Download presentation
Presentation is loading. Please wait.

1
The Role of Diagnostic Imaging in Appendicitis
D. Joseph Grunz, MD Department of Radiology Mercy Children’s Hospital- St. Louis

2
Objectives Discuss current topics and role of diagnostic imaging for evaluation of appendicitis Discuss controversies regarding specific imaging techniques, especially regarding multi-detector computed tomography and ultrasound Discuss current preferences and imaging strategies

3
CT vs. US Benefits of CT studies Downside of CT studies
Rapid evaluation High degree of diagnostic confidence High degree of reproducibility Evaluation of other etiologies Decreased negative laparotomy and perforation rates Downside of CT studies Radiation concerns IV contrast usage

4
CT vs. US Benefits of ultrasound Downside of ultrasound
No use of radiation Evaluation of pelvic disease in girls Can localize to site of pain Downside of ultrasound Not on site after hours Lower degree of diagnostic confidence Lower degree of reproducibility Limited evaluation of other etiologies

5
CT Findings Normal appendix- blind ending tubular structure with air

6
CT Findings Dilated tubular fluid structure with contrast-enhancing walls, possible appendicolith

7
US Findings Normal appendix, compressible, less than 6 mm in thickness

8
US Findings Abnormal appendix, non-compressible, increased vascular flow, fluid-filled

9
Choosing Wisely American College of Radiology- Five Things Physicians and Patients Should Question 1. Don’t do imaging for uncomplicated headache. 2. Don’t image for suspected pulmonary embolism (PE) without moderate or high pre-test probability. 3. Avoid admission or preoperative chest x-rays 4. Don’t do computed tomography (CT) for the evaluation of suspected appendicitis in children until after ultrasound has been considered as an option. 5. Don’t recommend follow-up imaging for clinically inconsequential adnexal cysts.
 without moderate or high pre-test probability. 3. Avoid admission or preoperative chest x-rays. 4. Don’t do computed tomography (CT) for the evaluation of suspected appendicitis in children until after ultrasound has been considered as an option. 5. Don’t recommend follow-up imaging for clinically inconsequential adnexal cysts.")
10
ACR-Choosing Wisely Although CT is accurate in the evaluation of suspected appendicitis in the pediatric population, ultrasound is nearly as good in experienced hands. Since ultrasound will reduce radiation exposure, ultrasound is the preferred initial consideration for imaging examination in children. If the results of the ultrasound exam are equivocal, it may be followed by CT. This approach is cost-effective, reduces potential radiation risks and has excellent accuracy, with reported sensitivity and specificity of 94 percent.

11
The way we were 1981 1988 Computed tomography? It will never last!
R. Brooke Jeffrey- early US advocate Goal was to reduce unnecessary laparotomy rates Establish criteria to exclude appendicitis Take home point- US appendix has been around a long time.

12
Are We Resistant to New Technology?
PACS technology CT angiography CT perfusion CT urography CT 3D reformat CT coronary artery MR enterography MR angiography MR cholangiogram US pyloric channel US sonohysterography US musculoskeletal

13
Intussusception Standard of care was barium enema reduction

14
Intussusception Air insufflation enema adopted

15
Intussusception Ultrasound

16
Come and gone Intravenous pyelography Plain film tomography
Herniography Venography CT colonoscopy CT screening for cancer

17
Not yet or never were US gastro-esophageal reflux
US voiding cystourethrography US malrotation/midgut volvulus US intussusception reduction US with IV contrast

18
It’s not over until … CT pulmonary angiogram vs. V/Q scan
Fluoroscopic voiding cystourethrogram vs. nuclear medicine voiding cystourethrogram CT angiography vs. MR angiography vs. conventional angiography MR lumbar spine vs. CT lumbar spine myelography

19
“When the facts change, I change my mind. What do you do, sir?”
― John Maynard Keynes

20
1999-2000 Increased reliance on CT for diagnosis of pediatric appendicitis
95 % sensitivity, 94 % specificity Alternate diagnosis in 34 %

22
USA Today 2001 Children are exposed to unnecessary radiation doses for CT studies. Children are receiving adult radiation settings for CT studies CT studies should be calibrated for child age/size

23
23

24
New England Journal of Medicine, Nov. 2007
“The largest increases in CT use have been in the categories of pediatric diagnosis and adult screening.” “There is direct evidence from epidemiologic studies that the organ doses corresponding to a common CT study (two or three scans, resulting in a dose in the range of 30 to 90 mSv) result in an increased risk of cancer. The evidence is reasonably convincing for adults and very convincing for children.” *Brenner, D. et al. NEJM 357, , Nov. 29, 2007
 result in an increased risk of cancer. The evidence is reasonably convincing for adults and very convincing for children. *Brenner, D. et al. NEJM 357, , Nov. 29,")
25
Children are at higher risk to develop cancer because…
Children are more radiosensitive Children have a longer lifespan for cancer to develop

26
Increased ED utilization 2000-2006

27
Public Awareness (?)
")
29
2011 Articles There has been significantly increased utilization of CT scans in the pediatric emergency room setting. Based upon population studies, if 1.6 million CT studies are performed, there is a theoretical risk that 1,500 children will develop a fatal neoplasm as a result Did not conclude these exams were unnecessary, but such was the implication

30
Back to Ultrasound Stats

31
Sweden (2002) Children US sensitivity 86%, specificity 95%
CT sensitivity 80%, specificity 97% Prevalence of 41% Negative predictive value of 92%

32
High sensitivity study- Kessler, France (2004)
125 patients, appendicitis prevalence of 46% Appendix identified in 86% of patients Appendix identified in 96% of patients with appendicitis Appendix identified in 72% of patients without appendicitis Negative predictive value of 90% if appendix not visualized

33
Meta-analysis study (2006)
US sensitivity 88%, specificity 94% for children CT sensitivity 94%, specificity 95% for children

34
Our experience Matches CT experience of other institutions
Nowhere close to the ultrasound percentages for finding the appendix, making the diagnosis, or excluding the diagnosis

35
"When you unwrap a Reggie bar, it tells you how good it is
"When you unwrap a Reggie bar, it tells you how good it is." - Catfish Hunter

36
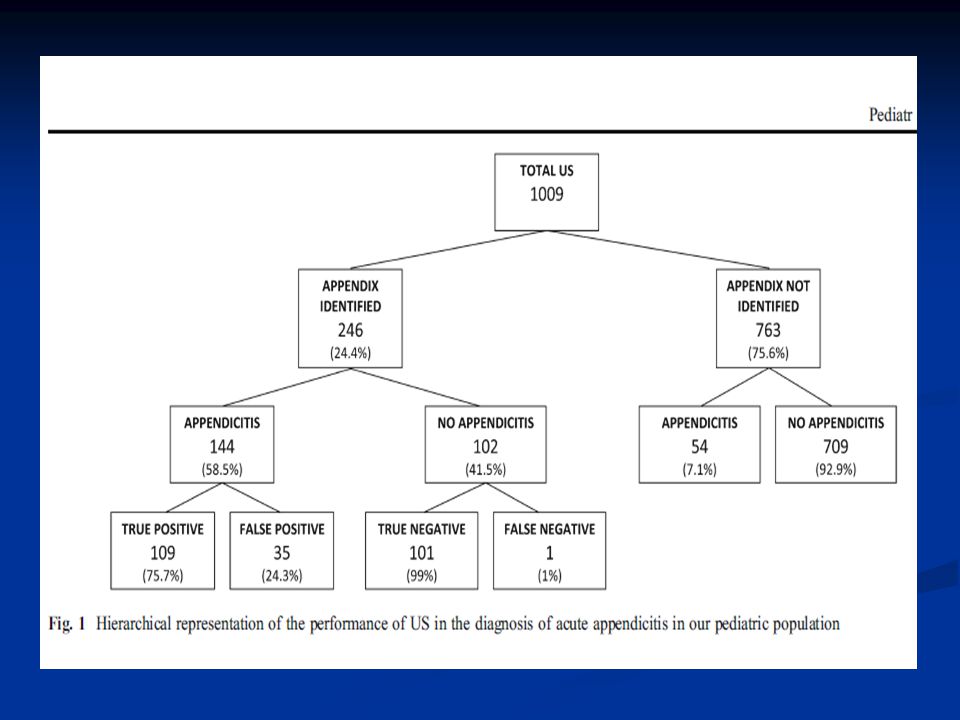
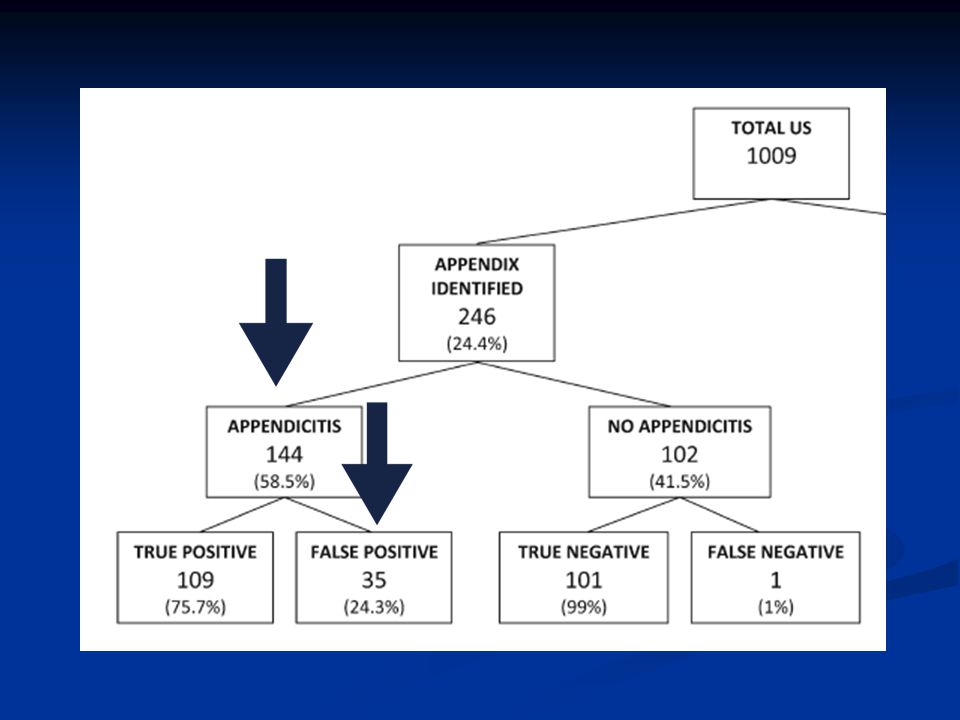
University of Michigan, Pediatric Radiology, March 2012
Observed their experience doesn’t correspond as well as described in the literature Identified the appendix 24% of the time.

40
What to do?

41
Understand the Issues for the ED physicians

42
ED Issues Safe, reliable, available diagnostic exam for appendicitis is highly desirable Discharge home or admission for observation is frequently undesirable Unstable social situation Long travel distance Rapid clinical deterioration Pain control Limited hospital beds Malpractice issues

43
Risks of Appendicitis Most common acute abdominal condition requiring childhood surgery Commonly missed or delayed diagnosis Complications include peritonitis, sepsis, bowel obstruction, death Second most common cause for litigation, and one third of claims involve diagnostic error

44
Put risks into perspective
Lifetime cancer risk is 44.00% for men, 38.00% for women Single CT scan for a child age five theoretically increases that risk 00.02% Physicians need to understand the risk/benefit Risk of missed diagnosis is immediate and real Risk of radiation exposure is delayed and theoretical Eliminate unnecessary exams, not necessary exams

45
Estimated Lifetime Risk of Death
Lightning strike Bicycle accident Drowning Motor vehicle accident Cancer (natural causes) Cancer, pediatric (single CT) 1 in 100,000 1 in 10,000 1 in 1,000 1 in 100 1 in 3-4 1 in ,000
 Cancer, pediatric (single CT) 1 in 100, in 10, in 1, in in in ,000.")
46
Understand institutional/population bias
Patient population Prevalence of obesity Relevant for US vs. CT Social/cultural conditions Time of presentation/need for follow-up Age/gender of patients Younger children/adolescent females Institution resources/support

47
My biases Awareness of cancer risks associated with pediatric CT need to be raised Alternatives to CT studies need to be explored If there is a low pre-test probability, neither ultrasound nor CT study is an appropriate diagnostic imaging examination If there is mid to high pre-test probability, and it will likely change the course of treatment, CT is the study of choice for appendicitis

48
Pre-test probability

49
My bias against ultrasound
There is still controversy about this exam, decades after introduction, even among highly qualified radiologists The appendix is not found in ¾ of all examinations When the appendix is not found, appendicitis can’t be excluded When the appendix is found and appendicitis suspected, there is still a false positive rate of 25% The immediate risk of patient harm from missed ultrasound diagnosis is much more compelling than the theoretical risk (and lower) long-term risk from medical radiation
 long-term risk from medical radiation.")
50
My bias in favor of CT studies
If the appendix is seen and normal, no appendicitis If the appendix is not seen, but no other abnormalities identified, very low chance of appendicitis If the appendix is inflamed, then surgery If the appendix is not seen but inflammation present, follow closely

51
Trends for the future Better physician and patient education
Clinical decision rules to minimize need for imaging Awareness of the issues and time constraints upon ED physicians for rapid diagnosis Development of alternatives to CT studies Technical alteration of CT protocols to minimize radiation exposure

52
Conclusions

53
Conclusions There is still controversy concerning diagnostic imaging for appendicitis in pediatric patients We are pro-active in keeping medical radiation exposure as low as reasonable achievable The experience with our pediatric population, emergency room physician expectations for accuracy, and surgical follow-up has led us to recommend CT studies for appendicitis in the appropriate clinical setting

Similar presentations




: Department.>")
 Director of Evidence-Based Practice, Quality Management Assistant Professor,>")


 in adults has grown rapidly. Although.>")












 LECT7 ALI B ALHAILIY.>")
