Download presentation
Presentation is loading. Please wait.

1
Pediatric Tracheostomy
M. Lauren Lalakea MD Chief, Otolaryngology/HNS, Valley Medical Center, San Jose, CA Clinical Associate Professor, Stanford

2
Tracheotomy--Introduction
Initially procedure of last resort to relieve airway obstruction, eg diphtheria, epiglottitis High expectation for short duration, w decannulation Indications expanded to include access for pulmonary toilet and assisted ventilation (polio) nathanclarkecommunication.wikispaces.com Uofmchildrenshospital.org
 nathanclarkecommunication.wikispaces.com. Uofmchildrenshospital.org.")
3
Tracheostomy--Introduction
Current trends: ↓trachs for acute airway obstruction ↑trachs for prolonged ventilation (>50%) ↓decannulation rate: 28—51% ↑trach duration: 2 yrs for those decannulated Avg. age: 2—3 yr, >50% younger than 1 yr Indications Airway obstruction Assisted ventilation Pulmonary toilet
 ↓decannulation rate: 28—51% ↑trach duration: 2 yrs for those decannulated. Avg. age: 2—3 yr, >50% younger than 1 yr. Indications. Airway obstruction. Assisted ventilation. Pulmonary toilet.")
4
Indications Airway obstruction Congenital: Craniofacial anomalies
Bilateral vocal cord paralysis Tracheomalacia Laryngeal anomaly Neoplasm

5
Craniofacial Anomaly: Pierre Robin micrognathia, glossoptosis, cleft palate
php.med.unsw.edu.au

6
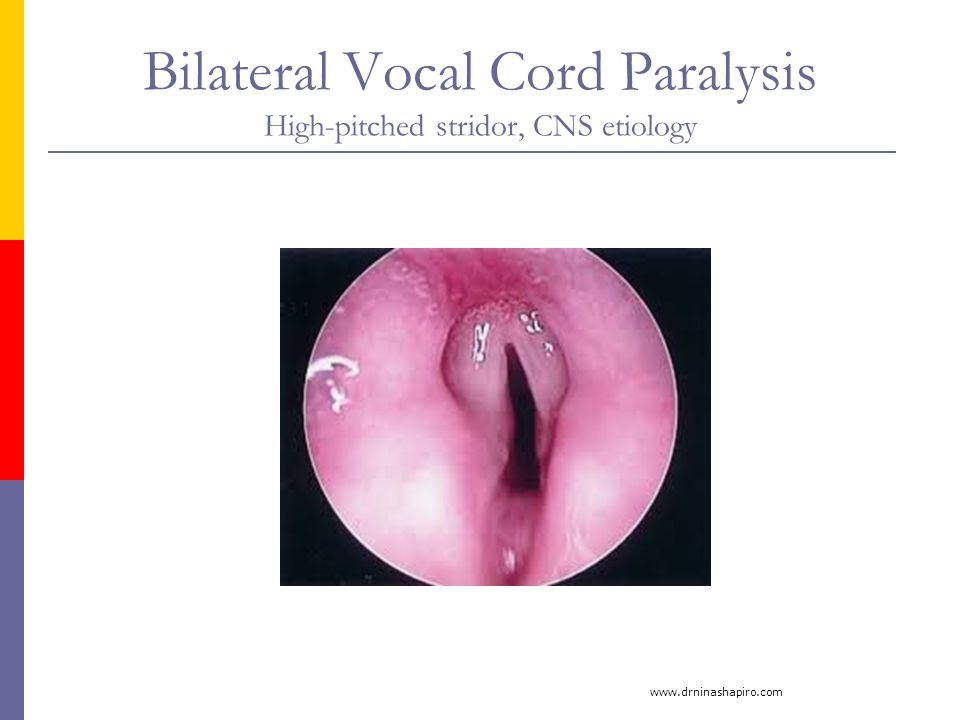
Bilateral Vocal Cord Paralysis High-pitched stridor, CNS etiology
7
Tracheomalacia Inspiratory and expiratory stridor
2011.prepsa.courses.aap.org

8
Laryngeal Anomaly: Glottic Web
wiki.uiowa.edu

9
Neoplasm: Lymphangioma
openi.nlm.nih.gov

10
Indications Airway Obstruction Acquired: Subglottic stenosis
Cricoid is a complete ring ETT -->mucosal ischemia, necrosis Perichondritis, cartilage injury Progressive stridor, failed extubation Trach if med and surgical management fail Recurrent respiratory papillomatosis Trauma emedicine.medscape.com

11
Indications Assisted ventilation Pulmonary toilet
Congenital central hypoventilation Chronic lung dz, eg BPD Neuromuscular disease Pulmonary toilet Neurologically impaired children Recurrent respiratory infections, aspiration

12
Timing of Tracheotomy Controversial in pedi pts
Prolonged intubation → risk of airway injury Incidence of subglottic stenosis low in neonates despite lengthy intubation Meticulous NICU care Pliable larynx and trachea Older children and adults: Consider trach after 2-3 wks of intubation Consider likelihood that underlying process will reverse/improve

13
Pre-Trach Evaluation Airway obstruction
Flexible laryngoscopy—dynamic evaluation Rigid laryngoscopy and bronchoscopy with spontaneous ventilation Any treatable conditions?

14
Pre-Trach Evaluation Dynamic evaluation--laryngomalacia
primehealthchannel.com

15
Pre-Trach Evaluation Assisted Vent + Neurologic Dz All
Discussion with 1° team, Pulmonary, family Goals of care All Wt> 1500 gm, FiO2 <60% Hct, coags Informed Consent

16
Tracheotomy Technique
General Anesthesia, with ETT Vs. LMA or bronchoscope Positioning with neck extended Palpation of landmarks, incision marked Pedi larynx is high, cricoid easiest to palpate Horizontal or vertical incision below cricoid

17
Tracheotomy Technique
Midline dissected, thyroid isthmus divided Stay sutures placed thru rings Trachea opened vertically

18
Tracheotomy Technique
ETT is withdrawn slightly Appropriate trach tube placed Position and adequate ventilation confirmed Tube size adjusted prn Excessive leak Excessive length

19
Tracheotomy Technique
Tube secured with sutures Stay sutures labeled Facilitate tube replacement in case of accidental decannulation Twill tape used around neck to secure trach Snugly tied to prevent dislodgement

20
Tracheostomy Variations
Vertical skin incision Stoma ‘matured’ by suturing skin in 4 quadrants to edges of tracheal incision Allows easier tube replacement if dislodged

21
Post-Operative Care Transport directly to ICU
CXR to confirm tube position, r/o PTX Sedation to minimize risk of accidental decannulation while stoma immature Routine suctioning, humidified air “Do not change trach ties” Obturator, extra trach tubes at bedside Same size, and one size smaller

22
Post-Operative Care First trach change
At 5-7 days post-op 2 ENT MDs Neck extended, fresh tube placed Stay sutures removed, ties changed Confirms that stoma is sufficiently mature to allow future changes by non-surgical personnel Sedation weaned, transfer out of ICU as appropriate

23
Post-Operative Care ‘Hands-on’ caregiver training begins
Infants and young children vulnerable to trach catastrophe Pedi trach tubes are single canula--require meticulous care General trach care, suctioning technique Trach tube changes—q 1-2 wk CPR training Discharge planning

24
Complications Complication rates vary, up to 40—50% Early:
Accidental decannulation False passage, loss of airway Potential for significant morbidity/mortality ↓Risk with: Adequate sedation/ immobilization Appropriately sized and secured tube Close monitoring and nursing care Stay sutures +/- ‘mature’ stoma to facilitate tube replacement sciencedirect.com

25
Complications: Early Tube obstruction/ mucus plugging
Potential for significant morbidity/ mortality in kids Small diameter single canula, vulnerable age group ↓Risk with: Humidified air Frequent suctioning Appropriate monitoring Pneumothorax/ pneumomediastinum 0.6 – 6% Hemorrhage Local infection, skin breakdown

26
Complications--Late Tracheal granuloma—39% Stomal, suprastomal, distal
↓Risk with meticulous trach care, proper suctioning technique Surveillance bronchoscopy, excision to maintain patency tracheostomy.com Utmb.edu

27
Complications: Late Tube obstruction/ mucus plugging – 13%
Accidental decannulation—12% Caregiver training is critical Adequate monitoring and home support Local infection – 9%

28
Complications: Late Speech delay
Smaller trach size allows for better airflow and voicing Passey-Muir valve appropriate for some Early Start and Speech Tx

29
Complications: Late Suprastomal collapse/ malacia – 8%
Tracheal or subglottic stenosis Arterial erosion/ tracheal-innominate fistula “Sentinel Bleed” TE fistula--acquired readcube.com

30
Complications Tracheocutaneous fistula: 11-42% Death
Persistent fistula after successful decannulation ↑Risk if trach duration > 1 yr 90% of ‘Starplasty’ trachs have TC fistula May require surgical repair Death Trach-related = 0 – 3% Accidental decannulation / mucus plugging most common Overall = 8.5 – 19%

31
Trach Tubes: Which are Best?
Cuffed vs. uncuffed Neonatal vs. pediatric Bivona vs. Shiley Single cannula vs. with inner cannula Metal vs. plastic Appropriate length and diameter? Fenestrated Jackson Trach tube Cuffed Shiley Trach with Inner Cannula

32
Trach Tubes: Which are Best?
Fenestrated tube Allows passage of air up thru vocal cords to facilitate speech May ↑ aspiration risk More prone to granulation tissue formation tracheostomy.com

33
Trach Tubes: Which are Best?
Ideal trach tube: Soft enough to conform w/o pressure, injury, discomfort Rigid enough to avoid collapse Material causes minimal tissue reaction Has inner cannula that can be removed and cleaned Not available for plastic pediatric trachs Has stylet or obturator to facilitate insertion Bivona and Shiley meet most criteria

34
Trach Tube Size Guidelines
Length Neonatal vs. Pedi Neonatal equivalent diameter vs. Pedi, but 5-8 mm shorter in length Too short ↑chance of accidental decannulation Too long May abrade carina or rest in right mainstem Longer tubes desirable if tracheal stenosis or malacia Length confirmed by CXR or flex. endoscopy

35
Trach Tube Size Guidelines
Diameter Too large Mucosal injury, stenosis Inability to voice Too small Excessive leak in ventilated pts Inadequate air exchange Difficult to suction adequately Pedi trach tubes sized based on inner diameter, correspond to endotracheal tube sizes

36
Trach Tube Size Guidelines
Child’s Age Inner Diameter (mm) Premie, <1000 gm 2.5 neo Premie, gm 3.0 neo Neonate – 6 mo 3.0 – 3.5, neo 6 mo -- 1 yr 3.5 – 4.0 1 – 2 yr 4.0 – 5.0 > 2 yrs Age/4 + 4
 Premie, <1000 gm. 2.5 neo. Premie, gm. 3.0 neo. Neonate – 6 mo. 3.0 – 3.5, neo. 6 mo -- 1 yr. 3.5 – – 2 yr. 4.0 – 5.0. > 2 yrs. Age/")
37
Shiley Pediatric Trach Tubes
Options: Neo, Pedi, Pedi-Long (PDL), Pedi c Cuff (PDC), Pedi-Long c Cuff (PLC)
, Pedi c Cuff (PDC), Pedi-Long c Cuff (PLC)")
38
Bivona Trachs Similar sizing Cuffed Tubes: TTS (tight to shaft)
Neo and Pedi Cuffed Tubes: TTS (tight to shaft) Excellent option for pts who need cuff Reorder Code Size ID (mm) OD (mm) Length (mm) 67P025 2.5mm 4.0mm 38.0mm 67P030 3.0mm 4.7mm 39.0mm 67P035 3.5mm 5.3mm 40.0mm 67P040 6.0mm 41.0mm 67P045 4.5mm 6.7mm 42.0mm 67P050 5.0mm 7.3mm 44.0mm 67P055 5.5mm 8.0mm 46.0mm
 Excellent option for pts who need cuff. Reorder Code. Size. ID (mm) OD (mm) Length (mm) 67P mm 4.0mm 38.0mm 67P mm 4.7mm 39.0mm 67P mm 5.3mm 40.0mm 67P mm 41.0mm 67P mm 6.7mm 42.0mm 67P mm 7.3mm 44.0mm 67P mm 8.0mm 46.0mm")
39
Bivona FlexTend Trach Tubes
Flexible extended length connection ‘built-in’ to trach

40
Decannulation Suitability: Procedure:
Off ventilator, minimal suctioning requirement, no obstructive pathology Tolerates capping/occlusion Recent bronchoscopy is clear Procedure: Admission to ICU, monitoring Downsizing vs removal, occlusive dressing Observation hrs

Similar presentations



 – Oral-tracheal – Naso-tracheal Tracheostomy (trach) 1.>")






>")
 Internal trauma (Endotracheal intubation, tracheostomy) Other ▪ Systemic diseases (vasculitis,>")





 Amended 2012.>")

