Download presentation
Presentation is loading. Please wait.

1
The Medical Patient The Renal System; Hypertensive Emergencies
Condell Medical Center EMS System October 2008 CE Site Code # E1208 Prepared by: Sharon Hopkins, RN, BSN, EMT-P

2
Objectives Upon successful completion of this module, the EMS provider should be able to: List the components and function of the urinary system State signs and symptoms of chronic kidney disease Define hemodialysis Identify the differences between AV fistulas and AV shunts & implications in the field Apply the Renal SOP’s given a scenario List the steps in performing an abdominal assessment

3
Describe the physical assessment of the patient with flank pain
Describe the management of the patient with flank pain Define the criteria for a hypertensive emergency List the signs and symptoms of hypertensive emergencies Describe the rationale for treatment using Lasix and Nitroglycerin for hypertensive emergencies Describe the proper technique to obtain a blood pressure Describe the components of a neurological assessment

4
Successfully calculate the GCS given the findings of the patient assessment
Return demonstrate pupillary assessment Return demonstrate the in-line Albuterol set-up Return demonstrate the preparation of an Amiodarone IVPB set-up Identify and appropriately state interventions for a variety of EKG rhythms Identify ST elevation on a 12 lead EKG Successfully complete the 10 question quiz with a score of 80% or better

5
Urinary System Contains 4 major structures Kidneys Vital organs
Located in upper abdomen; retroperitoneal area 1 behind the spleen; 1 behind the liver Ureters Urinary bladder Urethra

7
Function of the Urinary System
Major functions Maintains blood volume via proper balance of water, electrolytes, and pH Retains key compounds (ie: glucose) and eliminates wastes (ie: urea) Monitors and maintains arterial blood pressure (in addition to other mechanisms) Regulates erythrocyte (RBC) development
 and eliminates wastes (ie: urea) Monitors and maintains arterial blood pressure (in addition to other mechanisms) Regulates erythrocyte (RBC) development.")
8
Urinary Bladder Storage receptacle for the production of urine until it is convenient or necessary to void Fully distended can hold 500 ml of urine The more distended the bladder, the more vulnerable to blunt trauma After urination, the bladder contains about 10 ml of fluid

9
Chronic Kidney Disease
Can be from a specific kidney disease or as a complication from other conditions Diabetes #1 reason in USA for need for kidney transplant Hypertension Kidney inflammation (glomerulonephritis) Inflammation of blood vessels (vasculitis) Polycystic kidney disease
 Inflammation of blood vessels (vasculitis) Polycystic kidney disease.")
10
Chronic Kidney Disease
Diseased or injured kidneys Blood flow through the renal system decreases Inflammatory changes occur in the glomeruli A group of capillaries where blood is filtered into a nephron (structure that produces urine) Capillary walls thicken decreasing permeability Glomerular filtration rate (GFR) is reduced Volume of blood filtered per day thru glomeruli
 Capillary walls thicken decreasing permeability. Glomerular filtration rate (GFR) is reduced. Volume of blood filtered per day thru glomeruli.")
11
Symptoms of Chronic Kidney Disease
Most common symptoms Swelling, usually of lower extremities Fatigue Weight loss, loss of appetite Nausea and/or vomiting Change in urination Reduction in volume or frequency Change in sleep patterns Headache Itching – high levels of phosphorus in system; dry skin Difficulties with memory or concentration

12
Complications of Chronic Kidney Disease
Hypertension May be a leading cause but can also develop in the early stages as a complication Anemia Decreased production of red blood cells Bone disease Disorders of calcium and phosphorus Malnutrition Altered functional status and well-being

13
Dialysis Dialysis is required when the kidneys fail and a transplant is not performed Peritoneal dialysis uses a catheter thru the abdominal wall to filter the blood

14
Hemodialysis Hemodialysis is a procedure in which a machine filters harmful waste and excess salt and fluid from your body Access points are created to be functional within weeks and to last several to many years Usual access point is the forearm

15
Fistulas and Shunts Arteriovenous (AV) fistula
Most common type of access Fistula created internally by sewing an artery to a vein forming a small opening between the two Pressure from the arterial flow eventually enlarges and strengthens the vein May take 6 weeks to heal but can last for years

17
Arteriovenous (AV) graft
Access is similar to a fistula A synthetic tube is used to surgically connect the artery to the vein AV graft often heals within 2-3 weeks With proper care, can last several years Higher likelihood of forming clots or becoming infected than an AV fistula

18
Renal Dialysis

19
Hemodialysis Most people treated with hemodialysis 3 times a week
Each session lasts approximately 3-5 hours Some patients, at some dialysis centers, may choose daily dialysis Usually performed 6 days per week for 2 – 21/2 hours each session Patients often report improved B/P and quality of life

20
Continuous Ambulatory Peritoneal Dialysis
CAPD is a self-care treatment where the patient instills dialysate fluid into the peritoneal (abdominal) cavity through a surgically implanted catheter through the abdominal wall The dialysate stays in the abdominal cavity a prescribed period of time and then is drained out
 cavity through a surgically implanted catheter through the abdominal wall. The dialysate stays in the abdominal cavity a prescribed period of time and then is drained out.")
21
CAPD Instructions Do not disconnect the CAPD bags from the catheter
If the patient is transported, transport with the drainage bag remaining below the level of the patient’s waist Do not infuse any fluids or medications directly into the catheter This IS NOT an alternate IV site Transport the patient with the CAPD intact

22
Renal Protocol Care of Patients with Grafts or Shunts
Do NOT take B/P on arm with active fistula or graft Do NOT start IV on arm with active fistula or graft If site is bleeding, apply direct pressure In case of arrest and no IV access consider IO site Access of fistula or graft is only with contact to Medical Control

23
Care of The Renal Patient
Best to err on the side of conservative treatment Monitor and support the ABC’s High flow O2 is appropriate to maximize respiratory efficiency Carefully monitor fluid administration Monitor cardiac rhythm for disturbances Caregivers can help manage the additional equipment on the patient

24
Abdominal Pain Assessment
Chief complaint The sign or symptoms that prompted the patient to call for help Use an open – ended question to determine the reason for the call “Why did you call us today?” or “What seems to be the problem?” During the interview the chief complaint generally becomes more specific

25
Assessment O – onset of the problem P – provocation/palliation
Did problem start suddenly or gradually? What was patient doing at the time? P – provocation/palliation What makes the symptoms worse? Better? Q – quality In the patient’s own words how do they describe their pain (ie: crushing, tearing, sharp, dull?)
")
26
R – region/radiation Where is the symptom? Does it move?
If the patient uses one finger or isolates to one spot, the pain is considered localized If the pain is described using both hands or indicating a larger area, the pain is diffuse Is there referred pain (pain felt in a body area away from the source)?
")
27
S – severity T – time Intensity of pain or discomfort 0 – 10 scale
“0” is no pain; “10” is the worse pain in your life Can the patient be distracted? Do they lie still or are they writhing about? T – time When did the symptoms begin?

28
Associated symptoms Pertinent negatives
Are other symptoms present that are commonly linked to certain diseases that can help rule in or out your diagnosis? Pertinent negatives Are any likely associated symptoms absent? Absence of symptoms can be information as helpful as presence of other symptoms

29
Assessment Pitfalls in the Chronic Renal Patient
The challenge to the medical professional is to separate the acute complaint from the chronic condition What is new today that changes your status? Many of these patients have unstable baselines to start with Fluid and electrolyte imbalance EKG disturbances

30
Physical Assessment - Abdomen
Boundaries run from xiphoid process to symphysis pubis A full bladder will distort assessment and increase discomfort for the patient To relax the abdominal wall or to ease pain, a pillow placed under the knees would be helpful Start by asking the patient where it hurts Examine painful areas last

31
Warm your hands and stethoscope
If hands are cold, palpate over clothing until hands warm up Monitor facial expressions for pain or discomfort Validate the facial expression Often the patient scrunches their face in anticipation of pain Assessment techniques to use Inspection, auscultation, percussion, lastly palpation

32
Abdominal Assessment Techniques
Inspection A visual review looking for abnormalities Auscultation Move the stethoscope in a circle approximately 2 inches from the umbilicus listening for bowel sounds Normal bowel sounds gurgle approximately every 5-15 seconds

33
Percussion Not often performed in the field Helps determine size and location of organs Determines gas, solid, and fluid filled areas Tympany heard over most of abdomen Dullness percussed over spleen and liver

34
Palpation Palpate painful areas last To increase comfort to patient, have them take slow, deep breaths thru open mouth Flexing knees relaxes abdominal wall Abdominal pain on light palpation indicates peritoneal irritation or inflammation Voluntary guarding – patient anticipates pain or is not relaxed Involuntary guarding – peritoneal inflammation (lining of abdominal cavity)
")
35
SOP Abdominal Pain Stable Patient
Routine medical care Watch the patient for vomiting Stable patient Patient alert Skin warm and dry Systolic B/P > 100 mmHg Contact Medical Control for pain management

36
SOP Abdominal Pain Unstable Patient
Routine medical care Watch the patient for vomiting Unstable patient Altered mental status Systolic B/P < 100 mmHg Establish IV; x2 if possible Fluid challenge in 200 ml increments 20 ml/kg in pediatric patient (max 3 challenges) Contact Medical control for pain management
 Contact Medical control for pain management.")
37
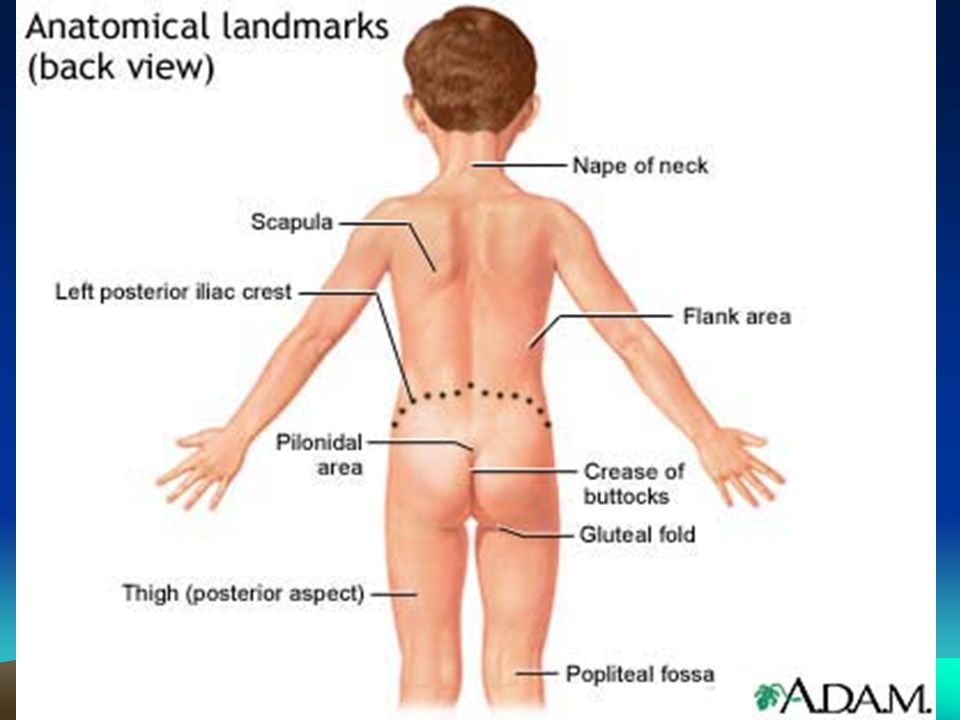
Flank Pain Where’s the flank? What organs lie in the flank areas?
The area of the back below the ribs and above the hip bones What organs lie in the flank areas? The kidneys What is a common reason for flank pain? Renal calculi (aka kidney stones)
")
39
Causes of flank pain

40
Kidney Stones The formation of crystals in the kidney’s collection system Hospitalization common for pain control and fluid hydration Additional inpatient treatment may be necessary Lithotripsy – sound waves used to break apart larger stones into smaller ones that can be passed during urination

41
Kidney Stones More common in males Suggestion of hereditary patterns
Risk factors include immobility and certain medications (anesthetics, opiates, psychotropic drugs) Stones can form in metabolic disorders (ie: gout) Production of excessive uric acid and calcium
 Stones can form in metabolic disorders (ie: gout) Production of excessive uric acid and calcium.")
42
Stones From Calcium Salts
The most common type of stone 75 – 85% of all stones Calcium stones 2 – 3 times more common in men Average age of onset 20 – 30 years Familial indication History of one stone and patient likely to form another one within 2 – 3 years

43
Struvite Stones Represent 10 – 15% of all stones
Formation associated with chronic urinary tract infection or frequent bladder catheterization Patients with spinal cord injuries Patients with spina bifida More common in women (due to their higher incidence of UTI’s)
")
44
Uric Acid Stones The least common of all stones Form more often in men
Tend to occur with family histories so most likely a hereditary component Half of patients with uric acid stones have gout

45
Patient Assessment Chief complaint almost always severe pain
Kidney stones considered to be the most painful medical condition Pain started vague, dull, poorly localized (visceral pain) in one flank Within 30 – 60 minutes pain is extremely sharp, remains in the flank and radiates downward and anteriorly to the groin
 in one flank. Within 30 – 60 minutes pain is extremely sharp, remains in the flank and radiates downward and anteriorly to the groin.")
46
Physical Exam Agitated, restless, uncomfortable patient
B/P and heart rate elevated with the pain Skin typically pale, cool, clammy Patient may not be able to lie still for abdominal examination Observed urine sample may have gross hematuria or will be evident in lab analysis

47
Management Position of comfort Be prepared for vomiting (due to pain)
IV fluids for volume replacement and as a drug route, and to promote urine formation and movement through the system to flush through the stone Analgesia for pain – limited amounts used in the field often have minimal effect, if at all

48
SOP Flank Pain SOP treatment same as abdominal pain
Call Medical Control to obtain pain medication orders Be patient’s advocate for pain control Kidney stones are considered the most painful human condition (just ask someone who has had one!)
")
49
Hypertensive Emergency
A life-threatening crisis with an acute elevation of the blood pressure Systolic B/P > 230 mmHg Diastolic B/P > 120 mmHg Usually seen in patients with untreated or poorly controlled hypertension

50
Hypertensive Emergency
Signs and symptoms Epistaxis – nosebleed The nasal tissue is very thin and prone to bleed Headache “The worst headache in my life” often indicates a subarachnoid bleed Visual disturbances (ie: blurred, blindness)
")
51
Restlessness Confusion Nausea and vomiting Neurologicial changes Altered mental status to seizures to coma Complications Hypertensive encephalopathy Severe headache, vomiting, visual changes, paralysis, seizures, stupor, coma Ischemic (clot) or hemorrhagic (bleed) stroke
 or hemorrhagic (bleed) stroke.")
52
Field Assessment Chief complaint received is often headache
Additional accompanying complaints Nausea and/or vomiting Blurred vision Shortness of breath Epistaxis (nosebleed) Vertigo (dizziness) Level of consciousness may be normal, altered, or patient may be unconscious
 Vertigo (dizziness) Level of consciousness may be normal, altered, or patient may be unconscious.")
53
Field Assessment Findings Skin may be pale, flushed, or normal
Skin may be warm or cool; moist or dry If hypertensive encephalopathy is present, it may cause left ventricular failure Patient will be in pulmonary edema Lung sounds clear unless in pulmonary edema Pulse often strong and bounding

54
SOP - Hypertensive Emergency
Routine Medical Care Obtain and record the B/P in both arms Monitor & record vital signs and neuro status every 5 minutes Lasix 40 mg IVP 80mg if already on Lasix at home Contact Medical control for further orders Possible Nitroglycerin order

55
Treating Hypertensive Emergencies
Initial goal To achieve a progressive, controlled reduction in the blood pressure to minimize risks of hypoperfusion in the vascular beds in cerebral, coronary, and renal blood flow Goal is not to reduce the blood pressure to “normal” levels as fast as possible

56
Why Give Lasix? Lasix is a venodilator and a diuretic
By dilating blood vessels, blood pressure can be decreased Venodilator effect noticed before evidence of diuretic effects are seen Decreasing fluid volume is another method to reduce the blood pressure by reducing the volume to be pumped

57
Why Give Nitroglycerin
Primarily a venodilator Will dilate the diameter of blood vessels Decreases blood pressure Especially useful in the patient with coronary ischemia Still need to screen for use of Viagra or Viagra type drugs in the past hours

58
Obtaining A Blood Pressure

59
Blood Pressure Measurement
Poor technique can result in inaccurate values Patient’s arm should be at the same vertical height as the heart The cuff bladder should fit snugly around the arm The lower edge of the cuff should be placed 1 inch above the brachial artery The bladder should be centered over the brachial artery

60
The bell end of the stethoscope will produce better sounds
The diaphragm is easier to place and hold with one hand The cuff and tubing should not be touching clothes which can give false sounds After the cuff is pumped up, the air should be released slowly Air released too fast may cause an inaccurate measurement to be read Cracked tubing causes air to leak too fast

61
Obese Site & B/P Cuff Wrap the blood pressure cuff around the forearm
Center the bladder over the radial artery Place the stethoscope over the radial artery Obtain and document the blood pressure in the usual manner (ie: 120/80)
")
62
Blood Pressure by Palpation
Rough estimation of the systolic value Palpate for the loss of the radial or brachial pulse and continue to inflate the cuff an additional 30 points Slowly release the air and when the pulse is first felt, this is the recorded systolic B/P Document the reading as “100/palpation”

63
Rough Estimate of Blood Pressure By Palpation
A rough guideline; accuracy is debatable If the radial pulse is palpated, the B/P is said to be roughly 80 mmHg If the femoral pulse is palpated, the B/P is said to be roughly 70 mmHg If only the carotid (central) pulse is felt, the B/P is said to be roughly 60 mmHg
 pulse is felt, the B/P is said to be roughly 60 mmHg.")
64
A “Neuro” Assessment Level of consciousness
A – alert (means awake but not necessarily oriented; spontaneous eye opening; responds to voice but can be confused; and has motor function ) V – responds to verbal command no matter how slight and type of response P – responds to pain or tactile stimuli only U – unresponsive with no eye, voice, or motor response at all to voice or pain
 V – responds to verbal command no matter how slight and type of response. P – responds to pain or tactile stimuli only. U – unresponsive with no eye, voice, or motor response at all to voice or pain.")
65
Ask 2 questions to determine level of consciousness
“What month is this?” “How old are you?” Obtain the Glasgow Coma Scale (GCS) on all EMS patients Best eye opening (4 points) Best verbal response (5 points) Best motor response (6 points) Evaluate pupillary response
 on all EMS patients. Best eye opening (4 points) Best verbal response (5 points) Best motor response (6 points) Evaluate pupillary response.")
66
Performing a Pupillary Check
Ask patient to focus on an object (ie: tip of your nose) Bring the light in from the side and out the same way Without shining in the eyes move the penlight into position for the opposite side and repeat
 Bring the light in from the side and out the same way. Without shining in the eyes move the penlight into position for the opposite side and repeat.")
67
Check muscle tone and strength Evaluate facial symmetry (smile)
Vital signs Signs of increasing intracranial pressure include increasing B/P and dropping heart rate Check muscle tone and strength Evaluate facial symmetry (smile) Evaluate clarity of speech The above 3 are the Cincinnati Stroke Scale Arm drift, facial symmetry, speech Additionally: Coordination or gait and sensory Movement and sensation
 Evaluate clarity of speech. The above 3 are the Cincinnati Stroke Scale. Arm drift, facial symmetry, speech. Additionally: Coordination or gait and sensory. Movement and sensation.")
68
Repeat Assessment If you want to see where the patient is going, you’ve got to know where they’re coming from GET A BASELINE EVALUATION You can anticipate something happening if you are watching the trends PERFORM REPEAT ASSESSMENTS AS OFTEN AS INDICATED Prevents surprises

69
Need to constantly monitor the situation
Watch for trends Anticipate surprises

70
Pain Management SOP Routine trauma or medical care
Continuous patient monitoring Respiratory status SaO2 Blood pressure Morphine 2 mg slow IVP over 2 minutes May repeat every 2 minutes Maximum total 10 mg

71
Respiratory Depression Related to Morphine Use
Supportive oxygenation If SaO2 is falling and ventilation rates are declining, consider supportive bagging Ventilation rates for supportive bagging (AHA) Adult 1 breath every 5 – 6 seconds Pediatric patients 8 and less 1 breath every 3 – 5 seconds Narcan (narcotic antagonist) 2 mg IVP if respiratory depression
 Adult 1 breath every 5 – 6 seconds. Pediatric patients 8 and less 1 breath every 3 – 5 seconds. Narcan (narcotic antagonist) 2 mg IVP if respiratory depression.")
72
Glasgow Coma Scale Exercise
Review the following 3 patient’s assessment findings Evaluate for their GCS Determine the best response and score the patients Best eye opening points Best verbal response 1 – 5 points Best motor response points Note: GCS to be obtained on all patients!

73
GCS Exercise #1 You are assessing a 56 year-old patient
The patient is unresponsive. Nothing happens when you call the patient’s name. when you pinch the patient, their eyes open, then close. When pinched, the patient says “don’t, stop” and then is silent. When pinched, the patient pushes you away

74
GCS Exercise #2 Your patient is a 16 year-old male.
Upon approaching, the patient’s eyes are open and they are looking around with an anxious look. They do not answer questions; they groan if pinched. They do not follow commands. When touched, the patient grabs your arm and doesn’t let go.

75
GCS Exercise #3 Your patient is an 8 month-old.
Their eyes are closed. There is no response to pinching. When pinched, the patient groans weakly. When pinched, the patient tries to pull away or turn away from the evaluator.

76
GCS Exercise Answers GCS #1 total –11 GCS #2 total – 11
Eye opening – 2 Verbal response – 4 Motor response – 5 GCS #2 total – 11 Eye opening – 4 Verbal response – 2 Motor response - 5 GCS #3 total – 7 Eye opening – 1 Verbal response – 2 (groans to pain – incomprehensible words) Motor response – 4 (withdraws to pain)
 Motor response – 4. (withdraws to pain)")
77
Skill – In-line Albuterol
For Albuterol to have its bronchodilating effects, it must be delivered down into the lungs If the patient can’t inhale it in, we have to push it in

78
Normal use with corrugated tubing connected to the T-piece
Kit connected to oxygen and run at 6 l/minute (enough to create a mist). Nebulizer kept upright at all times.
. Nebulizer kept upright at all times.")
79
In-line Albuterol Intubate the patient
While waiting to intubate, can “bag” the Albuterol into the lungs via in-line set-up thru ambu mask Confirm placement in the usual manner visualization chest rise & fall 5 point auscultation ETCO2 detector Evaluated after 6 breaths are delivered

80
To adapt nebulizer to in-line use:
Remove mouthpiece from T-piece and replace with BVM Connect nebulizer to oxygen source

81
Corrugated tubing left in place on T-piece
Clear adaptor placed on distal end of corrugated tubing Once intubated, clear adaptor connected to ETT

82
The BVM helps push the Albuterol where it will do the most good.
Albuterol will be effective if it gets into the bronchial system, not just into the back of the throat. The BVM helps push the Albuterol where it will do the most good.

83
EKG Review & Treatment There is NO pulse!!! The patient has no pulse!
6 second strip The patient has no pulse!

84
EKG Interpretation #1 PEA with a rate over 60 CPR Secure airway
Search for causes (6 H’s; 5 T’s) Establish IV/IO access Epinephrine 1:10,000 1 mg IVP/IO every 3-5 minutes No Atropine – rate over 60
 Establish IV/IO access. Epinephrine 1:10,000 1 mg IVP/IO every 3-5 minutes. No Atropine – rate over 60.")
85
6 H’s Hypovolemia – fluid challenge Hypoxia – supplemented oxygen flow
Hydrogen ion – acidosis – ventilate (breathe) for the patient Hyper/Hypokalemia – electrolyte imbalance Hypothermia – warm them up Hypoglycemia – screen all unconscious/altered level of consciousness patients for glucose level
 for the patient. Hyper/Hypokalemia – electrolyte imbalance. Hypothermia – warm them up. Hypoglycemia – screen all unconscious/altered level of consciousness patients for glucose level.")
86
5 T’s Toxins – think little kids getting into the wrong places (ie: purses, cabinets) Tamponade, cardiac Tension pneumothorax – needle decompression Thrombosis, coronary Thrombosis, pulmonary (embolism) Trauma
 Trauma.")
87
EKG Review & Treatment

88
EKG Interpretation #2 Strip A – complete heart block
Strip B – paced rhythm Unstable Type II and 3rd degree heart blocks Patient often unstable due to slow heart rate Begin TCP Rate: 80/minute Sensitivity: auto/demand Output: lowest mA until capture

89
Comfort Measures For TCP
Valium 2 mg IVP slowly over 2 minutes May repeat 2 mg IVP every 2 minutes Maximum of 10 mg Can touch the patient and not receive shocks It’s the patient that feels the electrical stimulation

90
EKG Review & Treatment

91
EKG Interpretation #3 VT – wide complex, until proven otherwise, is VT
2 questions to ask for all tachycardias Question #1 – is patient stable or unstable Evaluate LOC and B/P If you are not perfusing, you cannot maintain an adequate level of consciousness or blood pressure If unstable, prepare for immediate cardioversion If stable, ask question #2

92
2nd Question To Ask if Stable Tachycardia
Question #2 – is complex (QRS) narrow or wide? Narrow think SVT Adenosine is drug of choice Wide think VT EMS choice between Amiodarone or Lidocaine Mixing the antidysrhythmics makes the heart more irritable Let the ED know which drug therapy was started
 narrow or wide Narrow think SVT. Adenosine is drug of choice. Wide think VT. EMS choice between Amiodarone or Lidocaine. Mixing the antidysrhythmics makes the heart more irritable. Let the ED know which drug therapy was started.")
93
If stable VT Antidysrhythmic treatment
Amiodarone 150 mg diluted in 100 ml D5W IVPB Draw up Amiodarone dose, add to 100 ml D5W IV bag and gently agitate to mix; label the bag (drug, amount, time added) Run thru mini-drip tubing; piggyback into the primary IV line Run over 10 minutes (rapid drip rate just below wide open) OR Lidocaine 0.75 mg/kg IVP x1 Contact Medical Control for further orders
 Run thru mini-drip tubing; piggyback into the primary IV line. Run over 10 minutes (rapid drip rate just below wide open) OR Lidocaine 0.75 mg/kg IVP x1. Contact Medical Control for further orders.")
94
EKG Review & Treatment

95
EKG Interpretation #4 Sinus bradycardia
If symptomatic/unstable (poor cardiac output with altered mental status and B/P <100) Atropine 0.5 mg rapid IVP “When they’re alive give them 0.5” May repeat every 3-5 minutes to a max of 3 mg If ineffective begin TCP If TCP ineffective, treat per Cardiogenic Shock IV fluid challenge in 200 ml increments, Dopamine drip
 Atropine 0.5 mg rapid IVP. When they’re alive give them 0.5 May repeat every 3-5 minutes to a max of 3 mg. If ineffective begin TCP. If TCP ineffective, treat per Cardiogenic Shock. IV fluid challenge in 200 ml increments, Dopamine drip.")
96
Where’s ST elevation?

97
12 Lead Interpretation #1 ST elevation in exercise #1
V1 – V3 12 lead obtained in field EMS to evaluate the 12 lead looking for patterns of ST elevation I, aVL, V5, V6 II, III, aVF Any contiguous V leads EMS to call in what they see & fax the 12 lead

98
Where’s the ST elevation?

99
12 Lead Interpretation #2 ST elevation in exercise #2
V2 – V4 12 lead obtained in field EMS to evaluate the 12 lead looking for patterns of ST elevation I, aVL, V5, V6 II, III, aVF Any contiguous V leads EMS to call in what they see & fax the 12 lead

100
Where’s the ST elevation?

101
12 Lead Interpretation #3 ST elevation in exercise #3
II, III, aVF 12 lead obtained in field EMS to evaluate the 12 lead looking for patterns of ST elevation I, aVL, V5, V6 Any contiguous V leads EMS to call in what they see & fax the 12 lead

102
Bibliography Bledsoe, Porter, Cherry. Paramedic Care; Principles & Practices. 3rd Edition. Brady Burrows-Hudson, S. Chronic Kidney Disease. AJN. Feb Vol 105, No2.

Similar presentations






>")














