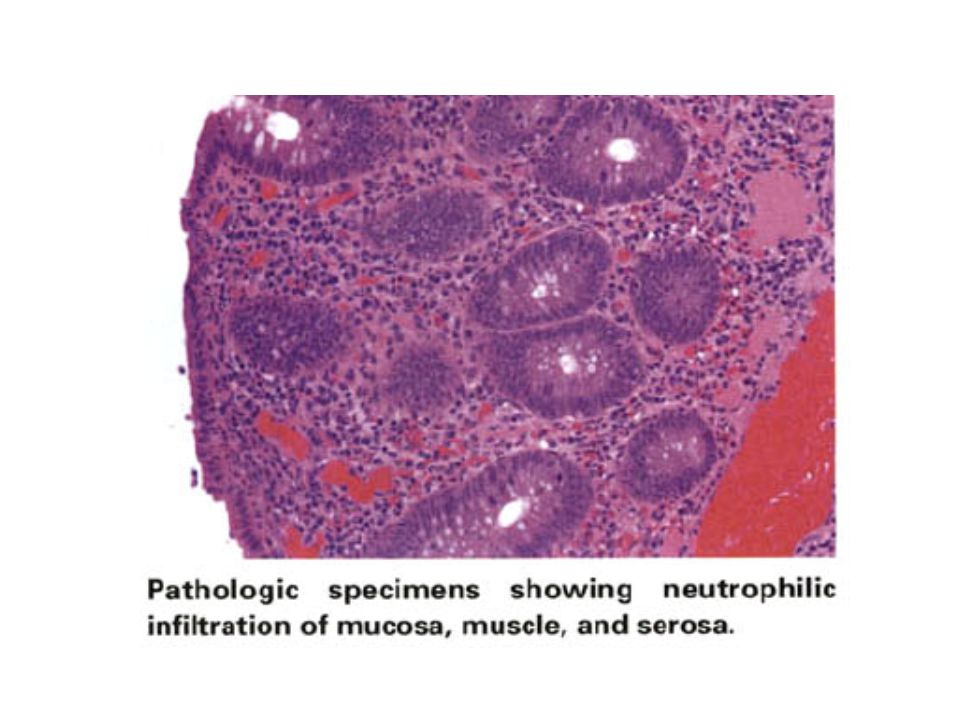
Download presentation
Presentation is loading. Please wait.

1
APPENDICITIS - WHAT WE ALL FORGOT (or never knew in the first place!)
")
2
APPENDICITIS History Berengario DaCarpi, a physician-anatomist,
made the first description of the appendix in 1521 Leonardo DaVinci demonstrated the appendix in drawings made in 1492 but not published until the 18th century. Lorenz Heister gave the first unequivocal account of appendicitis in 1711 The appendix is clearly illustrated in De Humani Corporis Febrica Liber V by Andreas Vesalius published in 1543 Vesalius A. De Humani Corporis Fabrica Liber V. Basel: Iohannis Oporini; 1543.

3
APPENDICITIS History Heister, a student of Boerhaave, described a perforation of the appendix with a small abscess adjacent to a gangrenous appendix Heister speculated that the appendix might be the site of acute inflammation. He described the autopsy on the body of a criminal Francois Melier, a Parisian physician, described 6 cases of appendicitis at autopsy and first suggested the possibility of removing the appendix in 1827

4
APPENDICITIS History Claudius Amyand, Sergeant Surgeon to George II, performed the first known appendectomy in He operated on an 11-year-old boy with a right scrotal hernia and a fistula. He identified the appendix, perforated by a pin, within the scrotum. He ligated the appendix and removed it. Shepherd JA. Acute appendicitis: a historical survey. Lancet 1954;2:

5
APPENDICITIS History Fitz – 1886
Proposed that the appendix is the cause of most inflammatory disease of the right lower quadrant. He went on to describe the clinical features of appendicitis and, importantly, proposed early surgical removal of the appendix Fitz RH. Perforating inflammation of the vermiform appendix: with special reference to its early diagnosis and treatment. Am J Med Sci 1886;92:

6
APPENDICITIS History In 1889, McBurney of New York published the first of several important papers regarding the appendix. He suggested early operative intervention and developed the muscle-splitting incision that bears his name and is commonly used today McBurney C. Experience with early operative interference in cases of disease of the vermiform appendix. NY Med J 1889;50: McBurney C. The incision made in the abdominal wall in cases of appendicitis, with a description of a new method of operation. Ann Surg 1894;20:38-43.

7
APPENDICITIS Introduction Lifetime risk – 6% to 7%
Peak age – Adolescents and young adults Uncommon <5 and >50 yrs 1 in 35 men 1 in 50 women Male:Female 1.3:1

8
APPENDICITIS Introduction
More common in industrialised nations (refined, low fibre diet) Presumably, this diet leads to hard stool, higher intracolic pressure and faecolith formation Familial association is simply due to similar environment and dietary habits
 Presumably, this diet leads to hard stool, higher intracolic pressure and faecolith formation. Familial association is simply due to similar environment and dietary habits.")
9
APPENDICITIS Pathophysiology Small lumen to length ratio
Predisposed to closed loop obstruction, especially with proximal swelling or faecolith Ongoing mucosal secretion leads to elevated intraluminal pressure Venous pressure is exceeded and ischaemia develops Hypoxic mucosa begins to ulcerate Bacterial translocation

11
APPENDICITIS Clinical Features
Begins as peri-umbilical discomfort – poorly localised and unrelieved by stools. Loss of Appetite (80%) Nausea (+- vomiting) Diarrhoea (uncommon) 6-12 hours later localised to RIF (localised peritonism) Less tenderness in retrocaecal or pelvic appendix Pyrexia (37.5 to 38) – 25% to 50% have temp <37.5
 Nausea (+- vomiting) Diarrhoea (uncommon) 6-12 hours later localised to RIF (localised peritonism) Less tenderness in retrocaecal or pelvic appendix. Pyrexia (37.5 to 38) – 25% to 50% have temp <37.5.")
12
APPENDICITIS Clinical Features Leukocytosis…
Cardall and colleagues showed that fever and leukocytosis were not always present and cannot be wholly relied upon in the diagnosis Pieper and colleagues reported 493 patients in which only 67% had a leukocyte count greater than 11.0 CRP Cardall T, Glasser J, Guss DA. Clinical value of the total white blood cell count and termperature in the evaluation of patients with suspected appendicitis. Acad Emerg Med 2004;11:1021-7 Pieper R, Kager L, Nasman P. Acute appendicitis: a clinical study of 1018 cases of emergency appendectomy. Acta Chir Scand 1982;48:51-62.

13
APPENDICITIS Clinical Features

14
APPENDICITIS Clinical Features PSOAS SIGN
The psoas sign. Pain on passive extension of the right thigh. Patient lies on left side. Examiner extends patient's right thigh while applying counter resistance to the right hip. Anatomic basis for the psoas sign: inflamed appendix is in a retroperitoneal location in contact with the psoas muscle, which is stretched by this manoeuvre.

15
APPENDICITIS OBTURATOR SIGN
Pain on passive internal rotation of the flexed thigh. Examiner moves lower leg laterally while applying resistance to the lateral side of the knee resulting in internal rotation of the femur. Anatomic basis for the obturator sign: inflamed appendix in the pelvis is in contact with the obturator internus muscle, which is stretched by this manoeuvre.

16
Perforation - Clinical Features
APPENDICITIS Perforation - Clinical Features Occurs in 20%-30% Longer duration of symptoms before presentation Age <3yrs and >50yrs Increasing abdominal pain (severity and sight) Temperature > 38 The morbidity of a negative appendectomy is preferable to the morbidity of perforated appendicitis
 Temperature > 38. The morbidity of a negative appendectomy is preferable to the morbidity of perforated appendicitis.")
17
Peri-appendiceal Abscess - Clinical Features
APPENDICITIS Peri-appendiceal Abscess - Clinical Features Occurs in 10% Scenario – Develops RIF pain and fever for 1-2 days then resolves, then recurs 7-10 days later Palpable mass Ultrasound or CT to confirm diagnosis Avoid surgery if possible, especially if appendix is difficult to find (discussed later)
")
18
Recurrent Appendicitis
Debatable existence Sinanan has shown it to be a real entity Recurrent attacks of RIF pain If interval appendectomy not done after medical Rx, 10-80% recurrence Histology in recurrent pain pts- chronic AND acute inflammation Sinanan M. Acute Abdomen and Appendix. In: Greenfield LJ, Mulholland MW, Oldham KT, Zelenock GB, editors. Surgery: Scientific Principles and Practice. Philadelphia: JB Lippincott; 1993, pp

19
APPENDICITIS Chronic Appendicitis Chronic RIF pain
If appendectomy relieves pain, and histology shows chronic inflammation – Diagnosis is made retrospectively

20
Atypical Presentations
APPENDICITIS Atypical Presentations 3 factors… 1) Extremes of age 2) Variable appendiceal position 3) Associated conditions (e.g. pregnancy, Crohn’s, antibiotics, steroids, recent abdominal surgery)
 Extremes of age. 2) Variable appendiceal position. 3) Associated conditions (e.g. pregnancy, Crohn’s, antibiotics, steroids, recent abdominal surgery)")
21
Atypical Presentations
APPENDICITIS Atypical Presentations 3 factors… 1) Extremes of age Age 1-5 has 70% perforation rate Age < 1yr has almost 100% perforation rate REASONS… Communication Shorter, incompletely formed omentum
 Extremes of age. Age 1-5 has 70% perforation rate. Age < 1yr has almost 100% perforation rate. REASONS… Communication. Shorter, incompletely formed omentum.")
22
Atypical Presentations
APPENDICITIS Atypical Presentations 3 factors… 3) Associated conditions (e.g. pregnancy, Crohn’s, antibiotics, steroids, recent abdominal surgery) Pregnancy causes delays in diagnosis Abdominal pain, nausea, vomiting, leukocytosis all ‘normal’ for pregnancy Appendix moves to RUQ in 3rd trimester
 Associated conditions (e.g. pregnancy, Crohn’s, antibiotics, steroids, recent abdominal surgery) Pregnancy causes delays in diagnosis. Abdominal pain, nausea, vomiting, leukocytosis all ‘normal’ for pregnancy. Appendix moves to RUQ in 3rd trimester.")
23
Differential Diagnosis
APPENDICITIS Differential Diagnosis CHILDREN… Extra-abdominal – (Otitis, pneumonia, meningitis, URTI – can all present with abdominal pain, nausea, vomiting. Diarrhoea – usually suggestive of gastroenteritis Mesenteric Lymphadenitis Meckel’s diverticulitis Intussusception (Tender mass and red-currant stools) Typhlitis (neutropaenic child)
 Typhlitis (neutropaenic child)")
24
APPENDICITIS Imaging A SHORT NOTE…
If the diagnosis is apparent from the history, examination and lab findings – then surgery is indicated without imaging. Imaging is reserved for doubtful diagnosis

25
APPENDICITIS Imaging PLAIN RADIOGRAPHS… Faecolith (5-8%)
Gas in the appendix Localised paralytic ileus Loss of caecal shadow Blurring of R Psoas R scoliosis of lumbar spine Free air (rare)
")
26
APPENDICITIS Imaging PLAIN RADIOGRAPHS…
Study of 821 patients… no x-ray was sensitive or specific Use to rule out other condition (obstruction, renal calculus, perforation) Overall – not cost effective Rao PM, Rhea JT, Rao JA, Conn AK. Plain abdominal radiography in clinically suspected appendicitis: diagnostic yield, resource use, and comparison with CT. Am J Emerg Med 1999;17:325-8.
 Overall – not cost effective. Rao PM, Rhea JT, Rao JA, Conn AK. Plain abdominal radiography in clinically. suspected appendicitis: diagnostic yield, resource use, and comparison with CT. Am J Emerg Med 1999;17:")
27
APPENDICITIS Imaging ULTRASOUND
Deutsch and Leopold visualised appendix in 1981 Graded pressure technique (compresses the bowel overlying the appendix) Immobile, non-compressible, blind-ending structure consisting of an anechoic lumen surrounded by an echogenic mucosa and hypoechoic thickened wall adjacent to the caecum. Deutsch A, Leopold GR. Ultrasonic demonstration of the inflamed appendix: case report. Radiology 1981;140:163-4.
 Immobile, non-compressible, blind-ending structure consisting of an anechoic lumen surrounded by an echogenic mucosa and hypoechoic thickened wall adjacent to the caecum. Deutsch A, Leopold GR. Ultrasonic demonstration of the inflamed appendix: case. report. Radiology 1981;140:")
28
APPENDICITIS Imaging ULTRASOUND
The diagnostic accuracy of graded compression ultrasound has been reported to range from 71% to 97%, with sensitivities and specificities in the 76% to 96% and 47% to 94% ranges, respectively Operator dependent Normal appendix must be visualised to rule out appendicitis (60-82%) Retrocaecal appendix difficult to visualise
 Retrocaecal appendix difficult to visualise.")
29
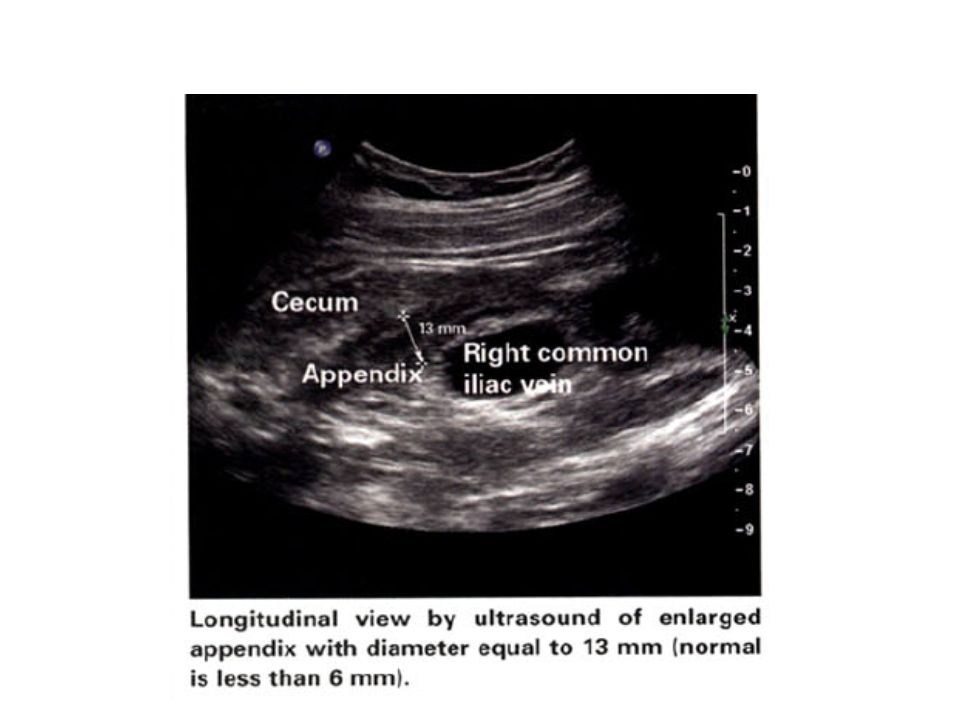
APPENDICITIS Imaging ULTRASOUND Appendicitis features –
Appendiceal diameter > 6-7mm (sensitivity 100%, specificity 64%) Target sign Loculated peri-caecal fluid (rupture) Appendicolith Absence of gas in appendix lumen
 Target sign. Loculated peri-caecal fluid (rupture) Appendicolith. Absence of gas in appendix lumen.")
31
APPENDICITIS Imaging ULTRASOUND - summary Disadvantages…
Low specificity Discomfort for patient with probe pressure Advantages… Inexpensive Non-invasive No radiation Can find other abdominal pathology

32
APPENDICITIS Imaging CT SCAN… Accuracy of 93-98% Sensitivity 87-100%
Specificity 95-99% Enlarged appendix Appendiceal wall thickening Peri-appendiceal fat stranding Appendiceal wall enhancement Rao PM, Rhea JT, Novelline RA. Sensitivity and specificity of the individual CT signs of appendicitis: experience with 200 helical appendiceal CT examinations. J Comput Assist Tomogr 1997;21:

33
APPENDICITIS Imaging CT SCAN… Study of 908 patients…
Drop in perforation rate (22% to 14%) Drop in negative appendectomy rate (20% to 7%) Rao P, Rhea JT, Rattner DW, Wenus LG, Novelline RA. Introduction of appendiceal CT: impact on negative appendectomy and appendiceal perforation rates. Ann Surg 1999;229:344-9. .
 Drop in negative appendectomy rate (20% to 7%) Rao P, Rhea JT, Rattner DW, Wenus LG, Novelline RA. Introduction of. appendiceal CT: impact on negative appendectomy and appendiceal perforation. rates. Ann Surg 1999;229:")
34
APPENDICITIS Imaging CT vs. ULTRASOUND… CT advantages…
Higher diagnostic accuracy Operator independence CT Disadvantages Contrast problems Radiation Cost

36
APPENDICITIS Antibiotics Large meta-analysis of 9576 patients
Proven to prevent wound infection and intra-abdominal abscess Cover Gram negative and anaerobic organisms Andersen BR, Kallehave FL, Andersen HK. Antibiotics versus placebo for prevention of postoperative infection after appendicectomy. Cochrane Database Syst Rev 2004;4:1-64

37
APPENDICITIS Surgery Generally indicated unless…
Symptoms resolved when patient presents Peri-appendiceal abscess without peritonitis – percutaneous drainage Interval appendectomy Optimise patient before surgery

38
APPENDICITIS Open Appendectomy Normal appendix?
Check Caecum, ileum (and sigmoid) for diverticular disease. Check for Meckel’s Gall Bladder Iiflammatory Bowel Disease Perforated Duodenal Ulcer GUT (females – PID, follicular cysts, ectopic) Mesenteric lymphadenpathy NB – if ++ pus, full exploration required
 for diverticular disease. Check for Meckel’s. Gall Bladder. Iiflammatory Bowel Disease. Perforated Duodenal Ulcer. GUT (females – PID, follicular cysts, ectopic) Mesenteric lymphadenpathy. NB – if ++ pus, full exploration required.")
39
APPENDICITIS Open Appendectomy Normal appendix?
Do appendectomy anyway (presence of the scar, etc.) Exception is diseased caecum (e.g. Crohn’s) where a fecal fistula may form
 Exception is diseased caecum (e.g. Crohn’s) where a fecal fistula may form.")
40
Peri-appendiceal Abscess
APPENDICITIS Peri-appendiceal Abscess CT or Sonar guided percutaneous catheter 7-10 days of drainage Interval appendectomy at 6-8 weeks If laparotomy done… Open abscess Appendectomy only if safe If caecum friable, leave it and do interval appendectomy (10% to 80% risk of recurrence)
")
41
Laparoscopic Appendectomy
APPENDICITIS Laparoscopic Appendectomy Kurt Semm 1983 Major meta-analysis, still major controversy Dependent on expertise and equipment Allows for better visualisation of the abdomen

42
Laparoscopic Appendectomy
APPENDICITIS Laparoscopic Appendectomy CONTRA-INDICATIONS… Lack of surgeon’s experience Inability to tolerate GA Refractory coagulopathy Diffuse peritonitis with haemodynamic compromise Previous abdominal surgery (relative) Portal Hypertension (relative) Advanced pregnancy (relative) Severe cardiac failure (relative)
 Portal Hypertension (relative) Advanced pregnancy (relative) Severe cardiac failure (relative)")
43
Selected randomized trials of laparoscopic versus open appendectomy
Reference number OR Time Conversion rate(%) LOS <days> L O Long et al (2002) 93 105 107 91 16 2.6 3.4 Pedersen et al (2001) 282 301 60 40 23 2 Ozmen et al (1999) 35 28 38 — 1.6 3.7 Hellberg et al (1999) 244 256 12 Heikkinen et al (1998) 19 21 31 41 5.3 Klinger et al. (1998) 87 82 3 4 Reiertsen et al (1997) 42 51 25 3.5 3.2 Minne et al (1997) 27 67 7.4 1.1 1.2 Macarulla et al (1997) 106 104 55 45 8.3 4.8 Ortega et al (1995) 167 86 68 58 6.5 2.8
 LOS <days> L. O. Long et al (2002) Pedersen et al (2001) Ozmen et al (1999) — Hellberg et al (1999) Heikkinen et al (1998) Klinger et al. (1998) Reiertsen et al (1997) Minne et al (1997) Macarulla et al (1997) Ortega et al (1995)")
44
Laparoscopic Appendectomy
APPENDICITIS Laparoscopic Appendectomy Laparoscopic longer by minutes 5% - 25% conversion Hospital stay same or 1 day in favour of laparoscopic Return to normal activity 5-7 days earlier Results of complication rates mixed No difference in cost (equipment/length vs. hospital stay) ‘Jury is still out
 ‘Jury is still out.")
Similar presentations