ventilation Improvements of sleep quality and quality of life are comparable to BiPAP-S/T However: Sleep quality is not completely normalized Further studies are needed Storre et al. Chest 2006; 130:

63
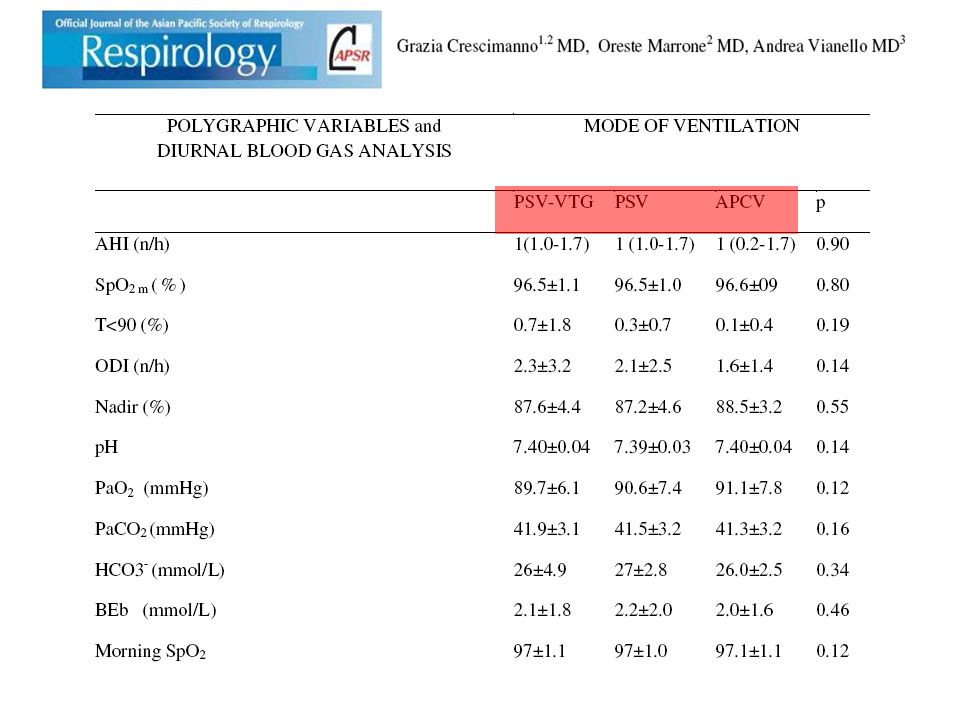
Efficacy and comfort of Volume-Guaranteed Pressure Support (PSV-VTG) in patients with chronic ventilatory failure of neuromuscular origin
 in patients with chronic ventilatory failure of neuromuscular origin")
65
Efficacy and comfort of Volume-Guaranteed Pressure Support (PSV-VTG) in patients with chronic ventilatory failure of neuromuscular origin
 in patients with chronic ventilatory failure of neuromuscular origin")
66
Four types of asynchronies:
Efficacy and comfort of Volume-Guaranteed Pressure Support (PSV-VTG) in patients with chronic ventilatory failure of neuromuscular origin Four types of asynchronies: Ineffective inspiratory effort (IE): thoraco-abdominal displacements not assisted by the ventilator positive pressure boost; Inspiratory trigger delay: a time lag between the initiation of the patent’s IE and the onset of inspiratory support; Prolonged inspiration or late expiratory cycling (hang-up): prolongation of mechanical insufflation beyond the end of patient inspiration; Autotriggering: rapid succession of at least three pressurizations at a RR of >40 br/min.
 in patients with chronic ventilatory failure of neuromuscular origin. Four types of asynchronies: Ineffective inspiratory effort (IE): thoraco-abdominal displacements not assisted by the ventilator positive pressure boost; Inspiratory trigger delay: a time lag between the initiation of the patent’s IE and the onset of inspiratory support; Prolonged inspiration or late expiratory cycling (hang-up): prolongation of mechanical insufflation beyond the end of patient inspiration; Autotriggering: rapid succession of at least three pressurizations at a RR of >40 br/min.")
67
Efficacy and comfort of Volume-Guaranteed Pressure Support (PSV-VTG) in patients with chronic ventilatory failure of neuromuscular origin
 in patients with chronic ventilatory failure of neuromuscular origin")
68
Details: PEEP? Positive End Expiratory Pressure Pressure cm H20 PEEP
Time Positive End Expiratory Pressure

69
Effects of PEEP Normal, Awake Lying down / Paralysis / +- pathology
in expiration alveoli do not close (closing capacity) change size Lying down / Paralysis / +- pathology Lungs smaller, compressed Harder to distend, starting from a smaller volume In expiration alveoli close (closing capacity) PEEP Keeps alveoli open in expiration Danger: applied to all alveoli Start at higher point on ‘compliance curve’
 change size. Lying down / Paralysis / +- pathology. Lungs smaller, compressed. Harder to distend, starting from a smaller volume. In expiration alveoli close (closing capacity) PEEP. Keeps alveoli open in expiration. Danger: applied to all alveoli. Start at higher point on ‘compliance curve’")
70
Effects of PEEP ‘over-distended’ alveoli Compliance= Volume
Pressure Volume Curva pressione/volume del sistema respiratorio. La distensibilità è massima nella zona in cui si respira normalmente: 0.1L/cmH2O. Fenomeno dell’isteresi: forza ad una determinata lunghezza è maggiore in fase di allungamento. energy needed to open alveoli ?damaged during open/closing - abnormal forces Pressure

71
Effects of PEEP Compliance= Volume Pressure Volume
PEEP: start inspiration from a higher pressure ↓?damage during open/closing Pressure Raised ‘PEEP’

72
Regional ventilation: PEEP
Spontaneous, standing ‘over-distended’ alveoli Compliance= Volume Pressure Volume Gradiente di pressione pleurica: 0.2cmH2O/cm dipende da forze elastiche (parete) e forze gravitarie (peso polmone) e genera diversa espansibilità parti polmone Pressure
 e forze gravitarie (peso polmone) e genera diversa espansibilità parti polmone. Pressure.")
73
Regional ventilation: PEEP
Mechanical Ventilation Compliance= Volume Pressure Volume Situazione si modifica quando il soggetto respiri ad un livello dimaggiore espirazione, in cui sono le parti alte ad essere più espansibili. Volume di chiusura: volume al quale si chiudono i bronchioli delle regioni polmonari declivi. In alcuni casi è prossimo ad FRC. Applicazione di PEEP aumenta FRC sopra il volume di chiusura delle vie aeree. Pressure

74
Details: Cardiovascular effects
Compresses Pulmonary vessels Reduced RV outflow Reduced LV inflow

78
Details: Cardiovascular effects
Compresses Pulmonary vessels Reduced LV inflow Cardiac Output: Stroke Volume Blood Pressure = CO x resistance – Blood Pressure Neurohormonal Reduced RV outflow- backtracks to body Head- Intracranial Pressure Others - venous pressure

79
Vent settings to improve <oxygenation>
PEEP Increases FRC Prevents progressive atelectasis and intrapulmonary shunting Prevents repetitive opening/closing (injury) Recruits collapsed alveoli and improves V/Q matching Resolves intrapulmonary shunting Improves compliance Enables maintenance of adequate PaO2 at a safe FiO2 level Disadvantages Increases intrathoracic pressure (may require pulmonary a. catheter) Rupture: PTX, pulmonary edema Common examples of methylation-induced silencing: Imprinted genes (Prader-Willi, Angelmann Syndromes) Inactivated 2nd X chromosome in females DNA methylation results in histone deacetylation, compacted chromatin, and repression of gene activity Methylation can have a profound effect in tumorigenesis by silencing tumor suppressors
 Recruits collapsed alveoli and improves V/Q matching. Resolves intrapulmonary shunting. Improves compliance. Enables maintenance of adequate PaO2 at a safe FiO2 level. Disadvantages. Increases intrathoracic pressure (may require pulmonary a. catheter) Rupture: PTX, pulmonary edema. Common examples of methylation-induced silencing: Imprinted genes (Prader-Willi, Angelmann Syndromes) Inactivated 2nd X chromosome in females. DNA methylation results in histone deacetylation, compacted chromatin, and repression of gene activity. Methylation can have a profound effect in tumorigenesis by silencing tumor suppressors.")
80
PEEP: Indications Clinical Physiological Auto-PEEP
Cardiogenic pulmonary edema (↑ LV preload) Hypoxemia with FIO2 > 0.5 Collapsing alveoli (ARDS, postop atelectasis) Chest wall instability (chest trauma) Physiological PaO2 < 60 mm Hg on FIO2 0.8 PaO2 ↑ < 10 mm Hg with FIO2 F of 0.2 PA-aO2 > 300 on FIO2 1.0 Shunt > 30%
 Hypoxemia with FIO2 > 0.5. Collapsing alveoli (ARDS, postop atelectasis) Chest wall instability (chest trauma) Physiological. PaO2 < 60 mm Hg on FIO PaO2 ↑ < 10 mm Hg with FIO2 F of 0.2. PA-aO2 > 300 on FIO Shunt > 30%")
81
NIV treatment: summary
The ventilator management of NIV is continuously evolving; New ventilators are introduced, offering novel features; Clinical applications have been expanding; Clinicians must make selections that best match the ventilator with the patient’s requirements.

Similar presentations