Download presentation
Presentation is loading. Please wait.

1
Deep Hypothermic Circulatory Arrest in Pediatric Cardiac Surgery 2009
Nabila Fahmy, MD Professor of Anesthesiology Ain Shams University

2
Cessation of the blood circulation for some time during surgery of the arch and repair of congenital heart defects is normally required to allow a bloodless operation field.. Hypothermia is the most important mechanism for end-organ protection, particularly the brain, during such operations. Cardiopulmonary bypass is used for core cooling before deep hypothermic circulatory arrest (DHCA) is initiated .
 is initiated .")
3
WHAT IS DHCA?

4
DEEP HYPOTHERMIC CIRCULATORY ARREST (DHCA)
Mild hypothermia – 30 C to 34 C Moderate hypothermia – 25 C to 30 C Deep hypothermia – 15 C to 22 C Circulatory arrest – no flow in the blood vessels DHCA – no blood flow during deep hypothermia

5
HOW DO WE DO DHCA?

6
TECHNIQUE OF DHCA Usually planned
Most protocols involving DHCA involve the following : Administration of barbiturates, usually thiopental for the reduction of cerebral metabolism. Mannitol to help reduce potential increased intracranial pressure and to reduce free radicals. Steroids to promote cell membrane integrity and reduce brain swelling. Cooling is started before CPB by simply cooling the operating room and with ice packing to the head After systemic heparinization and cannulation are performed, CPB is started and cooling is begins for at least minutes. The patient's body temperature is monitored by means of esophageal, tympanic, and rectal routes. After adequate cooling is achieved, the circulation is arrested to allow the surgeon to perform the critical part of the reconstruction. The duration of DHCA is limited to the shortest time possible. After circulation is restarted, the rest of the repair is performed during the rewarming phase. The anesthetic and surgical plan involves mutual goals of tissue and organ protection by decreasing cellular metabolism and substrate delivery during the absence of perfusion.

7
WHY DHCA?

8
ADVANTAGES OF DHCA Bloodless operating field with improved exposure
Decreased exposure to cardiopulmonary bypass with its sequelae (such as activation of white cells and endothelium, activation of cascades, consumption of coagulation factors and platelets, hemolysis, etc.) Diminished risk of embolism (solids and gases) No cannulas in the operating field Less distortion of heart - cannulas are not in place DHCA offers brain protection for a period of about minutes. Reduced CMRO2 to be approximately 10%-15% of its normothermic base line. Lower plasma activated complement (C3a), interleukin 8, interleukin 6 (when compared with low-flow CPB) Bellinger DC, et al. N Engl J med. 1995;332:
 Diminished risk of embolism (solids and gases) No cannulas in the operating field. Less distortion of heart - cannulas are not in place. DHCA offers brain protection for a period of about minutes. Reduced CMRO2 to be approximately 10%-15% of its normothermic base line. Lower plasma activated complement (C3a), interleukin 8, interleukin 6 (when compared with low-flow CPB) Bellinger DC, et al. N Engl J med. 1995;332:")
9
The duration of DHCA is limited to the shortest time possible as (landmark boston circulatory arrest study, march 2007) 3-5 mins of cerebral ischemia can be tolerated at 37 c. 15 mins c. 41 mins c.

11
CEREBRAL PHYSIOLOGY DURING
CARDIAC SURGERY CLINICAL STUDIES (Greeley, Kern, Ungerdeider) HAVE BEEN UNDERTAKEN IN THE LATE 1980s TRHOUGH MID 1990s TO UNDERSTAND NEUROPHYSIOLOGY IN INFANTS AND CHILDREN DURING CARDIAC SURGERY INVOLVING CPB AND DHCA CNS HAS A HIGH METABOLIC NOTE & LIMITED ENERGY STORES CNS IS THE MOST SENSITIVE ORGAN TO ISCHEMIA ATTENTION HAS BEEN CENTERED ON NEUROLOGIC OUTCOME WHEN PERFUSION IS REDUCED, LEADING TO NEUROLOGIC COMPLICATIONS IN THE POSTOPERATIVE PERIOD.
 HAVE BEEN UNDERTAKEN IN THE LATE 1980s. TRHOUGH MID 1990s TO UNDERSTAND. NEUROPHYSIOLOGY IN INFANTS AND CHILDREN. DURING CARDIAC SURGERY INVOLVING CPB. AND DHCA. CNS HAS A HIGH METABOLIC NOTE & LIMITED ENERGY STORES. CNS IS THE MOST SENSITIVE ORGAN TO ISCHEMIA. ATTENTION HAS BEEN CENTERED ON NEUROLOGIC OUTCOME WHEN PERFUSION IS REDUCED, LEADING TO NEUROLOGIC COMPLICATIONS IN THE POSTOPERATIVE PERIOD.")
12
THE REPORTED INCIDENCE OF NEUROLOGICAL COMPLICATIONS
AFTER PEDIATRIC CARDIAC SURGERY RANGES FROM 2% TO 25% Austin EH III,Edmonds HI,Auden SM et al. Benefit of neurophysiological monitoring for pediatric Cardiac surgery.J Thorac Cardiovasc Surg 1997;114 :707-15 Menache CC,du Plessis AJ,Wessel DL et al. Current incidence of acute neurologic complications After open heart operation in children Ann Thorac Surg 2002; 73:1752.8

13
Neurologic morbidity include
seizures stroke changed tone and mental status motor disorders - time to recovery of EEG activity . Abnormal cognitive function Post Pump choreoatherosis paraplegia Areas most vulnerable to ischemic Injury : Neocortex Hippocompus Striatum

14
mechanism of brain injury involves binding of glutamate to NMDA receptor , increasing the intracellular ca++ and subsequently activates proteases phospholipases and deoxyribonucleases , promotes the generation of free radicals cell injury , cell death . Hypothermia the release of glutamate During DHCA , microemboli can be detected .

15
THE ETIOLOGY OF NEUROLOGICAL
DYSFUNCTION IN CHILDREN IS FOR THE MOST PART ISCHEMIA PATHOPHYSIOLOGIC MECHANISMS ACCOUNTING FOR NEUROLOGIC INJURY INCLUDE: rate and extent of cooling and rewarming management of CPB prolonged DHCA anemia low cardiac output

16
16

17
17

18
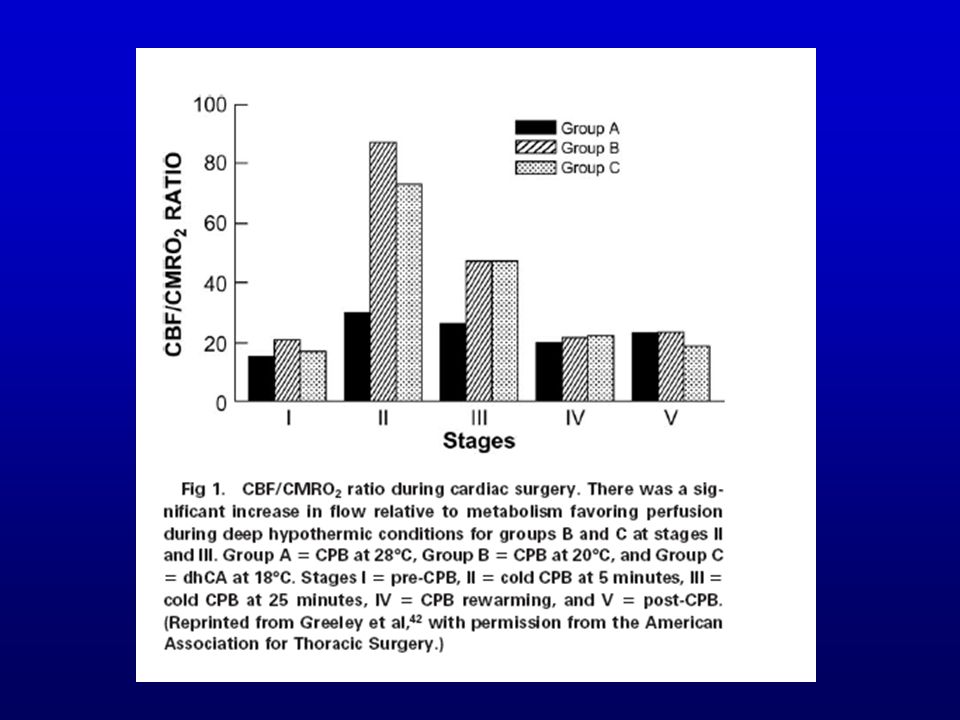
UNDER DEEP HYPOTHERMIC CPB CBF IS REDUCED BUT THERE IS AN
EXPONENTIALLY GREATER REDUCTION IN CMRO2. A STATE OF LUXURY PERFUSION EXISTS WITH AN EXCESS OF FLOW RELATIVE TO OXYGEN CONSUMPTION; 1:75 (conferring cerebral protection) IN PATIENTS UNDERGOING DHCA CBF AND CMRO2 REMAIN DECREASED AFTER REWARMING AND WEANING FROM CPB Sara Lozano, MD , Emad Mossad, MD – Journal of Cardiothoracic and Vascular Anesthesia. Volume 18, Issue 5, Pages (October 2004)
 IN PATIENTS UNDERGOING DHCA CBF AND. CMRO2 REMAIN DECREASED AFTER. REWARMING AND WEANING FROM CPB. Sara Lozano, MD , Emad Mossad, MD – Journal of Cardiothoracic and Vascular Anesthesia. Volume 18, Issue 5, Pages (October 2004)")
20
IMPROVING NEUROLOGIC OUTCOMES
20

21
Acid -- Base Management
BLOOD GAS MANAGEMENT (a-stat vs pH-stat) DURING CPB SIGNIFICANTLY AFFECTS CEREBRAL PHYSIOLOGY AN MAY HAVE AN IMPACT ON NEUROLOGICAL OUTCOME ############# من هنا
 DURING CPB SIGNIFICANTLY AFFECTS. CEREBRAL PHYSIOLOGY AN MAY HAVE. AN IMPACT ON NEUROLOGICAL OUTCOME. ############# من هنا.")
22
pH-stat strategy – adding carbon dioxide - compensates for this shift.
Changes in cellular pH during hypothermia are mediated through pco2 homeostasis. When blood is cooled during cardiopulmonary bypass, pH becomes more alkaline. pH-stat strategy – adding carbon dioxide - compensates for this shift. This situation causes pH to increase as temperature decreases and electrochemical neutrality to be maintained. Carbon dioxide is a potent cerebral vasodilator. α-stat strategy – electrochemical neutrality is maintained by keeping pH normal in temperature-uncorrected gases. 22

23
i.e, α-stat strategy – arterial blood measured at 37 C with pH of 7.40 and arterial pCO2 of 40 mm Hg (the hypothermic blood is alkalemic and hypocapneic) pH-stat strategy – hypothermic arterial blood at pH of 7.40 and arterial pCO2 of 40 mm Hg (blood at 37 C is acidemic and hypercapneic)
 pH-stat strategy – hypothermic arterial blood at pH of 7.40 and arterial pCO2 of 40 mm Hg. (blood at 37 C is acidemic and hypercapneic)")
24
PaCO2 26 mmHg PaCO2 26 mmHg PaCO2 40 mmHg
Stat pH stat pH pH 7.26 PaCO2 40 mmHg PaCO2 56 mmHg lab 37oC 28 oC pH pH CO pH 7.4 PaCO2 26 mmHg PaCO2 26 mmHg PaCO2 40 mmHg

25
ADVANTAGES/DISADVANTAGES
α-stat strategy: preserves autoregulation, optimizes cellular enzyme activity, but less metabolic suppression pH-stat strategy: improves cerebral blood flow, cerebral oxygenation, and brain cooling efficiency during CPB, but greater risk of microembolism and free radical-mediated damage 25

26
Higher Hematocrit Improves Cerebral Outcome After Deep Hypothermic Circulatory Arrest
Extreme hemodilution (hematocrit < 10%) causes inadequate oxygen delivery during early cooling and higher hematocrit (30%) achieved with blood prime results in improved cerebral recovery after circulatory arrest. Shin’oka T, Shum-Tim D, Jonas RA, Lidov HGW, Laussen PC, Miura T and du Plessis A Children’s Hospital Boston/Harvard Medical School J Thorac Cardiovasc Surg 1996;112: 26
 causes inadequate oxygen delivery during early cooling and higher hematocrit (30%) achieved with blood prime results in improved cerebral recovery after circulatory arrest. Shin’oka T, Shum-Tim D, Jonas RA, Lidov HGW, Laussen PC, Miura T and du Plessis A. Children’s Hospital Boston/Harvard Medical School. J Thorac Cardiovasc Surg 1996;112:")
27
Temperature Management
No difference between surface and core cooling. Provide adequate duration of cooling (> 20 min) before institution of DHCA. Avoid rapid cooling, avoid rapid rewarming and hyperthermia in postoperative period. Sharma R, et al. Neurological evaluation and intelligence testing in the child with operated congenital heart disease. Ann Thorac Surg 2000; 70: 575–581 Cottrell SM et al. Early postoperative body temperature and developmental outcome after open heart surgery in infants. Ann Thorac Surg 2004; 77: 66–71
 before institution of DHCA. Avoid rapid cooling, avoid rapid rewarming and hyperthermia in postoperative period. Sharma R, et al. Neurological evaluation and intelligence testing in the child. with operated congenital heart disease. Ann Thorac Surg 2000; 70: 575–581. Cottrell SM et al. Early postoperative body temperature and developmental. outcome after open heart surgery in infants. Ann Thorac Surg 2004; 77: 66–71.")
28
Neuroprotective drugs

29
Current recommendations and results of clinical trials
Drug Basis Current recommendations and results of clinical trials Pre-operative use of methyl prednisolone Lesser inflammatory response after CPB; cerebral function recovers earlier. Intravenous methyl prednisolone 10 mg/kg administered 8 hours and 2 hours prior to surgery in high risk groups like neonates Barbiturates Suppresses EEG activity; can cause reduction in high-energy phosphates which is detrimental after circulatory arrest. Not recommended prophylactically Aprotinin Beneficial effect on recovery of cerebral high energy phosphates and intracellular pH. No clear evidence favoring use in pediatric CPB.

30
Allopurinol, NAC May reduce injury due to free radicals. NAC may improve myocardial function. No clear data. NMDA antagonists (magnesium, selfotel) Reduce excitotoxicity No benefit in human trials. Nimodipine (calcium channel antagonist) Reduces cellular injury mediated by calcium influx during reperfusion. Negative results in human stroke trials. Erythropoetin (EPO) EPO switches off apoptosis Limits excitotoxic cell death Mediated by NMDA - R Blocks the inflammatory cascade EPO is a cerebral vasodilator EPO 1000 units/kg IV for 3 doses – 12 hours pre-op / after CPB then 24 hours after.
 Reduce excitotoxicity. No benefit in human trials. Nimodipine (calcium channel antagonist) Reduces cellular injury mediated. by calcium influx during reperfusion. Negative results in human stroke trials. Erythropoetin (EPO) EPO switches off apoptosis. Limits excitotoxic cell death. Mediated by NMDA - R. Blocks the inflammatory cascade. EPO is a cerebral vasodilator. EPO 1000 units/kg IV for 3 doses – 12 hours pre-op / after CPB then 24. hours after.")
31
Slowing of neuronal metabolism Slow apoptosis and block iCa++
Inhaled anesthetics Isoflurane Desflurane Slowing of neuronal metabolism Slow apoptosis and block iCa++ neuronal injury and death. Be placed in the CPB sweep gas flow Vasodilation It would appear desirable to use this agents liberally on CPB. Even seeking to achieve a target blood level while cooling. Especially if DHCA or other such techniques are to be used. CPB: cardiopulmonary bypass; EEG: electroencephalograph; NAC: N-acetyl cysteine; NMDA: N-methyl D-aspartate Langley SM, et al. Eur J Cardiothorac Surg 2000. Clancy RR, et al. Pediatrics 2001. Miller SP, et al. Ann thorac Surg 2004. Bickler PE, Fahlman CS. Anesth Analg 2006, 103.

33
EEG it is a rough guide to anesthetic depth it is affected by temperature,CPB,anesthetics not easy to use BIS (BISPECTRAL INDEX) it is currently used to guide the depth of anesthesia easy to use - less reliable during hypothermia SjVO2 (JUGULAR VENOUS BULB OXYMETRY) it is considered the gold standard of global cerebral oxygenation it is invasive Unilateral SjVO2 may not reflect contralateral events
 it is currently used to guide the depth of anesthesia. easy to use - less reliable during hypothermia. SjVO2 (JUGULAR VENOUS BULB OXYMETRY) it is considered the gold standard of global cerebral. oxygenation. it is invasive. Unilateral SjVO2 may not reflect contralateral events.")
34
TCD (TRANSCRANIAL DOPPLER ULTRASOUND)
it is a sensitive real-time monitor of CBF, can detect microemboli it monitor the middle cerebral artery Absent signal during DHCA. S- 100B (Biochemical marker) Detects preexisting neurologic deficit Multiple sampling periods required NIRS (NEAR-INFRARED SPECTROSCOPY) it is a non-invasive optical technique most devices utilize 2-4 wavelengths of infrared light at nm, where oxygenated and deoxygenated hemoglobin have distinct absorption spectra two depth of light penetration are used to subtract out data from the skin and skull resulting in brain oxygenation value Changes in cerebral vascular composition will affect rSO2 reading Useful during DHCA.
 Detects preexisting neurologic deficit. Multiple sampling periods required. NIRS (NEAR-INFRARED SPECTROSCOPY) it is a non-invasive optical technique. most devices utilize 2-4 wavelengths of infrared light. at nm, where oxygenated and deoxygenated. hemoglobin have distinct absorption spectra. two depth of light penetration are used to subtract. out data from the skin and skull resulting in brain. oxygenation value. Changes in cerebral vascular composition will affect rSO2 reading. Useful during DHCA.")
37
Conclusion Survival after neonatal and infant cardiac surgery has improved dramatically, but quality of life, including neurodevelopmental outcomes, still needs study and improvement. It is important to protect the brain using established strategies,and test new strategies with carefully designed follow-up studies. Potential exists for significant improvement in this area.

38
Thank you

Similar presentations














 ・ In 1998, we developed a modified elephant trunk (ET) technique using a single four-branched arch graft with a sewing “collar” and “long.>")



 Sensitive indicator of perfusion Diagnosis and prognosis of.>")

 Cerebral physiology 1 Explain cerebral ischemia 23 Algorithm for brain protection 4 Strategies.>")

