Download presentation
Presentation is loading. Please wait.

1
Prof. Rosanna Abbate Univ.di Firenze

2
Commonly-used anticoagulant treatments affect several steps of coagulation pathway
Intrinsic pathway Extrinsic pathway XII XIIa TF VII XI XIa VIIa VIIIa Ca2+ PL IXa PS IX Ca2+ Legend PC PCa TM Coagulation mechanisms Xa X Xa Endogenous anticoagulant ATIII Xa Va PL Ca2+ TFPI ATIII Inhibition by heparins IIa II Inhibition by Vitamin K antagonists Fibrinogen Fibrin Clot

3
Anticoagulant drugs currently used
Heparins (standard unfractionated, low molecular weight) Oral anticoagulants (warfarin, acenocumarol) Hirudin (in Italy only for HIT)
 Oral anticoagulants (warfarin, acenocumarol) Hirudin (in Italy only for HIT)")
4
New agents in clinical development: The search for selectivity
Thrombin Inhibitors: DS, Hirudin, Bivalirudin, Argatroban, Melagatran, Ximelagatran IXa inhibitors Xa inhibitors: Pentasaccharide TAP, Antistasin, DX 9065a, DPC 906 Protein C Activators aPC, Thrombomodulin Coagulation Pathway Antithrombotics in development Tissue Factor Pathway Inhibitors TFPI, rNAPc2, VIIa inhibitors Initiation Thrombin generation activity TF/VIIa X IX IXa VIIIa Xa Va II IIa i

5
Vascular tone regulation Vascular release of TPA
Thrombin functions Platelet activation F V and F VIII activation Vascular tone regulation Fibrin formation Cellular migration F XIII activation Mitogenic activity Protein C activation Vascular release of TPA TAFI

6
TROMBINA: siti funzionali
Anion binding exosite II heparin binding site Catalytic site THROMBIN FIBRINOGEN Anion binding exosite I fibrinogen binding site

7
COMPARISON OF INHIBITORY EFFECTS OF HEPARIN ON
FLUID-PHASE ( ) AND FIBRIN-BOUND THROMBIN ( )
 AND FIBRIN-BOUND THROMBIN ( )")
10
Farmaci antitrombinici
AT III HEPARIN MELAGATRAN BSF BIBR 1048 MS THROMBIN HIRUGEN LU 58463 HIRUDIN HIRULOG

11
Ximelagatran The drug has a half-life of about 3 h mandating twice daily administration. The active agent, melagatran, is primarily eliminated via the kidneys. Consequently, its half-life is prolonged in the elderly, reflecting their reduced renal function. The pharmacokinetics and pharmacodynamics of ximelagatran are not influenced by aspirin and ximelagatran does not interfere with drugs that are metabolized by the P450 isozymes CYP2C19, CYP2C9 or CYP3A4 Weitz, et al. Thrombosis Research 106; 2002

12
XIMELAGATRAN (H 376/95) pro-drug oral administration melagatran
tmax melagatran h half life of melagatran h (healthy vol.) bioavailability of melagatran of approx 20% low variability in melagatran exposure dose, time, gender independent no food interaction (minor decrease in AUC <10%)
 bioavailability of melagatran of approx 20% low variability in melagatran exposure. dose, time, gender independent. no food interaction (minor decrease in AUC <10%)")
13
MELAGATRAN subcutaneous dosing bid
rapidly and complete absorption subcutaneously low volume of distribution 0.2 L/kg plasma protein binding <15% not metabolised clearance mainly (80%) renal tmax 0.5 h half life h (healthy subjects) inter-individual variability of AUC low (CV; about 15%) NOT suitable for oral dosing
 renal. tmax 0.5 h. half life h (healthy subjects) inter-individual variability of AUC low (CV; about 15%) NOT suitable for oral dosing.")
14
Melagatran LMW selective direct thrombin inhibitor
Synthetic compound - molecular weight of approx 400 EXOSITE 1 (also binding site of fibrin) THROMBIN ACTIVE SITE
 THROMBIN. ACTIVE SITE.")
15
Melagatran Synthetic compound - mol w of approx 400 -Directed to the Active Site of Thrombin
Hirudin also binding site of fibrin Hirulog Exosite 1 Exosite 1 Exosite 1 Melagatran Thrombin (with indirect blocked active site) H376/95 is an oral prodrug of Melagatran directed to the active site of thrombin • Exosite 1 is the main fibrin binding site of thrombin and is occupied in clot-bound thrombin. The active site, which is responsible for physiological thrombin activity, is free in both circulating and clot-bound thrombin. • Long chain thrombin inhibitors occupy exosite 1 when they bind to thrombin. They therefore have limited activity against clot-bound thrombin. • Melagatran binds to the active site of thrombin but not exosite 1. Both clot-bound and circulating free thrombin are inhibited by Melagatran. Thrombin (with binding to active site) Thrombin (with binding to active site) Adapted from Lefkovits. Circulation 1994;90:1522–1536.
 H376/95 is an oral prodrug of Melagatran directed to the active. site of thrombin. • Exosite 1 is the main fibrin binding site of thrombin and is occupied in clot-bound thrombin. The active site, which is responsible for physiological thrombin activity, is free in both circulating and clot-bound thrombin. • Long chain thrombin inhibitors occupy exosite 1 when they bind to thrombin. They therefore have limited activity against clot-bound thrombin. • Melagatran binds to the active site of thrombin but not exosite 1. Both clot-bound and circulating free thrombin are inhibited by Melagatran. Thrombin (with. binding to active site) Thrombin (with. binding to active site) Adapted from Lefkovits. Circulation 1994;90:1522–1536.")
16
Melagatran

19
Melagatran e’ il metabolita attivo di Ximelagatran
Biodisponibilita’ 20% (dose orale 60 mg, n=12) 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 Ximelagatran - t max 1.5 h - emivita 3 h - eliminazione renale Melagatran Plasma conc. (µmol/l) 2 4 6 8 10 12 Time (h) Eriksson, Blood, 1999
 Ximelagatran. - t max 1.5 h. - emivita 3 h. - eliminazione. renale. Melagatran. Plasma conc. (µmol/l) Time (h) Eriksson, Blood,")
20
Antithrombotic effect and bleeding in a rat model
Thrombus size (AU) Total bleeding time (min) 20 50 Warfarin 40 15 Melagatran 30 10 20 5 Effect 10 Bleeding 0.01 0.1 1 10 Dose (µmol/kg/h) , (µmol/kg/day) Elg M et al, Thromb Res 1999;94:187
 Total bleeding time (min) Warfarin Melagatran Effect. 10. Bleeding Dose (µmol/kg/h) , (µmol/kg/day) Elg M et al, Thromb Res 1999;94:187.")
21
Melagatran/ximelagatran Studi clinici sperimentali
Fase I TEV profilassi FA terapia SCA Melagatran - 22 studi H 376/95 - 24 studi TR2-0002 TR2-0005 METHRO I METHRO II MASCOT I 203 (USA) METHRO III PLATINUM EXPRESS EXULT A EXULT B TR2-0001 THRIVE I THRIVE IV THRIVE III THRIVE II THRIVE V SPORTIF II SPORTIF III SPORTIF IV SPORTIF V ESTEEM
 METHRO III. PLATINUM. EXPRESS. EXULT A. EXULT B. TR THRIVE I. THRIVE IV. THRIVE III. THRIVE II. THRIVE V. SPORTIF II. SPORTIF III. SPORTIF IV. SPORTIF V. ESTEEM.")
22
EXPRESS: disegno dello studio
M e l a g a t r a n sc Ximelagatran orale 24 mg bid (mattino e sera) 2 mg 3 mg 2835 THR/ TKR pts Enoxaparina mg sc qd (ogni sera) sera op sera Tempo h h h h gg sett flebografia follow-up Each administered with matched placebo Treatment: 7-12 days F-up: 4-6 wks Eriksson, JTH 2003
 2 mg. 3 mg THR/ TKR pts. Enoxaparina 40 mg sc qd (ogni sera) sera op sera. Tempo -12 h 0 h 12 h 24 h 8-11 gg. 4-6 sett. flebografia follow-up. Each administered with matched placebo. Treatment: 7-12 days F-up: 4-6 wks. Eriksson, JTH")
23
EXPRESS: TVP Prossimale + PE
RRR = 60% % event 9 RRR=63.2% RRR=67% 8 7 6 melagatran (sc) and ximelagatran (po) 5 4 enoxaparina(sc) 3 2 1 THR interventi TKR Interventi THR+TKR Interventi Eriksson, JTH 2003
 and ximelagatran (po) enoxaparina(sc) THR interventi. TKR Interventi. THR+TKR Interventi. Eriksson, JTH")
24
EXPRESS: TEV totali VTE sintomatico raro RRR=21% RRR=23.6% RRR=29%
% eventi 50 40 RRR=23.6% RRR=29% melagatran (sc) and ximelagatran (po) 30 20 enoxaparina(sc) 10 THR Interventi TKR Interventi THR+TKR Interventi Eriksson, JTH 2003 VTE sintomatico raro
 and ximelagatran (po) enoxaparina(sc) 10. THR Interventi. TKR Interventi. THR+TKR Interventi. Eriksson, JTH VTE sintomatico raro.")
25
EXPRESS: Emorragie Maggiori
Surgery Bleeding Category Enoxaparin Melagatran/ Ximel. THR+ ITT population TKR -Fatal Bleeding -Critical Site -Severe % 3.1% -Other % 9.2% -Non wound related transfusion > 2 units % -Requiring re-operation# 0.4% % -Blood transfusions 61.7% 66.8%* May have occurred during the entire study period * Difference significant for THR, not for TKR Eriksson, JTH 2003

26
Proximal DVT/PE, % (95% Cl) Blood loss during surgery, mL (95% Cl)
Efficacy and safety of (xi)melagatran for prevention of VTE after THR or TKR: analysis of 3 randomized, double-blind studies, to evaluate the influence of time and dose Treatment/ Preoperative dose Proximal DVT/PE, % (95% Cl) Total DVT/PE, % (95% Cl) Bleeding, % (95% Cl) Blood loss during surgery, mL (95% Cl) Melagatran/0 mg (METHRO III) 5.7 (4.4;7.2) 31.0 (28.3;33.7) 1.4 (0.9;2.2) 211.8 (190.3;235.7) Melagatran/2 mg (EXPRESS) 2.3 (1.5;3.3) 20.2 (17.9;22.7) 3.3 (2.4;4.4) 195.4 (175.5;217.6) Melagatran/3 mg (METHRO II) 2.4 (1.0;4.9) 15.1 (11.1;19.8) 4.8 (2.8;7.4) 215.0 (175.0;264.2) LMWH (pooled data) 6.3 (5.4;7.3) 27.1 (25.4;28.8) 1.5 (1.1;2.0) 205.7 (191.6;220.9) A. T. Cohen, ISTH 2003
melagatran for prevention of VTE after THR or TKR: analysis of 3 randomized, double-blind studies, to evaluate the influence of time and dose. Treatment/ Preoperative dose. Proximal DVT/PE, % (95% Cl) Total DVT/PE, % (95% Cl) Bleeding, % (95% Cl) Blood loss during surgery, mL (95% Cl) Melagatran/0 mg (METHRO III) 5.7 (4.4;7.2) 31.0 (28.3;33.7) 1.4 (0.9;2.2) (190.3;235.7) Melagatran/2 mg (EXPRESS) 2.3 (1.5;3.3) 20.2 (17.9;22.7) 3.3 (2.4;4.4) (175.5;217.6) Melagatran/3 mg (METHRO II) 2.4 (1.0;4.9) 15.1 (11.1;19.8) 4.8 (2.8;7.4) (175.0;264.2) LMWH (pooled data) 6.3 (5.4;7.3) 27.1 (25.4;28.8) 1.5 (1.1;2.0) (191.6;220.9) A. T. Cohen, ISTH")
27
EXULT A TRIAL TKR Ximelagatran (24 mg bid) Ximelagatran (36 mg bid)
(++North-America) Ximelagatran (24 mg bid) Ximelagatran (36 mg bid) Warfarin (INR 1.8-3) TKR Each administered with matched placebo Treatment: 7-12 days F-up: 4-6 wks Warfarin initiated the evening of the day of surgery Ximelagatran initiated 12 hrs or more after surgery Francis NEJM 2003
 Ximelagatran (24 mg bid) Ximelagatran (36 mg bid) Warfarin (INR 1.8-3) TKR. Each administered with matched placebo. Treatment: 7-12 days F-up: 4-6 wks. Warfarin initiated the evening of the day of surgery. Ximelagatran initiated 12 hrs or more after surgery. Francis NEJM")
28
EXULT A - Efficacy end points
Warfarin (95% CI) Ximelagatran 24 mg (95% CI) Ximelagatran 36 mg (95% CI) Total VTE and death 27.6% ( ) 24.9% ( ) 20.3% ( )* Proximal VTE and death 4.1% ( ) 2.5% ( ) 2.7% ( ) *p=0.003 RRR 26.4% ARR 7.3% Symptomatic DVT or death < 1% in each group Francis NEJM 2003
 Ximelagatran 24 mg (95% CI) Ximelagatran 36 mg (95% CI) Total VTE and death. 27.6% ( ) 24.9% ( ) 20.3% ( )* Proximal VTE and death. 4.1% ( ) 2.5% ( ) 2.7% ( ) *p=0.003 RRR 26.4% ARR 7.3% Symptomatic DVT or death < 1% in each group. Francis NEJM")
29
EXULT A: Safety end points
Warfarin (95% CI) Ximelagatran 24 mg (95% CI) Ximelagatran 36 mg (95% CI) Major bleeding 0.7% ( ) 0.8% ( ) Major or minor bleeding Minor bleeding 4.5% ( ) 4.0% 4.8% ( ) 4.7% 5.3% ( ) No statistically significant differences for perioperative indicators of bleeding, or wound drainage or appearance Francis NEJM 2003
 Ximelagatran 24 mg (95% CI) Ximelagatran 36 mg (95% CI) Major bleeding. 0.7% ( ) 0.8% ( ) Major or minor bleeding. Minor bleeding. 4.5% ( ) 4.0% 4.8% ( ) 4.7% 5.3% ( ) No statistically significant differences for perioperative indicators of bleeding, or wound drainage or appearance. Francis NEJM")
31
EXULT B TRIAL TKR Ximelagatran (36 mg bid) Warfarin (INR 1.8-3)
(++North-America) Ximelagatran (36 mg bid) Warfarin (INR 1.8-3) TKR Study design very close to EXULT A 2303 pts enrolled, 2299 received at least one dose, 1949 had adequate venography Weitz ISTH 2003
 Ximelagatran (36 mg bid) Warfarin (INR 1.8-3) TKR. Study design very close to EXULT A pts enrolled, 2299 received at least one dose, 1949 had adequate venography. Weitz ISTH")
32
EXULT B: Total VTE and all-cause mortality
End point Warfarin (%) Ximelagatran (%) RRR (%) p Total VTE and all-cause mortality event rate 31.9 22.5 29.3 <0.001 ARR 9.3% (95% CI ) NNT 11 (8-18) A trend was observed to reduction of proximal DVT (4% vs 3.5%) Colwell CW et al. American Society of Hematology; December 6-9, 2003; San Diego, CA.
 Ximelagatran (%) RRR (%) p. Total VTE and all-cause mortality event rate < ARR 9.3% (95% CI ) NNT 11 (8-18) A trend was observed to reduction of proximal DVT (4% vs 3.5%) Colwell CW et al. American Society of Hematology; December 6-9, 2003; San Diego, CA.")
33
EXULT B: Bleeding events
End point Warfarin (%) Ximelagatran (%) p Major bleeding 0.4 1.0 NS Minor bleeding 3.4 4.2 No relevant alterations in liver function tests as in EXULT A Colwell CW et al. American Society of Hematology; December 6-9, 2003; San Diego, CA.
 Ximelagatran (%) p. Major bleeding NS. Minor bleeding No relevant alterations in liver function tests as in EXULT A. Colwell CW et al. American Society of Hematology; December 6-9, 2003; San Diego, CA.")
34
(Xi)melagatran in chirurgia ortopedica maggiore
USA Xi 24 mg x2 = enoxa 30 x2 in TKR Xi 24 mg x2 = W in TKR Xi 24 mg x2 < enoxa 30 x2 in THR Xi 36 mg x2 > W in TKR (EXULT) M 3 mg pre e 3mg post + Xi 24 mg x2 > dalte 5000 x1 ma > emorragie in THR+TKR M 2 mg pre e 3mg post + Xi 24 mg x2 > enoxa 40 x1 in THR+TKR (EXPRESS) M 3mg post + Xi 24 mg x2 = enoxa 40 x1 in THR+TKR Europa D Prisco 2004
 M 3 mg pre e 3mg post + Xi 24 mg x2 > dalte 5000 x1 ma > emorragie in THR+TKR. M 2 mg pre e 3mg post + Xi 24 mg x2 > enoxa 40 x1 in THR+TKR (EXPRESS) M 3mg post + Xi 24 mg x2 = enoxa 40 x1 in THR+TKR. Europa. D Prisco")
35
Timing of initial administration of prophylaxis against deep vein thrombosis in patients following hip or knee surgery (Hull 2003) Quadratic fit for study OR for DVT vs. the number of hrs from surgery for the first dose of the antithrombotic regimen. Peak efficacy ranges between 2 h preop and 6-8 h postop.

36
DVT treatment, THRIVE I - Study design
Ximelagatran 24 mg oral bid n=68 N=350 DVT pts Ximelagatran 36 mg oral bid Multicentre, randomised, controlled, parallel group, dose-finding n=65 R Ximelagatran 48 mg oral bid n=73 Ximelagatran 60 mg oral bid n=71 Dalteparin sc + warfarin n=73 Visit 1 Visit 2 Visit 3 Visit 14 Visit 5 Pre-entry Day 3-5 Day 6-9 Day 12-16 Day 26-32 Phlebography Phlebography Follow-up Adv Ev Eriksson H et al. J Thromb Haemost 2003; 1: 41-7.

37
THRIVE I - treatment of patients with DVT Ximelagatran (24 - 60 mg bid) vs warfarin + dalteparin
Efficacy: Change in Marder score units at 14 days (n=295) 24 mg 36 mg 48 mg 60 mg W/D 10 20 30 40 50 60 70 <-5 [-5 to +5] >5 Patients % Total bleeding: Ximelagatran (12 %, no dose response), W/D (10 %) Eriksson H et al. J Thromb Haemost 2003; 1: 41-7.
 24 mg. 36 mg. 48 mg. 60 mg. W/D <-5. [-5 to +5] >5. Patients % Total bleeding: Ximelagatran (12 %, no dose response), W/D (10 %) Eriksson H et al. J Thromb Haemost 2003; 1:")
38
THRIVE I- Conclusions:
H 376/95 in DVT Flat dose-response Broad therapeutic interval No severe bleedings Use without monitoring supported

39
THRIVE II: design of the study
Warfarin or H 376/95 n= 1241 H 376/95 36 mg b.i.d. + Placebo Warfarin/Enoxaparin stratification R 37% enrolled pts with PE Placebo H 376/95 + Warfarin/Enoxaparin E Enoxaparin (1 mg/Kg bid) End of Treatment 24 hours n= 1250 max 14 days Until INR 2.0 at two consecutive measurements ( days of Enoxaparin) 6 Month 14 days follow up Objective confirmation of DVT and/or PE onset of symptoms of DVT of lower limbs +/- PE
 End of Treatment. 24 hours. n= max 14 days. Until INR 2.0 at two consecutive measurements. ( days of Enoxaparin) 6 Month. 14 days follow up. Objective confirmation of DVT and/or PE. onset of symptoms of DVT of lower limbs. +/- PE.")
40
THRIVE II: results Event Ximelagatran n (%*) Enoxa/warfarin n (%*)
Absolute difference ximel: enoxa/w (%*; 95% Cl) Recurrent VTE (ITT) 26 (2.1%) 24 (2.0%) +0.2%** (-1.0%; + 1.3%) Recurrent VTE (OT) 23 (2.0%) 17 (1.5%) +0.5% (-0.6%; + 1.6%) All-cause mortality (ITT) 28 (2.3%) 42 (3.4%) -1.0%** (-2.4%; + 0.2%) Major bleeding (OT) 14 (1.3%) 25 (2.2%) -0.9% (-2.0%; + 0.2%) Recurrent VTE and/or major bleeding (OT) 37 (3.2%) 42 (3.6%) -0.4% (-1.9%; + 1.1%) *Estimated cumulative risk; **rounded figures; CI = confidence interval; ITT = intention-to-treat; OT = on-treatment
 Recurrent VTE (ITT) 26 (2.1%) 24 (2.0%) +0.2%** (-1.0%; + 1.3%) Recurrent VTE (OT) 23 (2.0%) 17 (1.5%) +0.5% (-0.6%; + 1.6%) All-cause mortality (ITT) 28 (2.3%) 42 (3.4%) -1.0%** (-2.4%; + 0.2%) Major bleeding (OT) 14 (1.3%) 25 (2.2%) -0.9% (-2.0%; + 0.2%) Recurrent VTE and/or major bleeding (OT) 37 (3.2%) 42 (3.6%) -0.4% (-1.9%; + 1.1%) *Estimated cumulative risk; **rounded figures; CI = confidence interval; ITT = intention-to-treat; OT = on-treatment.")
41
Volume 349: October 30, 2003 Number 18 Secondary Prevention of Venous Thromboembolism with the Oral Direct Thrombin Inhibitor Ximelagatran Sam Schulman, M.D., Karin Wåhlander, M.D., Torbjörn Lundström, M.D., Solveig Billing Clason, M.Sc., Henry Eriksson, M.D., for the THRIVE III Investigators

42
THRIVE III: disegno dello studio
ITT population Initial VTE event Ximelagatran (24 mg, b.i.d., p.o.) Stratification - malignancy 617 patients n=612 E R 616 patients n=611 Placebo Stop of study treatment INR<1.5 Standard anticoagulation Study treatment 6 ±1 months 18 months 2 weeks follow up Leg US scan + perfusion lung scan at baseline Schulman, NEJM 2003
 Stratification - malignancy. 617 patients. n=612. E. R. 616 patients. n=611. Placebo. Stop of study treatment. INR<1.5. Standard anticoagulation. Study treatment. 6 ±1 months. 18 months. 2 weeks follow up. Leg US scan + perfusion. lung scan at baseline. Schulman, NEJM")
43
THRIVE III: TEV totali - TVP e/o EP (ITT population)
Estimated cumulative risk (%) 2 4 6 8 10 12 14 12.6% P<0.0001 HR=0.16 (95%CI 0.09; 0.30) 9.8% 3 6 9 12 15 18 Months Ximelagatran Placebo 2.8% Schulman, NEJM 2003
 % P< HR=0.16 (95%CI 0.09; 0.30) 9.8% Months. Ximelagatran. Placebo. 2.8% Schulman, NEJM")
44
THRIVE III: Emorragie maggiori e minori (ITT population)
Estimated cumulative risk (%) 30 25 P= (NS) HR=1.19 (95%CI 0.93; 1.53) 21.0% 23.9% 20 15 Ximelagatran 10 Placebo 5 3 6 9 12 15 18 Months Schulman, NEJM 2003
 P= (NS) HR=1.19 (95%CI 0.93; 1.53) 21.0% 23.9% Ximelagatran. 10. Placebo Months. Schulman, NEJM")
45
Ridker PM et al, N Engl J Med 2003

46
THRIVE III Placebo Ximelagatran Emorragie maggiori * 0.8% 1.0% Morti
Morti +TEV 1.2% 13.3% 3.9% HR 0.23 Aumento ALT (>3 x limite superiore normale) 6.4%**HR 6.5 *nessuna fatale o intracranica ** Senza iperbilirubinemia, massimo valore osservato 25 x, mesi, transitorio, andamento indipendente da sospensione ximelagatran o meno, non segni o sintomi, non spiegabile con caratteristiche di pazienti o farmaci associati Schulman, NEJM 2003
 6.4%**HR 6.5. *nessuna fatale o intracranica. ** Senza iperbilirubinemia, massimo valore osservato 25 x, mesi, transitorio, andamento indipendente da sospensione ximelagatran o meno, non segni o sintomi, non spiegabile con caratteristiche di pazienti o farmaci associati. Schulman, NEJM")
47
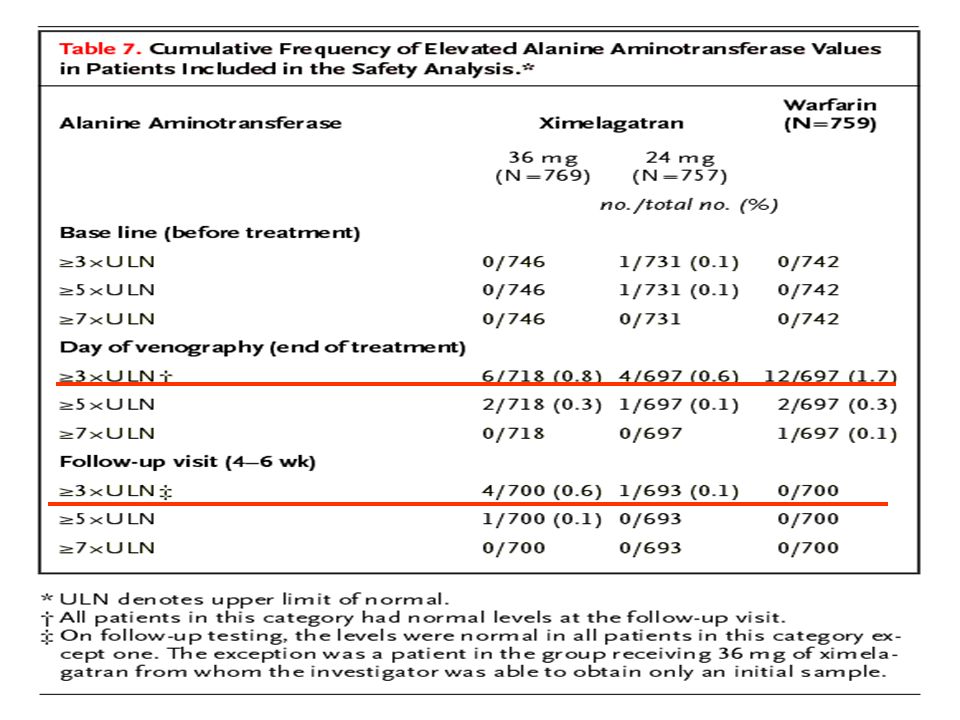
Time Courses of Elevations in the Alanine Aminotransferase Level in Patients Receiving Ximelagatran in Whom the Values Exceeded Three Times the Upper Limit of Normal at Least Once Diamonds represent the last observation in a given patient; dotted lines represent patients in whom treatment with ximelagatran was discontinued. The highest peak shows the maximal elevation in a patient with positive serologic-test results for Epstein–Barr virus infection. The outlying peak near 360 days shows the maximal elevation in a patient with a gall-bladder concrement. Schulman, NEJM 2003

48
® Fibrillazione atriale – Fase III Ximelagatran 36 mg bid Warfarin
Fino a 27 mesi 3000 paz. “resto del mondo” open label, : SPORTIF III 3000 paz. USA & Canada double-blind, double-dummy, sham INR : SPORTIF V

49
Stroke Prevention using an ORal Thrombin Inhibitor in atrial Fibrillation (SPORTIF III)
Lancet 2003;362:

50
The SPORTIF III Study Warfarin ximelagatran Adjusted-dose (INR 2-3)
Fixed-dose ximelagatran (36 mg b.i.d.) Nonvalvular atrial fibrillation patients with at least one aditional risk factor for stroke n=3 407 Randomised, parallel group, open-label treatment allocation, blinded event assessment 23 countries, 259 centers Exposure: mean 17 months, 4941 patient-years and 96 primary endpoints. Primary objective: To establish the non-inferiority of ximelagatran compared to dose-adjusted warfarin (INR ) for prevention of all strokes and/or systemic embolic events in patients with nonvalvular paroxysmal or persistent atrial fibrillation and 1 adjunctive risk factor for stroke
 Nonvalvular atrial fibrillation patients with. at least one aditional risk factor for stroke. n= Randomised, parallel group, open-label treatment allocation, blinded event assessment. 23 countries, 259 centers. Exposure: mean 17 months, 4941 patient-years and 96 primary endpoints. Primary objective: To establish the non-inferiority of ximelagatran compared to dose-adjusted warfarin (INR ) for prevention of all strokes and/or systemic embolic events in patients with nonvalvular paroxysmal or persistent atrial fibrillation and 1 adjunctive risk factor for stroke.")
51
Paragone di vari eventi compositi
SPORTIF III, Lancet 2003;362:

52
SPORTIF III Stroke e/o embolia sistemica (intention to treat)
56 eventi (2.3%/anno) 1 2 3 4 p=0.10 40 eventi (1.6%/anno) Eventi cumulativi (%) Warfarin Ximelagatran 3 6 9 12 15 18 21 Durata (mesi) Presented at ACC 2003
 p= eventi (1.6%/anno) Eventi cumulativi (%) Warfarin. Ximelagatran Durata (mesi) Presented at ACC")
53
Eventi avversi maggiori (on treatment analysis)
Eventi (% per anno) Warfarin 14 RRR=25% p = 0.022 Ximelagatran 12 10 8 6.1% 6 4.6% 4 2 Eventi primari + emorragie maggiori + morte Presented at ACC 2003
 Warfarin. 14. RRR=25% p = Ximelagatran % % Eventi primari + emorragie maggiori + morte. Presented at ACC")
54
Altri eventi avversi Aumento enzimi epatici
Warfarin 14 Ximelagatran 12 10 p <0.001 8 6.5% 6 4 2 0.7% ALT >3x limite sup. norma Presented at ACC 2003

55
The SPORTIF V Study Warfarin Ximelagatran Adjusted-dose (INR 2-3)
Fixed-dose Ximelagatran (36 mg bid) Nonvalvular atrial fibrillation patients with at least one aditional risk factor for stroke n=3 922 Randomised, double-blind, double-dummy, sham INR, blinded endpoint assessment USA and Canada, 409 centers Exposure: mean 20 months, 6405 patient-years and 88 primary endpoints. SPORTIF V, the largest stroke prevention study in atrial fibrillation to date, including 3922 patients with moderate to high risk for stroke is a further landmark study comparing the first oral in a new class of direct thrombin inhibitor ximelagatran with dose-adjusted warfarin. The key results of SPORTIF III, which involved open-label treatment according to the same protocol, were reported earlier this year. The protocol stipulated a minimum exposure of 12 months per patient, an aggregate follow-up of more than 4,000 patient-years, and at least 80 patients with verified primary events. The primary analysis was based on intention-to-treat and compared the combined rates of all strokes (ischemic or hemorrhagic) and systemic embolic events in patients assigned to ximelagatran with those assigned to warfarin. Although the SPORTIF program included two independently powered trials, the analysis plan also called for pooling the event rates from both to examine the relative effects of warfarin and ximelagatran on events occurring at low frequencies. The efficacy of warfarin in patients with atrial fibrillation made a placebo control unethical. Hence the study was designed to evaluate whether ximelagatran was at least as effective as warfarin within a pre-specified margin of 2% for the difference in primary event rates. Primary objective: To establish the non-inferiority of fixed-dose ximelagatran compared to dose-adjusted warfarin (INR ) for prevention of all strokes and/or systemic embolic events in patients with nonvalvular paroxysmal or persistent atrial fibrillation and 1 adjunctive risk factor for stroke
 Nonvalvular atrial fibrillation patients with. at least one aditional risk factor for stroke. n= Randomised, double-blind, double-dummy, sham INR, blinded endpoint assessment. USA and Canada, 409 centers. Exposure: mean 20 months, 6405 patient-years and 88 primary endpoints. SPORTIF V, the largest stroke prevention study in atrial fibrillation to date, including 3922 patients with moderate to high risk for stroke is a further landmark study comparing the first oral in a new class of direct thrombin inhibitor ximelagatran with dose-adjusted warfarin. The key results of SPORTIF III, which involved open-label treatment according to the same protocol, were reported earlier this year. The protocol stipulated a minimum exposure of 12 months per patient, an aggregate follow-up of more than 4,000 patient-years, and at least 80 patients with verified primary events. The primary analysis was based on intention-to-treat and compared the combined rates of all strokes (ischemic or hemorrhagic) and systemic embolic events in patients assigned to ximelagatran with those assigned to warfarin. Although the SPORTIF program included two independently powered trials, the analysis plan also called for pooling the event rates from both to examine the relative effects of warfarin and ximelagatran on events occurring at low frequencies. The efficacy of warfarin in patients with atrial fibrillation made a placebo control unethical. Hence the study was designed to evaluate whether ximelagatran was at least as effective as warfarin within a pre-specified margin of 2% for the difference in primary event rates. Primary objective: To establish the non-inferiority of fixed-dose ximelagatran compared to dose-adjusted warfarin (INR ) for prevention of all strokes and/or systemic embolic events in patients with nonvalvular paroxysmal or persistent atrial fibrillation and 1 adjunctive risk factor for stroke.")
56
SPORTIF V - Stroke ed embolismo sistemico (Intention to treat)
Eventi cumulativi (%/anno) 1 2 3 4 5 7 6 Warfarin Ximelagatran 51 events (1.6%/anno) p=0.13 37 eventis (1.2%/anno) The SPORTIF V study met its primary objective of non-inferiority for ximelagatran in prevention of stroke and other thromboembolic complications when compared to well-controlled, dose-adjusted warfarin. 3 6 9 12 15 18 21 24 Mesi Ximelagatran Warfarin
 Warfarin. Ximelagatran. 51 events (1.6%/anno) p= eventis (1.2%/anno) The SPORTIF V study met its primary objective of non-inferiority for ximelagatran in prevention of stroke and other thromboembolic complications when compared to well-controlled, dose-adjusted warfarin Mesi. Ximelagatran Warfarin")
57
SPORTIF (Analisi intention to treat)
Ximelagatran meglio Warfarin meglio -0.66 SPORTIF III +0.45 SPORTIF V -0.03 Pooled When the entire SPORTIF phase III program is considered, ximelagatran is consistently associated with a low rate of thromboembolism, 1.6% per year. In patients assigned to warfarin, the event rate in the SPORTIF V trial is about half that in SPORTIF III, despite similar clinical risk profiles and anticoagulation intensity. The reason for this apparent disparity in warfarin efficacy is not clear, but patient, laboratory or other clinical factors may be responsible, or simply the play of chance. Taken individually, each of the large-scale SPORTIF trials satisfies the criteria in the primary analyses to establish the noninferiority of ximelagatran compared to warfarin. -1.5 -1 -0.5 0.5 1 1.5 2 Differenza assoluta nella frequenza di eventi (Ximelagatran – Warfarin)
")
58
SPORTIF V - Emorragie (Analisi on treatment)
Eventi (% /anno) Warfarin 50 47% Ximelagatran 40 37% 30 20 In the SPORTIF V study, rates of intracranial haemorrhage (ICH) are low with either treatment. Neither is there a significant difference between the groups in rates of major bleeding. A major haemorrhage was either fatal, affected a critical anatomical site, required transfusion, or decreased haemoglobin by 2 grams per decilitre. When minor as well as major events are counted, however, patients randomised to ximelagatran have significantly less bleeding then those given warfarin. p=0.16 NS 10 3.1% 2.4% 0.1% 0.1% Cerebrali Maggiori Maggiori + minori
 Warfarin % Ximelagatran % In the SPORTIF V study, rates of intracranial haemorrhage (ICH) are low with either treatment. Neither is there a significant difference between the groups in rates of major bleeding. A major haemorrhage was either fatal, affected a critical anatomical site, required transfusion, or decreased haemoglobin by 2 grams per decilitre. When minor as well as major events are counted, however, patients randomised to ximelagatran have significantly less bleeding then those given warfarin. p=0.16. NS % 2.4% 0.1% 0.1% Cerebrali. Maggiori. Maggiori + minori.")
59
SPORTIF V - aumento transaminasi ALT >3 x val. normale
50 Warfarin Ximelagatran 40 38 35 30 Numero di pazienti 20 An elevation of ALAT>3XULN was observed in 6% of patients treated with ximelagatran, a consistent level to that seen in other long-term ximelagatran studies. As before, these elevations were typically transient (occurring within fist 2-6 months), decreased towards baseline with treatment continuation or discontinuation and not typically associated with specific clinical symptoms. 10 10 7 6 4 4 3 3 2 2 2 2 2 2 1 1 1 1 1 1 1 1 1 1 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 Mesi
, decreased towards baseline with treatment continuation or discontinuation and not typically associated with specific clinical symptoms Mesi.")
60
Wallentin L et al, Lancet 2003; 362:789-97
Oral ximelagatran for secondary prophylaxis after myocardial infarction. The ESTEEM randomised controlled trial Wallentin L et al, Lancet 2003; 362:789-97

61
ESTEEM Study Wallentin L et al. Lancet 2003; 362: 789–97
Dose-finding, doppio cieco, controllato con placebo in 1883 pazienti con recente infarto del miocardio Ximelagatran 24 mg, 36 mg, 48 mg, or 60 mg 2 volte/die, per 6 mesi Tutti i pazienti ricevevano anche ASA 160 mg Obiettivi primari: mortalità generale, infarto non fatale, recidiva ischemica grave

62
ESTEEM Study Wallentin L et al. Lancet 2003; 362: 789–97
Rischio cumulativo di morte, infarto e stroke. Pool di tutte le dosi di ximelagatran, analisi “intention-to-treat”

63
ESTEEM- Emorragie Wallentin L et al. Lancet 2003; 362: 789–97

64
ESTEEM - Conclusioni Wallentin L et al, Lancet 2003; 362:789-97
L’associazione ximelagatran-ASA è più efficace del solo ASA nella prevenzione di eventi cardiovascolari maggiori nei 6 mesi successivi ad infarto del miocardio

65
What will the future bring us?
Studies so far demonstrate that (xi)melagatran has predictable pharmacokinetic characteristics in volunteers and in patients and has a wider therapeutic window than warfarin. (Xi)melagatran treatment does not need any lab monitoring However, no antidote is available for overdosage and the relevance of increase in ALT has to be clarified
melagatran has predictable pharmacokinetic characteristics in volunteers and in patients and has a wider therapeutic window than warfarin. (Xi)melagatran treatment does not need any lab monitoring. However, no antidote is available for overdosage and the relevance of increase in ALT has to be clarified.")
Similar presentations












 of these drugs should be the one(s) I use, and for what?>")





 No significant increase in rate of major hemorrhage 0 20 40 60 ESSENCE n = 3171 TIMI 11B n = 3910.>")

 Apixaban (oral) Betrixiban (oral) Edoxaban (oral)>")


