Download presentation
Presentation is loading. Please wait.

1
Approach in Vascular Patient
กิตติพันธุ์ ฤกษ์เกษม PhD, FACA

2
Topic Artery - Limb Ischaemia Venous - Varicose vein - Aneurysm
Leg ulcer

3
Limb Ischaemia Aetiology: most often atherosclerosis > trauma
Most management decisions are based upon 1.Differentiation acute vs chronic 2. Mechanism of occlusion 3.Location of the occlusion 4.Status of limb 5.Fitness of patients

4
1.Differentiation acute vs chronic

5
What is acute ischaemia?

6
Acute ischaemia Period of onset in minutes or hours
Sudden catastrophic Less effect in upper extremity and leg affected by chronic ischaemia

7
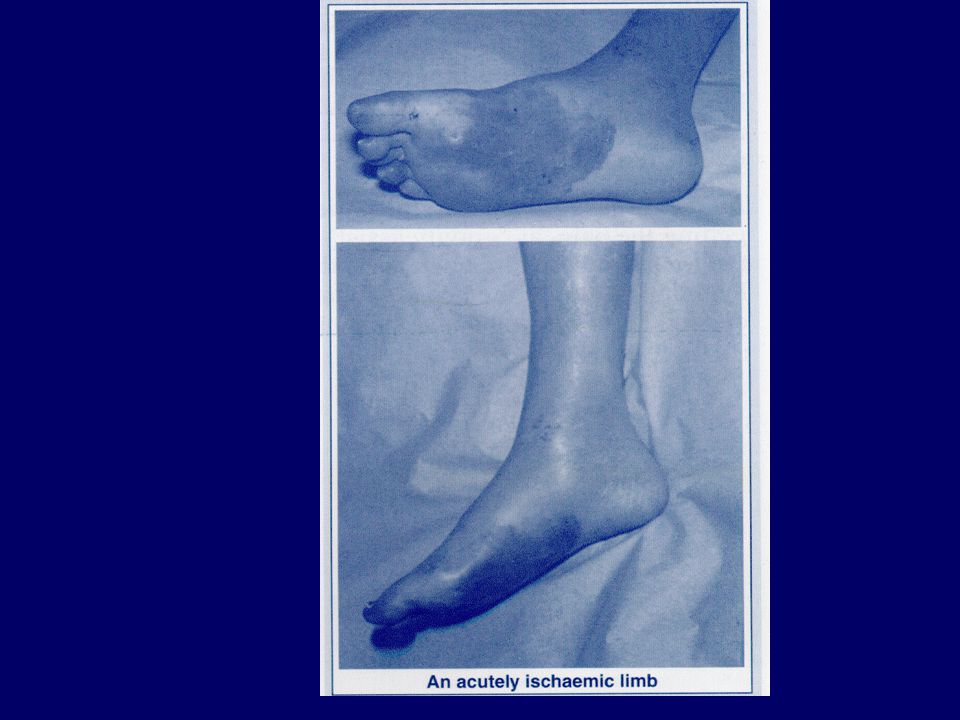
Acute ischaemia Symptom 5P pain pulselessness paresthesia pallor
paralysis

8
Marble white right foot in acute limb ischaemia

9
What is chronic ischaemia?

10
Chronic ischaemia Symptom of limited circulation over months or years
Slow deterioration of function Gradually symptom Life style changes-stop smoking or exercise: remission collateral vv

11
Chronic ischaemia Symptom and sign Claudication rest pain
ulceration/gangrene

12
Why should the effectes of acute arterial ischaemia occlusion be less in someone affected already by symptom of chronic ischaemia or in upper limb?

13
Collateral vessels!!

15
2. Mechanism of occlusion
Acute iscahemia caused by Trauma Non trauma - embolus - thrombosis

16
Trauma-fracture tibia

17
Embolus Mobile solid mass Free floating in blood
Capable of occluding a vein or artery distal to its site of origin

18
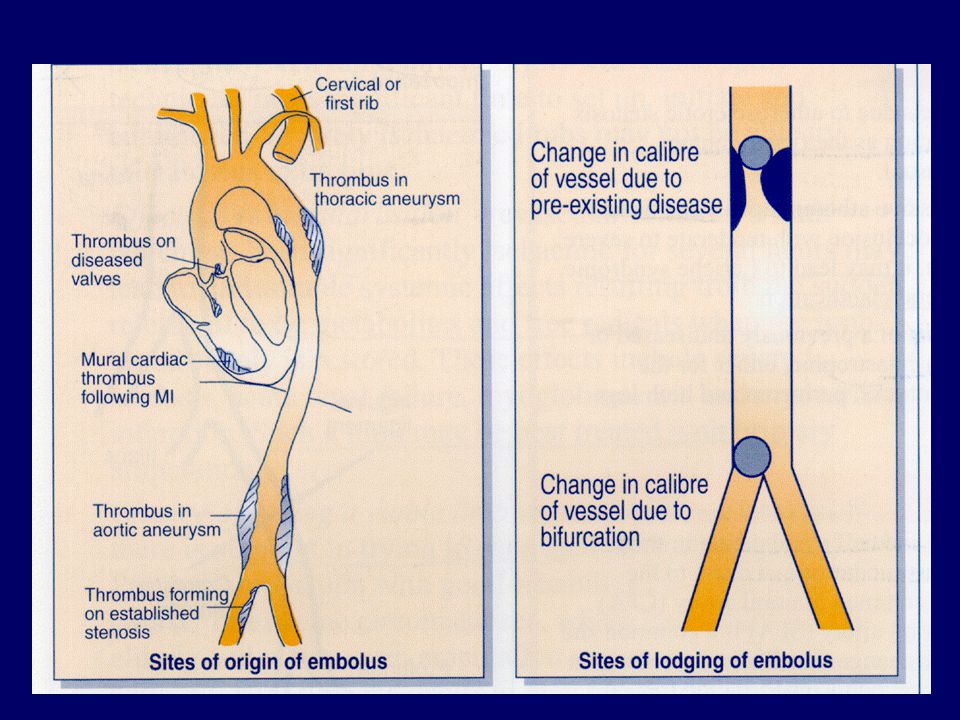
Composition of embolus
Atheromatous debris or thrombus(clot) (common)
 (common)")
19
Common source of atheromatous or thrombus emboli
Left ventricle wall after MI Left atrium in atrial fibrillation Diseased mitral valve or aortic valve Atheromatous plaques in aorta or iliac vessels This embolus lodge at the area where arterial tree is smaller than the embolus e.g. bifurcation or pre-existing stenosis

21
Atheromatous debris-blue toe syndrome

22
Thrombosis Rupture of an atheromatous plaque esp moderate and severe stenosis Virchow’s triad: abnormality of flow, blood, vessel wall

23
Is it possible to differentiate between thrombosis and embolus as a cause of acute ischaemia??
Sometimes!!! Previously asymptomatic, preexisting cause with sudden onset of severe ischaemia (normal contralateral pulse) = embolus Previous claudication and sudden onset of acute ischaemia = thrombosis
 = embolus. Previous claudication and sudden onset of acute ischaemia = thrombosis.")
24
Chronic ischaemia Progressive narrowing
Cause : Atheromatous disease is the common cause Other uncommon cause: Aneurysm: popliteal aneurysm: special nature Diabetes Some rare disease Buerger’s disease Hyperhomocysteineaemia Takayasu’s disease

25
3. Location Acute occlusion: more proximal, the more extensive ischaemia Diagnostic location determines the best treatment

26
3. Location-aorto-iliac disease
Chronic: claudication at buttock, thigh calf, loss of femoral pulse in men: Leriche syndrome (French surgeon who described distal aortic occlusion and erectile impotence) Acute: catastrophic for ipsilateral limb, buttock, perineum
 Acute: catastrophic for ipsilateral limb, buttock, perineum.")
27
Distal aorta occlusion

28
Location Common femoral disease
Chronic: thigh and calf claudication, palpable the femoral pulse just below inguinal ligament Acute: femoral bifurcation is the common site of embolus-typical ischaemic limb

29
Location-superficial femoral disease
Chronic :a very common place for stenosis or occlusion where it passes posteriorly through adductor hiatus (Hunter’s canal) It can produce calf claudication, but rarely severe in presence of profunda femoris artery Acute: rare
 It can produce calf claudication, but rarely severe in presence of profunda femoris artery. Acute: rare.")
30
Bilateral occlusion of superficial femoral artery with collateral circulation via profunda

31
Location-popliteal atery dsease
Chronic: calf claudication Acute: sudden occlusion from thrombus or embolus causes severe ischaemia due to occlusion geniculate arteries

32
Location: crural arterial disease
Occlusion only one out of three vessel can asymptom unless either chronic or acute disease involve all three vessels

33
4. Status of the limb-acute iscahemia
Determine chance of saving limb vs amputation Pain: severe pain not response to opiate with tenderness in muscle:often irreversible ischaemia Paresthesia: range from percentible alternation to numbness. Numbness indicate acute critical ischaemia Pallor: pale > unfixed mottling -> fixed mottling (do not blanch on pressure) frequently beyond salvage
 frequently beyond salvage.")
34
4. Status of the limb-acute ischaemia
Pulselessness Paralysis: stiff of the limb, when patient cannot move ankle joint indicated severe ischaemia

36
4. Status of the limb –chronic ischaemia
Early calf claudication like angina i.e.tight, stiff or crushing pain

37
What factors influence claudication distance?
Anything increases work of walking Excess weight Walking uphill Walking against wind Carry shopping

38
More severe form Very short distance- a few steps
Rest pain first felt in the distal parts such as toes and dorsum of the foot – awake patient need rise from bed and walking around to relieve Unable to lie flat without pain patient sleep with hanging leg out of beds cause edema and worsen microvascular perfusion

39
Hanging foot

40
Last stage of chronic Gangrene, clinical depend on the degree of decomposition Range from ulcer (skin necrosis) to gangrene of toe and foot Gangrene: wet gangrene: black, soggy, discoloured green and malodorous requires urgent amputation Dry gangrene: black hard, brittle, wrinkle rarely odour : may autoamputation or surgery in proper time

41
5. Fitness of patient Determine investigation and treatment
“ surgeon need to consider the ability of the patient to withstand our effort. Our job should be relieve the symptom of which the patient complain” Common causes of unfitness - pre-event unfitness: cardiac e.g. MI, Lung-renal-metabolic disease - per-event unfitness: dehydration, acidosis, uncontrolled DM - postevent unfitness: myoglobinaemia, severe acidosis, MI

42
Investigation of occlusive disease
Clinical examination: full history Presence or absence of pulse Status of the limb Other test BUN, CR, electrolyte CBC, plasma viscosity Coagulation EKG, CXR

43
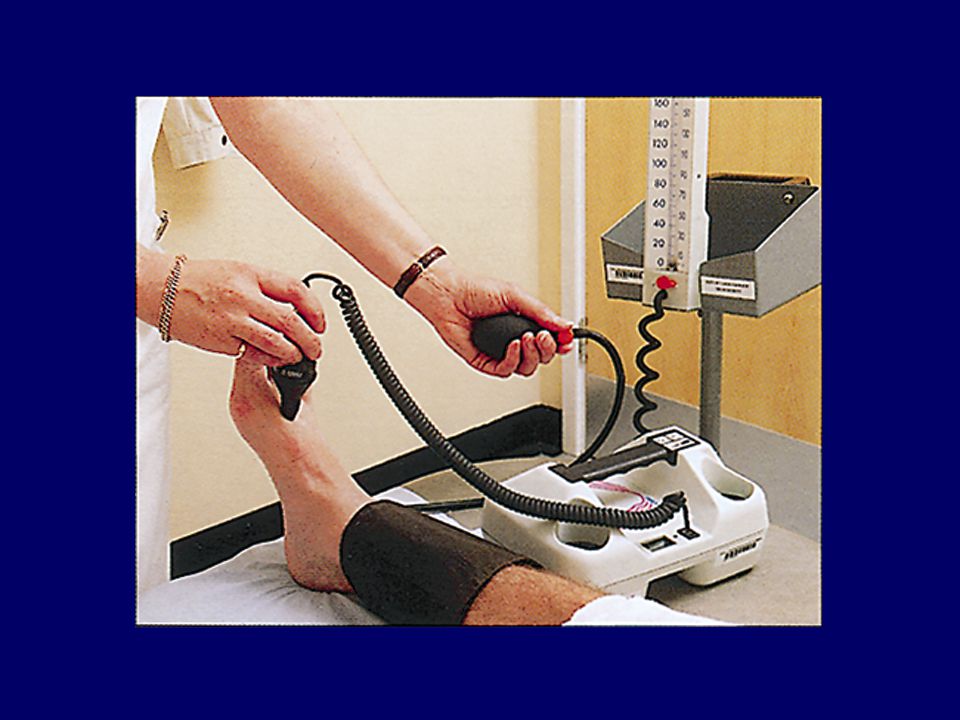
Fixed wave Doppler examination
Ankle brachial pressure index (ABPI) claudication < 0.5 critial limb ischaemia < 0.3 gangrene
 claudication. < 0.5 critial limb ischaemia. < 0.3 gangrene.")
45
Treadmill testing Walking incline 10% at speed 3 km/hr
Test of function to allow monitoring disease and the result of therapeutic effort

46
Ultrasound-duplex scan
Composed of 1. B-mode ultrasound reveal the anatomy:aneurysm, occlusive lesion 2. Doppler signal: flow indicate stenosis

47
Duplex scan of SFA stenosis

48
Contrast arteriography
Injection contrast agent make lumen visible Conventional angiogram: direct intraarterial route Now we have digital subtraction angiogram(DSA) CT angiogram: need of arterial puncture From the picture, what is the diagnosis?
 CT angiogram: need of arterial puncture. From the picture, what is the diagnosis")
49
Computerised tomographic (CT) angiograhy
Helical CT scan with intra-arterial contrast injection Look the relation between artery and other structure well Carotid body tumor

50
Magnetic resonance arteriography(MRA)
without contrast or IV gadolinium Suitable in patient should not given iodine containing contrast due to renal disease or allergy

51
Aneurysm Pulsatile expansile mass Clinical feature:
invade surrounding tissue cause- pain rupture embolisation - ischaemia e.g. claudication, trash foot

52
Ruptured AAA

53
Trash foot-multiple small atheromatous debris

54
Investigation Ultrasound CT scan ??? angiogram

55
CT scan “Infrarenal AAA”

56
Angiogram of popliteal aneurysm

57
Venous disease

58
Functional anatomy Superficial venous system devided into 3 parts
Long saphenous vein (LSV) Short saphenous vein (SSV) Perforating or communicating vein (PV)
 Short saphenous vein (SSV) Perforating or communicating vein (PV)")
59
Superficial venous system
LSV: medial malleolus to groin SSV: outer border of foot behind lateral malleolus ascend to middle of the calf 60% to pop V., 20% to LSV and 20% wherelse

60
Superficial venous system
PV connnect superficial and deep vein > 50 PV in one leg PV in thigh connect directly between superficial and deep system, in leg connect indirectly via venous plexus

61
Deep venous system 3 artery below knee, there are 2 vein beside of artery from foot up to knee joint Then pop V beside artery then in thigh ->superficial femoral vein join with profunda femoris vein -> common femoral vein

62
Physiology of venous drainage
Normal: superficial to deep and from distal(foot) to proximal(thigh and heart ) ?? At standing position, blood at ankle has to return against gravity to heart over a distance of > 1 metre “how”
 to proximal(thigh and heart ) At standing position, blood at ankle has to return against gravity to heart over a distance of > 1 metre how")
63
How 4 factors support this system
Functioning vein valves: resist > 300 mmHg Functioning foot and calf muscle pumps: weight compress venous plexus in foot and calf muscle compress sinusoidal and deep vein in leg Residual arterial pressure Negative intrathoracic pressure “ however absent valve or damaged valve, the muscle pump cannot work efficiently”

64
Pathophysiology of varicose vein
Abnormal dilated and tortuous superficial vein of the leg Response to a pathological increase in the vein’s intraluminal pressure This increases due to higher intraluminal pressure of deep vein (necessary to allow movement of blood out of leg) from deep to superficial system
 from deep to superficial system.")
65
Aetiology Primary e.g. saphenofemorla valve incompetence

66
Aetiology Secondary mostly due to previous DVT Simple obstruction
Destroying the valves within deep vein These lead to blood move to superficial system (compensatory mechanism) ** a must to know this, otherwise we may worsen patient with VV surgery** Primary VV or secondary VV
 ** a must to know this, otherwise we may worsen patient with VV surgery** Primary VV or secondary VV.")
67
Clinical feature of varicose vein
Cosmetic presentation Discomfort and pain Cramps Swelling Complication - thrombophebitis - haemorrhage - CVI

68
Patients assessment in VV(1)
History: past Hx of DVT Examination: standing position Area of VV Brodie Tredelenberg test Perthes’ test Continous wave Doppler

69
VV

70
Brodie Tredelenberg test

71
Patients assessment in VV(2)
Radiological evaluation when suspected of previous DVT Duplex scan Ascending venography (inject radioopaque in foot and watching it rise in the deep vein)
")
73
Varicose eczema

74
Chronic leg ulcer

75
Neuropathic ulcer

76
Venous ulcer

77
Arterial ulcer

78
Acute non-traumatic leg pain
Localised to skin soft tissue, vein -cellulitis -lymphagitis -thrombophlebitis Pain radiate from back Exacebate by bending -lumbosacral N root compression Deep pain in whole legThigh, calf 5P Pain, uniform swelling No paresis or sensory loss Emboli source, no IC,N contralat pulse*heparin DVT, rupture of baker’s cyst +ac emboli - ac thrombosis

79
Chronic non-traumatic leg pain
Pain radiate from back Exacebate by bending -lumbosacral N root compression Pain in calf, foot Not radiate to back claudication Critical limb ischaemia Rest pain, gangrene, ulcer

80
History of swelling, DVT Confirm with duplex scan
Varicose vein History of swelling, DVT Confirm with duplex scan Secondary VV Primary VV Intervention Sx, sclerotherapy Supportive treatment

81
Ulcer Flat, sloping edge, soft edge Punch out base Shallow, edema, erythrema Infection, granulation tissue Black, dry Deep to tendon position Digit, pressure Point, heel, metartarsal head Above medial malleolus Asso DVI Digit, heel Ischaemic ulcer Sensory ulcer Venous ulcer

Similar presentations