Download presentation
Presentation is loading. Please wait.

1
Iowa Plan: Dental Public Health in Iowa
Bob Russell, DDS, MPH Iowa Department of Public Health

2
Title V MCH Service Areas

3
Partners Within each county are multiple agencies (local public and private/non-private agencies) that serve families: County health departments Public health nursing services Home health care agencies Visiting nurse services Community action programs 3

4
Assessment Examples Open Mouth Surveys Medicaid Services
Title V Databases & Reports Public Health Supervision Reports Back to the three core functions of public health… In order to assess programmatic and policy needs - We monitor oral health status and prevalence of disease several ways. One thing that we do is to work with our contractors to conduct open mouth surveys. Our funding dictates that we primarily focus on children – and specifically a National Performance Measure for the Title V block grant requires determining prevalence of sealants on 3rd graders. These surveys are conducted as often as needed – based on statistical significance of results. Survey reports are posted on the IDPH Web site. We are also beginning to conduct more surveillance on children younger than school age – between 0 and 5. Two years ago we did an open mouth survey of Head Start children. Last year we collected information on children in WIC. This year we plan to go into day care centers. We also review Medicaid data – usually utilization and billing data. By looking at the ability of Medicaid-enrolled children to access services, we can assess the ability of at-risk children and families in general. It also provides us a means to determine if our programs are making an impact. We are also able to request specific reporting from Medicaid – which helps us to look at specific issues – for example, physicians who bill for fluoride varnish applications – where they are located, how many they did. These things help us to determine program needs and potential policy changes needed. Another means of assessment includes reviewing information from databases for our MCH Contractors – which track demographics, services provided (as well as barriers and needs) of CH and MH clients. We also receive annual reports from dental hygienists practicing under public health supervision – which provides a glimpse at the number of services and population who receive care via public health settings. There are other things we can use – such as the Behavioral Risk Factor Surveillance – BRFSS – and Iowa’s House hold Health survey. Our assessment function does not include RESEARCH – which is something more applicable to the University.
 of CH and MH clients. We also receive annual reports from dental hygienists practicing under public health supervision – which provides a glimpse at the number of services and population who receive care via public health settings. There are other things we can use – such as the Behavioral Risk Factor Surveillance – BRFSS – and Iowa’s House hold Health survey. Our assessment function does not include RESEARCH – which is something more applicable to the University.")
5
National Trends in Caries-Free Schoolchildren – Permanent Teeth
Fluoridation and Public Health 2011 Training Program National Trends in Caries-Free Schoolchildren – Permanent Teeth Ages 5-17 years Ages 6-19 years Similarly, the percentage of caries free children has been increasing.

6
Iowa: Untreated decay is decreasing

7
Iowa: Adults

8
Penetration of Public Health Sealant Programs in Iowa
79 elementary schools Total: 990 elementary schools 21 Junior High Schools Total: 299 Junior High Schools 9,941 Sealant placed on 1st molars in 2,381 sealants placed on second molar teeth

9
Decay Positive and Decay Negative
We subset the dataset into two datasets: decay positive and decay negative. The graph demonstrates how the treatment rate differed between decay and no decay treatment groups. This shows that there is a possibility that the screenings do play some role in children seeking treatment. Decay Positive and Decay Negative

10
Results Decay Positive Decay Negative 29.9% from East Central Iowa
29.1% Rural (Not adjacent to urban) 66.7% white, 16% unknown race/ethnicity 80.5% spoke English 92.2% had a Medical Home 69.3% had a Dental Home 52.7% Males 56.8% were younger than 5 37.8% from East Central Iowa 22.2% Rural (Not adjacent to urban) 70.5% white, 16% unknown race/ethnicity 85.2% spoke English 95.5% had a Medical Home 61.2% had a Dental Home 49.9% Males 73.5% were younger than 5 We used logistic regression analysis to find associations between variables and outcome of not receiving treatment. In CAReS, Medical and Dental Home are both determined for a child, based on responses to specific information from the parent or guardian. So, as you see on this slide, for the purposes of determining medical and dental home in CAReS: Medical home: child has a usual source of medical care, the care is available 24/7, and the source of the care maintains the child’s record Dental home: the child has a usual source of dental care, that source of care maintains the child’s record, and the child has seen a dentist within the past 12 months
 66.7% white, 16% unknown race/ethnicity. 80.5% spoke English. 92.2% had a Medical Home. 69.3% had a Dental Home. 52.7% Males. 56.8% were younger than % from East Central Iowa. 22.2% Rural (Not adjacent to urban) 70.5% white, 16% unknown race/ethnicity. 85.2% spoke English. 95.5% had a Medical Home. 61.2% had a Dental Home. 49.9% Males. 73.5% were younger than 5. We used logistic regression analysis to find associations between variables and outcome of not receiving treatment. In CAReS, Medical and Dental Home are both determined for a child, based on responses to specific information from the parent or guardian. So, as you see on this slide, for the purposes of determining medical and dental home in CAReS: Medical home: child has a usual source of medical care, the care is available 24/7, and the source of the care maintains the child’s record. Dental home: the child has a usual source of dental care, that source of care maintains the child’s record, and the child has seen a dentist within the past 12 months.")
12
Iowa: a State in Transition
Demographic Trends Rapid Ethnic Diversification Aging white population Low fertility rates among whites Exodus of graduates to other states Higher birth rates among native minorities Large influx of immigrants, primarily Latinos, to work in labor shortage

13
Iowa Implications of Changing Demographics
Need for increased outreach services Need for new service hours Child Care barriers Geographic and transportation barriers Different health care utilization patterns

15
Iowa Elderly in Assisted Living Centers
2007 Survey Results

16
The Iowa Picture We have stated that 92% of Iowans are receiving optimally fluoridated water. What does this % really mean? 92% of Iowans who receive their water from a Community Water Supply are receiving optimally fluoridated water. Overall, approximately 83% of Iowa’s total population is receiving optimally fluoridated water. This percentage may actually be higher depending on if the population who receives their water by a private well has naturally fluoridated water or is adding fluoride to their water. We have no system for tracking private wells or monitoring leaving over 248,205 estimated Iowans potentially lacking fluoridated water!

17
Trends are Troublesome
No longer provides fluoride Water System County Ashton Osceola County Columbus Junction Louisa County Coon Rapids Carroll County Elkader Clayton County Everly Clay County Floyd Floyd County Fort Madison Lee County Granger Dallas County Maxwell Story County Sac City Sac County Sanborn O’Brien County Sutherland Victor Iowa County

18
Considering discontinuation or reduction
Iowa Considering discontinuation or reduction Water System County Aplington Butler County Cedar Rapids Linn County Dallas Center Dallas County DeSoto Gilmore City Humboldt County Granger Keokuk Lee County Mechanicsville Cedar County New Sharon Mahaska County Ossian Winneshiek County Tama Tama County

19
I-Smile An Overview of Iowa’s Dental Home Initiative for Children
Bob Russell, DDS, MPH State Public Health Dental Director Iowa Department of Public Health

20
2005 Legislative Mandate By July 1, 2008, every recipient of medical assistance who is a child 12 years of age or younger shall have a designated dental home and shall be provided with the dental screenings and preventive care identified in the oral health standards under the EPSDT program. In response, the Iowa DHS partnered with the IDPH, the IDA, the IDHA, the University of Iowa, and others to develop a proposal that would fulfill the dental home mandate. The result is the I-Smile dental home project.

21
Iowa Legislative Mandate Modified
By December 31, 2010, every recipient of medical assistance who is a child 12 years of age or younger shall have a designated dental home and shall be provided with the dental screenings and preventive services, diagnostic services, treatment services, and emergency services as defined under the EPSDT program. 2010 has come and gone, but the mandate is still in effect. * Language modified in 2008, HF2539 21

22
Conceptual Dental Home
The dental home is a system that allows all children, even those often excluded from receiving dental care, to have early and regular care to ensure optimal oral health.

23
The I-Smile Dental Home
DENTIST NURSE PHYSICIAN DENTAL HYGIENIST What makes I-Smile unique is the way that we envision the dental home. The I-Smile dental home is not a dental office. It is envisioned as a conceptual dental home. Uses a team approach to manage oral disease Primary prevention and care coordination are a large focus Dentists provide treatment and definitive diagnosis Other health care professionals are part of a larger network – providing oral screenings, education, anticipatory guidance, and preventive services as needed 23

24
I-Smile Objectives Improve the dental support system for families.
Improve the dental Medicaid program. Implement recruitment and retention strategies for underserved areas. Integrate dental services into rural and critical access hospitals. The original plan for implementing I-Smile identified 4 objectives. The first objective, improving the support system for families, is the one with the most impact on our existing public health system – specifically the state’s Maternal and Child Health system – and is the one that I will focus on.

25
I-Smile Strategies Partnerships and planning
Link with local board of health Provide training for child health agency staff Develop agency oral health protocols Provide education and training for health care professionals Ensure completion of screenings and risk assessment Ensure care coordination services Ensure provision of gap-filling preventive services Each contractor must submit an action plan and budget, developing activities based on these strategies as well as based on their local needs and assets.

26
Improve Dental Support System for Families
Strengthen Iowa’s Title V MCH System Establish a dental hygienist within each Title V Child Health agency as the local I-Smile Oral Health Coordinator Currently, Iowa has 24 dental hygienists working as regional I-Smile™ Coordinators They create a system to assure optimal oral health for children. Work on this objective occurs through our state’s Title V Maternal and Child Health system. The Dept of Public Health has 22contractors – private/non-profit or public agencies – to implement the Title V child health program at the local level. Contractors are responsible for assuring health services for pregnant women and children. For several years, the Department of Public Health and the Department of Human Services have had an interagency agreement. The agreement allows IDPH to assist in achieving EPSDT standards through these contractors – and also allows the contractors to bill Medicaid for limited services provided to Medicaid-enrolled clients. This has also been the means for funding Iowa’s ABCD program. Using lessons learned from our ABCD program, we were able to develop I-Smile strategies to be implemented through our local MCH contractors – now also funded through the interagency agreement.

27
I-Smile Referral System

28
Medicaid, uninsured, and underinsured children from birth-12 years
I-Smile Dental Home Care Plan Diagram I-Smile Oral Health Coordinator Oral Screening and Risk Assessment Preventive Care Education Medicaid, uninsured, and underinsured children from birth-12 years Level Level Level 3 Low Risk No observable disease Moderate Risk No observable disease High Risk Observable disease High Risk Severe disease P L A N Care coordination Referral for dental exam within 1 year Oral screening, risk assessment, and preventive care in 6 months Referral for dental exam within 6 months Oral screening, risk assessment, and preventive care in 3-6 months Referral for dental exam within 3 months Oral screening, risk assessment, and preventive care in 3-6 months Care coordination Immediate referral to dentist/specialist Oral screening, risk assessment, and preventive care in 3 months

32
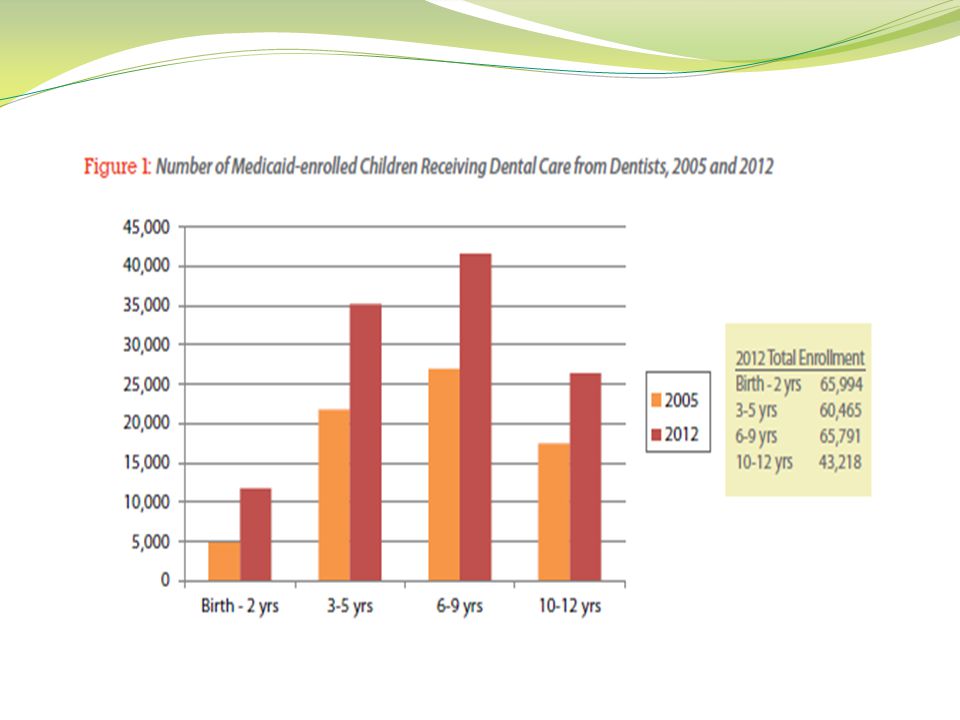
Based on SFY2012 Medicaid paid claims, Iowa Department of Human Services
In 2012: More than 1 ½ times as many children ages 0-12 saw a dentist for care than in 2005 3 ¾ times as many children ages 0-12 received care from a hygienist or nurse working for a Title V agency than in 61 % of children ages 3-12 saw a dentist

33
I-Smile--Challenges Still too many children under the age of 3 who do not receive dental services. Lack in dentists willing to see the very young child. Low participation by dentists willing to see Medicaid children. Low Medicaid reimbursement. Decreasing and aging dental workforce Mal-distribution of available dental providers Iowa Facts: Decreasing and aging dental workforce Increasing number of health professional shortage sites Mal-distribution of available dental providers Along with low reimbursement rates, the other barriers to treatment for our children include a shortage of dentists. Dentists in Iowa are aging, the average age is 55, with retirements and fewer dentists staying in Iowa after graduation from dental school the numbers are project to decline. Of the dental workforce only 2% are pediatric dentists and they are located in the major metropolitan areas. General dentists are reluctant to see children, especially those under age 3. All of this background just goes to show you how important your role is when it comes to educating parents and reducing the risk of dental problems among our low income population. Poor kids are more likely to have dental problems therefore education and preventive services are their best defense against future problems!!

34
I-Smile--Sustainability
Promote children’s oral health to parent’s and caregivers. Support gap-filling preventive services within public health and Title V agencies. Maintain partnerships with early childhood programs. Share information with stakeholders in anticipation of a changing health care system within Iowa. Continue to support “health homes” by collaborating with medical providers to include oral health as part of well-child care. Explore funding and collaborative opportunities with private organizations so that oral health becomes a priority statewide. Because children see their physician more during the years before age 3 and dentists are still reluctant to see young children physicians are being trained to do a more thorough oral evaluation during the well child exams. Medicaid is also paying for fluoride varnish application in the physicians office. I-Smile Screening Guide Basic Oral Health Screening Instructions I-Smile Coordinator Office “Lunch and Learn” sessions Web-based training with CMEs Peer-to-Peer study groups

35
I-Smile™ Future Good oral health for all children beginning at birth
Long-term savings in dental care costs Improved overall health of Iowa children and adults

36
Dental Screening Requirement
(became effective July 1, 2008) A critical step in “closing the gap” in access to care for underserved children Since 2008, Iowa children newly enrolling in elementary and high school must provide evidence of having a dental screening or exam.
 A critical step in closing the gap in access to care for underserved children. Since 2008, Iowa children newly enrolling in elementary and high school must provide evidence of having a dental screening or exam.")
37
Dental Screening Requirements
Elementary school Prior to age 6, but no earlier than age 3 Licensed physician, physician assistant, nurse, dental hygienist, dentist High School: Within one year of enrollment Licensed dental hygienist or dentist

38
Integration with I-Smile™
What if a child has a problem getting a screening? What if a problem is detected and a child doesn’t have a dentist? Contact local I-Smile Coordinator

39
Supervision Dental hygienist providing direct care services in Iowa must work under the supervision of a dentist. In public health settings, this would be either public health or general supervision.

40
Public Health Supervision
Recommended by IDPH, this allows hygienists working in a public health setting to provide services without the patient first being examined by a dentist. *Dentists providing public health supervision are not required to provide future dental treatment to patients served by the hygienist.

41
Some services required to maintain Public Health Status:
Requirements for Practice as a Public Health Supervision Hygienist (PHSH) Educational & Experiential Requirements An Active Iowa license and a Minimum of 3 years clinical experience No special educational requirements Must collect data on services provided Must have procedure for maintaining records Practice Settings Available to a PHSH Schools Head Start FQHCs Public Health Dental Vans CHCs Nursing facilities Free Clinics State/local federal public health programs Day Care Centers Services a PHSH can Provide Assessments Screenings Data collection Educational, diagnostic, preventive and therapeutic services defined in the rules May NOT provide local anesthesia or nitrous oxide. Requirements Settings Services Some services required to maintain Public Health Status:
 Educational & Experiential Requirements. An Active Iowa license and a. Minimum of 3 years clinical experience. No special educational requirements. Must collect data on services provided. Must have procedure for maintaining records. Practice Settings Available to a PHSH. Schools. Head Start. FQHCs. Public Health Dental Vans. CHCs. Nursing facilities. Free Clinics. State/local federal public health programs. Day Care Centers. Services a PHSH can Provide. Assessments. Screenings. Data collection. Educational, diagnostic, preventive and therapeutic services defined in the rules. May NOT provide local anesthesia or nitrous oxide. Requirements. Settings. Services. Some services required to maintain Public Health Status:")
42
Statutes & Rules Applicable Forms
Practice as Public Health Supervision Hygienist– What Else Do I Need to Know? Statutes & Rules Applicable Forms State Dental Practice Act Iowa Code 153 Iowa Code 147 Iowa Code 272C Dental Board Rules Public Health Supervision (PHS Application) PHS Reporting Form Iowa Dental Board
 PHS Reporting Form. Iowa Dental Board.")
43
General Supervision A dentist is required to see a patient prior to a dental hygienist providing certain services under general supervision Sealants Prophylaxis Radiographs

44
Public Health Supervision
Currently, a hygienist must have an Iowa license and a minimum of three years of clinical experience to work under public health supervision. *Language removed April For certain services (ie: prophy’s, sealants, and radiographs), there is no longer a period of time, no more than 12 months, in which an exam by a dentist must occur prior to providing this service to a patient again.
, there is no longer a period of time, no more than 12 months, in which an exam by a dentist must occur prior to providing this service to a patient again.")
45
Loan Repayment Two options:
National Health Service Corps – federal program State Loan Repayment Program (called PRIMECARRE) Site criteria: For PRIMECARRE, must be public or non-profit; NHSC also allows for-profit Federal Health Professional Shortage Area (found at Sliding fee scale, accept Medicaid and Medicare
 Site criteria: For PRIMECARRE, must be public or non-profit; NHSC also allows for-profit. Federal Health Professional Shortage Area (found at Sliding fee scale, accept Medicaid and Medicare.")
46
Applicant Eligibility
Full-time or half-time (meet definition) U.S. citizen Education-related debts No unfulfilled practice obligation to federal, state, local government or other entity (such as employer) Certification or license to practice in Iowa Serve all patients regardless of ability to pay Full time = 40 hours Half time = 20 hours Cannot do both loan repayment programs at the same time (but can do them back to back) Cannot have any other contractual obligation at the same time (employer contract)
 U.S. citizen. Education-related debts. No unfulfilled practice obligation to federal, state, local government or other entity (such as employer) Certification or license to practice in Iowa. Serve all patients regardless of ability to pay. Full time = 40 hours. Half time = 20 hours. Cannot do both loan repayment programs at the same time (but can do them back to back) Cannot have any other contractual obligation at the same time (employer contract)")
47
Eligible Professions Primary care physician Dentist Dental Hygienist
Physician Assistant Nurse Practitioner Certified nurse Midwife Clinical Psychologist Clinical Social Worker (LISW only) Psychiatric nurse specialist Mental Health Counselor Marriage and Family Therapist For health care providers providing DIRECT CARE!!! Private practice dentists would not qualify (they are not public/non-profit). For RDH’s they would have to work for an FQHC or other type of public health dental clinic.
 Psychiatric nurse specialist. Mental Health Counselor. Marriage and Family Therapist. For health care providers providing DIRECT CARE!!! Private practice dentists would not qualify (they are not public/non-profit). For RDH’s they would have to work for an FQHC or other type of public health dental clinic.")
48
Both Programs: Clinician must be: working in a federally designated HPSA, US citizen, qualified student loan debt, cannot be fulfilling another obligation at the same time NHSC PRIMECARRE Online application, Application cycle once per year available on IDPH website, Current due date: October 24, 2012 Federally Administered State Administered All Federal Funds 1:1 State/Federal Funds Requires Site Application Does not require site application Full time 2-year contract $60,000 Half time 2-year contract $30,000 Half time 4-year contract $60,000 Full time 2-year contract up to $100,000 or Half time 2 –year contract up to $50,000 (depending on availability of funding and number of applicants) Competitive Process based on HPSA scores Competitive Process with review committee Can be For-Profit, Non-Profit, or Public Sites Only Public or Non-Profit Site Entire amount of funding provided to clinician at beginning of 2-year contract with NHSC Half of funding provided at the beginning of each year of the 2-year contract; funds go directly to lender One-year continuations Can re-apply in two-year increments Comparison of the two programs: Applicants must be licensed by January 1 (date the contract starts) 14 typically apply 5-8 typically awarded
 Competitive Process based on HPSA scores. Competitive Process with review committee. Can be For-Profit, Non-Profit, or Public Sites. Only Public or Non-Profit Site. Entire amount of funding provided to clinician at beginning of 2-year contract with NHSC. Half of funding provided at the beginning of each year of the 2-year contract; funds go directly to lender. One-year continuations. Can re-apply in two-year increments. Comparison of the two programs: Applicants must be licensed by January 1 (date the contract starts) 14 typically apply. 5-8 typically awarded.")
49
Thank you! Iowa Department of Public Health Oral Health Center
Dr. Bob Russell, DDS, MPH Public Health Dental Director (515) Iowa Department of Public Health Oral Health Center Lucas State Office Building 321 East 12th Street Des Moines, Iowa 50319
 Iowa Department of Public Health. Oral Health Center. Lucas State Office Building. 321 East 12th Street. Des Moines, Iowa")
50
References Institute of Medicine, National Academy of Sciences. The Future of Public Health. Washington DC; National Academy Press; 1988. Public Health Functions Steering Committee. Public Health in America. Washington, DC: PHS; 1995. CDC. Ten Great Public Health Achievements - United States, MMWR. 1999;48(12);
;")
Similar presentations




 The National Health Service Corps and Other Federal Scholarship and Loan Repayment Opportunities for.>")






 Federal Scholarship and Loan Repayment Opportunities for Health Professionals W. Gary Hlady, MD, MS.>")






 Presentation to 3rd International Conference.>")


 County Health Department.>")