Download presentation
Presentation is loading. Please wait.

1
Hemodialysis adequacy & Outcome: from NCDS to HEMO & MPO
Saeed M.G Al-GHAMDI, FRCPC, FACP King Faisal Specialist Hospital & Research Center-Jeddah

2
Beginning of Hemodialysis

3
National Cooperative Dialysis Study
NCDS Lowrie eg; Laird NM, PARKER TF; SARGENT JA New England journal of medicine November 12;305(20):
:")
4
Lowerie EG, et al, N Engl J Med 1981, Nov, 12; 305(20): 1176-81
Effect of hemodialysis prescription of patients morbidity: Report of NCDS 151 patients 4 treatment groups Long dialysis Short dialysis High time-average urea concentration Low time-average urea concentration Protein intake was not restricted Lowerie EG, et al, N Engl J Med 1981, Nov, 12; 305(20):
:")
5
Lowerie EG, et al, N Engl J Med 1981, Nov, 12; 305(20): 1176-81
NCDS: Results No difference in mortality between groups Withdrawal was higher in the high urea group Hospitalization was higher in higher urea group Morbidity was higher in the high ATC-urea Morbidity may be decreased by prescription associated with more efficient removal of urea if adequate protein intake Lowerie EG, et al, N Engl J Med 1981, Nov, 12; 305(20):
:")
6
Mechanistic analysis of NCDS
Gotch used NCDS data and introduced kt/v of urea Efficiency of urea removal (small toxins) Dietary protein intake Kt/v is an important measure of clinical outcome Gotch, FA, Sargent,JA KI 1985; 28:
 Dietary protein intake. Kt/v is an important measure of clinical outcome. Gotch, FA, Sargent,JA KI 1985; 28:")
7
Kt/v: Single pool Vs double pool
Urea is equilibrated between muscles and plasma water Single pool kt/v (non- equilibrated): blood urea is measured at end of dialysis from circuit Double pool kt/v (equilibrated): venous sample post dialysis (30 minutes) Single pool kt/v is 0.20 higher than double pool
: blood urea is measured at end of dialysis from circuit. Double pool kt/v (equilibrated): venous sample post dialysis (30 minutes) Single pool kt/v is 0.20 higher than double pool.")
8
Kt/v: Practice & Recommendations
Slow the pump to 100 ml/minute Obtain urea sample 15 seconds later Target kt/v of 1.2 (URR of 65%) The mean delivered sp-kt/v in USA: 1.5, more than 90% above 1.2 The mean kt/v in Europe: KDOQI , AJKD 2006, EBPG, NDT 2002 USRDS 2007, EBPG, DOPPS 2004
 The mean delivered sp-kt/v in USA: 1.5, more than 90% above 1.2. The mean kt/v in Europe: KDOQI , AJKD 2006, EBPG, NDT USRDS 2007, EBPG, DOPPS")
9
Optimal Dialysis dose Is the summation of clinical and biochemical parameters which refer to the adequately delivered dose of dialysis , in which patient has no symptoms which could be attributed to under-dialysis and more importantly, to a measurable value at which the dialysis patient has the lowest morbidly and mortality

10
High kt/v: Positive observational studies
Survival in long-term hemodialysis patients: results from the annual survey of the Japanese society of dialysis therapy. Shinazato et al, NDT 1997; 12:884-8 Body size, dose of hemodialysis and mortality. Wolfe RA et al, AJKD 2000; 35: 80-88 Dialysis dose and body mass index are strongly associated with survival in hemodialysis patients. Port FK, et al, JASN 2002; 13:

11
High kt/v: negative observational study
The dose of hemodialysis and patient mortality. Held PJ et al, KI 1996; 50:550-6

12
Eknoyan G et al New Engl J Medicine 2002; 347: 2010
Effect of Dialysis Dose and Membrane Flux in Maintenance Hemodialysis HEMO study Eknoyan G et al New Engl J Medicine 2002; 347: 2010

13
HEMO study: Design 1846 prevalent patients in 72 dialysis units in USA
RCT: mean follow up of 2.8 year Two-by-two factorial design Standard dose: sp- kt/v 1.25 or URR 65% High dose: sp-kt/v 1.65 or URR of 75% Low-flux High-flux

14
HEMO study: Outcomes Primary outcome: Secondary outcome:
Death from any cause Secondary outcome: Rate of hospitalizations (excluding access) Composite outcome First hospitalization from cardiac cause or death from any cause (ACM) First hospitalization from infectious cause or death First decline of 15% in serum albumin from baseline value or death
 Composite outcome. First hospitalization from cardiac cause or death from any cause (ACM) First hospitalization from infectious cause or death. First decline of 15% in serum albumin from baseline value or death.")
15
HEMO Study Eknoyan G et al New Engl J Medicine 2002; 347: 2010

16
HEMO Study Eknoyan G et al New Engl J Medicine 2002; 347: 2010

17
HEMO Study : Primary outcome Eknoyan G et al New Engl J Medicine 2002; 347: 2010

18
HEMO Study Eknoyan G et al New Engl J Medicine 2002; 347: 2010

19
HEMO Study : Primary outcome Eknoyan G et al New Engl J Medicine 2002; 347: 2010

20
HEMO Study : Secondary outcome Eknoyan G et al New Engl J Medicine 2002; 347: 2010

21
HEMO conclusion: Primary outcome
Neither the difference between the two dose groups nor the difference between flux groups were significant After adjustment of base-line factors High dose group: risk of death 4% lower P= 0.53 High-flux group: risk of death 8% lower P= 0.23

22
HEMO conclusion: Secondary outcomes
The risk of main secondary outcome was the same for both dialysis dose groups and for both flux groups.

23
HEMO study: Conclusion
Among patients undergoing maintenance hemodialysis who were receiving thrice-weekly treatment lasting hours each, neither a higher dose nor the use of high-flux membranes significantly improved survival or reduced morbidity This support the current guidelines of single-pool kt/v of , and make no recommendation for or against routine use of high-flux membranes

24
HEMO study: Subgroup analysis
In high-flux there is significant reduction in RR of death (20%) from cardiac causes and combined outcome of first hospitalization or death from cardiac cause Longer dialysis duration High-flux dialysis for > 3.7 year has 32% lower risk of death when compared with low-flux Cheung A, et al , JASN 2003; 14:
 from cardiac causes and combined outcome of first hospitalization or death from cardiac cause. Longer dialysis duration. High-flux dialysis for > 3.7 year has 32% lower risk of death when compared with low-flux. Cheung A, et al , JASN 2003; 14:")
25
HEMO Study: Subgroup analysis
Sex and dialysis dose Women with high dose has 19% lower risk of death Men with high dose has 16% higher risk of death Beta-2-microglobulin: serum level correlated with mortality particularly from infectious causes

26
Effect of Membrane Permeability on Survival of Hemodialysis Patients (MPO Study)
Locatelli F, Martin-Malo A, Hannedouche T, Loureiro A, Papadimitriou M, Wizemann V, Jacobson SH, Czekalski S, Ronco C, Vanholder R, JASN 2009; 20:

27
MPO: Hypothesis Mortality in dialysis patients 24% in USA and 14-26% in Europe Retention of high MW molecules may be implicated in the high mortality High-flux membranes can remove those molecules Epidemiologic data suggested benefits Only one underpowered RCT which did not show benefit

28
MPO Study: Design RCT: 59 European study centers
738 incident hemodialysis patients Follow up from years (mean 3 year) Patients were randomized to receive high or low-flux membrane according to Low albumin <4 g/dl (567 patients) Normal albumin > 4 g/dl (171 patients) Minimal single-pool kt/v of 1.2
 Patients were randomized to receive high or low-flux membrane according to. Low albumin <4 g/dl (567 patients) Normal albumin > 4 g/dl (171 patients) Minimal single-pool kt/v of 1.2.")
29
MPO study; Methodology Locatelli, F. et al
MPO study; Methodology Locatelli, F. et al. J Am Soc Nephrol 2009;20:

30
MPO study: Results: Kaplan-Meier survival curves for the complete intention-to-treat population (Log-rank test P = 0.214) Locatelli, F. et al. J Am Soc Nephrol 2009;20: Locatelli, F. et al. J Am Soc Nephrol 2009;20:

31
MPO study : Results Kaplan-Meier survival curves for the population of patients with serum albumin <=4 g/dl (Log-rank test P = 0.032

32
MPO study : Results Kaplan-Meier survival curves for the subpopulation of patients with diabetes (Log-rank test P = 0.039) Locatelli, F. et al. J Am Soc Nephrol 2009;20:

33
MPO study: Results Locatelli, F. et al
MPO study: Results Locatelli, F. et al. J Am Soc Nephrol 2009;20:

34
MPO: Conclusions No significant effect of permeability on survival was found in the population as a whole High-flux showed significant survival benefit in high risk population (RR reduction of 37%) High-flux showed significant survival benefit in diabetics (adjusted risk reduction of 38%)
 High-flux showed significant survival benefit in diabetics (adjusted risk reduction of 38%)")
35
HEMO & MPO: Differences
Europe Membrane flux in high risk groups USA Dialysis dose Membrane flux RCT Incident patients Mostly Prevalent patients Enrollment yes no Risk stratification 3-7 year (3 y) 2.8 years Duration
 2.8 years. Duration.")
37
How can we decrease morbidity and mortality in HD patients?

38
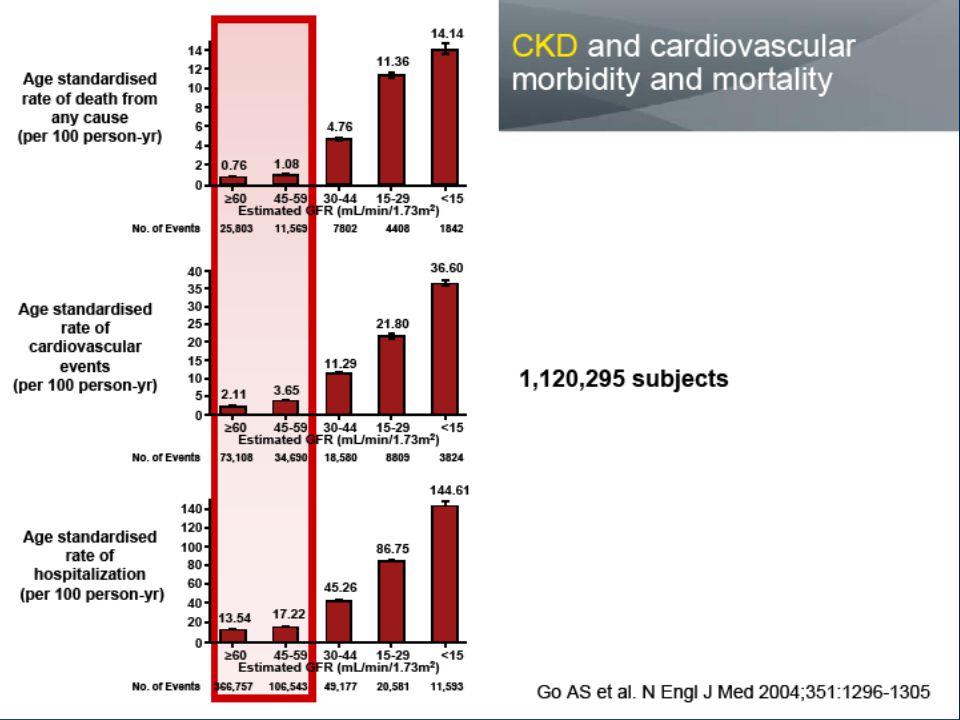
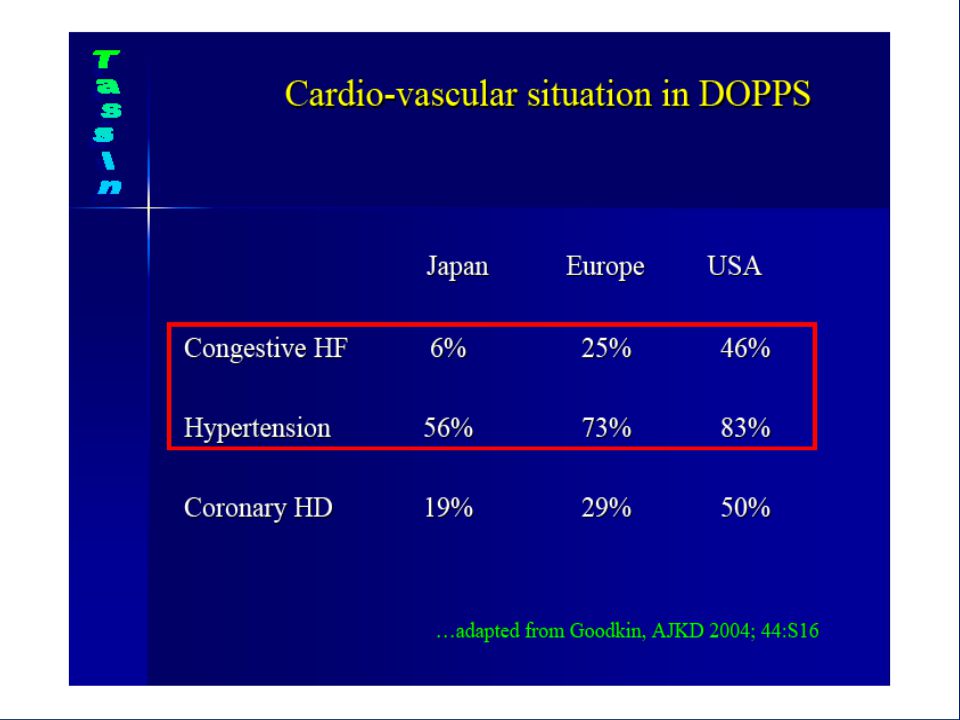
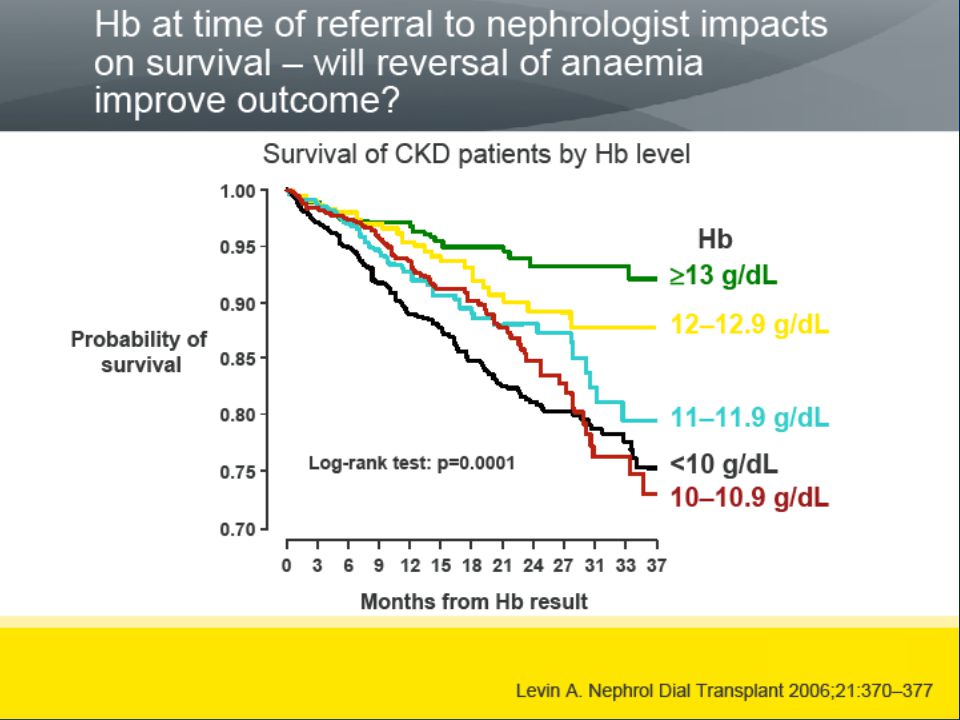
How can we reduce morbidity and mortality in HD patients?
Attention to traditional and non-traditional risk factors Anemia Hypertension CKD-MBD Individualization of dialysis therapy High flux for high risk group or non-transplant patients High dose kt/v for women

39
Future attempt to lower M&M
More refinement of our dialysis prescription Treatment Time Daily dialysis or Quotidian

40
Survival on dialysis according to country and DM
Hull, AR, Parker, TF III, Am J Kidney Dis 1990; 15:375, and Charra, B, Calemard, E, Ruffet, M, et al, Kidney Int 1992; 41:1286.

48
Conclusions Targeting high kt/v has no significant impact on mortality, and the current kt/v >1.2 is still holding High-flux membrane might be of benefit in high risk group and in chronic HD patients Longer treatment time of dialysis probably is more important than kt/v CKD-MBD has major impact on morbidity and mortality

49
Conclusion The focus to reduce morbidity and mortality may be directed to lowering traditional and non-traditional risk factors in dialysis population

50
Thank You

Similar presentations










 Source Jaber BL, Schiller B, Burkart JM, et al.>")
 Decreased muscle mass Increased incidence of morbidity and.>")

![Chronic kidney disease: [insert title here] Insert name, title, date here Insert acknowledgements here.](/12/3497998/big_thumb.jpg "Chronic kidney disease: [insert title here] Insert name, title, date here Insert acknowledgements here.>")



.>")

>")



 Kingsbrook Jewish Medical Center Clinical Instructor of Pharmacy Practice.>")
