Download presentation
Presentation is loading. Please wait.

1
PSYCHOLOGY & NEUROSCIENCE
DRUGS AND BEHAVIOR PSYCHOLOGY 305 GARY L WENK PROFESSOR PSYCHOLOGY & NEUROSCIENCE

2
ORDER OF LECTURE TOPICS
Introduction to Pharmacology Principles of Drug Action Acetylcholinergic System Drugs Catecholaminergic System Drugs Serotonergic System & Related Hallucinogens CANNABINOIDS GABAergic System: Alcohol, Barbiturates and Benzodiazepines OPIATES OTC Drugs

3
One guiding principle: everyone is treated consistently.
No extra credit for any reason. There are three major exams Exams will only cover material that is presented in class. If I do not cover a topic in class it will not be on an exam.

4
Be courteous of your fellow students.
You may come in late, leave early, sleep, eat, drink, read the newspaper, text message your friends, listen to your iPod, … Just do it quietly and do not disturb other students who are trying to pay attention to the lecture.

5
This course is about the brain, not the drugs.
Studying the effects of drugs upon the brain can teach us how the brain works.

6
If the book differs from anything I say.
-- I am right & the book is wrong. Bring it to my attention. Some of you may know more about selected drugs or certain issues than I do. Contribute your knowledge to the class (and to me) and correct me if I say something incorrect. I will try to always define the boundaries of the grey areas of my knowledge as well as that of the scientific community.
 and correct me if I say something incorrect. I will try to always define the boundaries of the grey areas of my knowledge as well as that of the scientific community.")
7
The drugs that I will discuss are psychoactive.
The term "psychopharmaceutical" first appeared in 1548 in the title to a collection of prayers of consolation, and prayers for the dead, called: "psychopharmakon, hoc est: medicina animae." The term here related to spiritual medicine, which was to be used in miserable and hopeless situations in life.

8
The word "pharmakos" originally meant scapegoat; a pharmakos was a person who was sacrificed as a remedy for whatever maladies another person might have been experiencing. Around 600 BC the term came to refer to medicine, drug or poison.

9
Naturally occurring psychoactive agents are fundamental to most cultures and the routine use of stimulants and depressants is so pervasive in most western societies that most of us don't even consider such substances to be drugs, but rather an actual nutrient. Indeed, the border between drug and nutrient is blurring.

10
How many people can get through the day without the assistance of the “natural drugs” coffee, tea, tobacco, alcohol, cocoa, or their illegal cousins marijuana, cocaine, or heroin? I want you to keep in mind that anything you take into your body should be considered a drug, whether it's obviously nutritious or not.

12
Our ancestors were very aware of these properties and sought them out for remedies for a variety of illnesses. The use of plant and synthetic products as medicine is but one in a long line of revolutions that occurred to alter culture and the way we view drugs.

13
The first revolution: -- treatment of communicable diseases. Pasteur and Koch (19th century) developed vaccines against measles and other disorders. This introduced us to drug taking on a large scale.
 developed vaccines against measles and other disorders. This introduced us to drug taking on a large scale.")
14
The second pharmacological revolution resulted from the evolution of sulpha drugs: penicillin, and the broad spectrum antibiotic agents. The third pharmacological revolution was the advent of tranquilizers for the treatment of the mentally ill (1950's). First time that compounds were widely used for their effect on the mind and not on the body.
. First time that compounds were widely used for their effect on the mind and not on the body.")
15
The fourth pharmacological revolution is still in progress.
Development of oral contraceptives. Their impact cannot yet be predicted. Over 10 million American women now using oral contraceptives. The most important point - for the first time, potent chemicals are being widely used by healthy people because of their social convenience. The evolution of our view of drugs that affect the brain continues with the introduction of cognitive enhancing drugs and neuroprotectants.

16
4 basic principles First: drugs per se are not "good" or "bad". When drug abuse is talked about, it is the behavior, the way the drug is being used, that is being referred to as bad. Drugs are simply chemicals! Second: every drug has multiple effects, they act in many different areas of the brain and may have different effects than intended. Third: the effects of a drug depend on the amount taken. Varying doses can change the magnitude and the character of the drug effect. This is called a dose-response effect.

17
Fourth: (possibly the most difficult to document) the effects depend in part on the individual's history and expectations of the drug taking experience. Conclusion: essentially it means that every drug experience is a mix of three ingredients: the drug itself, the individual taking the drug, and the setting in which the drug is taken.

18
Principles of Drug Action
Introduction to Pharmacology Principles of Drug Action

19
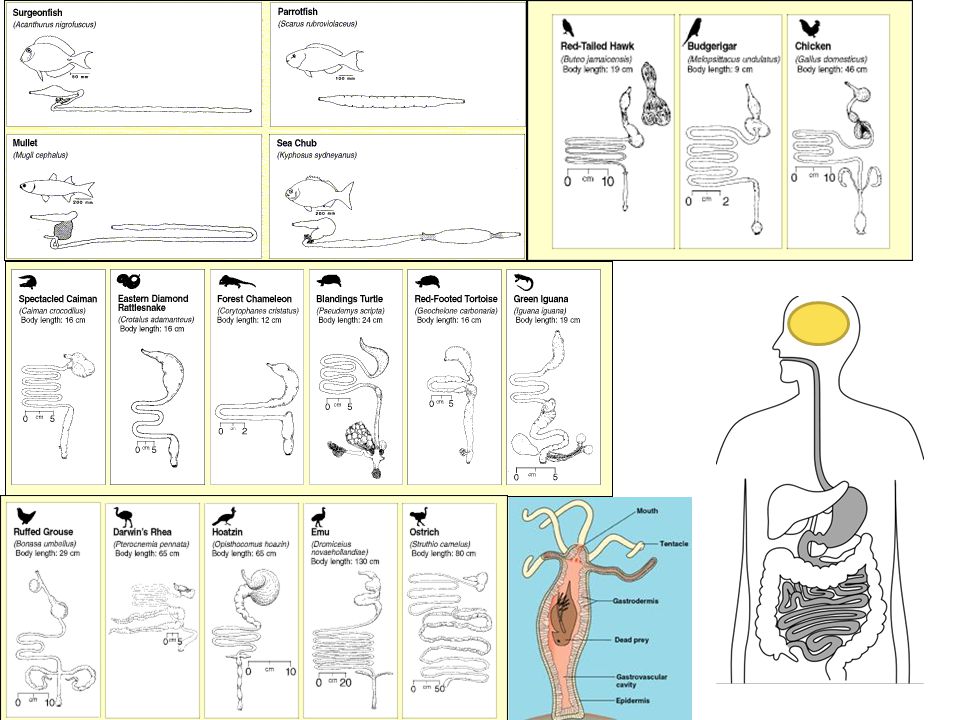
Principles of drug action
The part of the body where the drug acts to produce its effect is called the drug's "site of action." Drugs differ in their site of action. The effects of a drug provide clues to its site of action. For example: drugs that effect sleep, alter activity in the reticular activating system. Another clue to site of action is afforded by the unequal distribution of neurotransmitters in the brain. For example: dopamine is highly concentrated in the basal ganglia, which controls movement. Therefore, administration of drugs that affect the dopamine system may affect disorders of movement, such as in Parkinson's disease.

20
For a drug to produce an effect it must achieve an Adequate Concentration at its site of action.
Relevant factors are The route of administration The amount administered The extent and rate of absorption from the area of administration Distribution within the body Binding or localization in tissues Biotransformation Excretion

21
mq-fig jpg

22
4 Characteristics of the drug influence absorption
The route of administration 4 Characteristics of the drug influence absorption Molecular size and shape Solubility at site of its absorption Degree of ionization Relative lipid solubility of ionized and non-ionized forms

23
Route of administration
Enteral vs. Parenteral routes of administration Enteral routes include oral, rectal and sublingal. Drugs administered by enteral routes reach the liver before going into general circulation. This makes it possible for the drug to be metabolized by liver enzymes prior to being absorbed into the bloodstream for general circulation. Rectal route is useful when oral ingestion is precluded by vomiting or when the patient is unconscious. About 50% of the drug passes through the liver; thus this way is even better than orally. However absorption is often irregular and incomplete.

25
The exception is the sublingual administration.
Drugs given by this route do not go through the liver first. For this reason, nitroglycerin is given sublingually (or as a tongue spray). It is non-ionic, very lipid soluble, and very potent. Venous drainage from the mouth is to the superior vena cava and thus avoids the liver.
. It is non-ionic, very lipid soluble, and very potent. Venous drainage from the mouth is to the superior vena cava and thus avoids the liver.")
26
Absorption after ingestion is effected by pH gradient between the drug and absorbing surface.
In the stomach, which is highly acidic, acidic drugs are absorbed while basic drugs tend to accumulate. In the intestine, which is only slightly acidic, basic drugs are better absorbed than acidic drugs.

27
mq-table jpg

28
Effect of ionization on drug absorption
Non-ionized drugs can easily pass through membranes Ionized drugs can not easily pass through membranes mq-fig jpg

29
The route of administration
Intestinal contents affect absorption: E.G., Dietary fat increases the absorption of fat soluble vitamins and drugs. The quantity of food in the stomach is also important. Drugs are absorbed fastest and most completely when the stomach is empty.

30
The route of administration
Orally administered drugs are primarily absorbed through the small intestine. The passage of drugs from the stomach to the intestine is effected by the temperature of the solution, size of particles and pH of stomach Stability of the drug in the intestines is an important consideration. Must be resistant to low pH and digestive processes.

31
The route of administration
Injection and inhalation are called parenteral routes. This means by route other than via the intestines, including intravenous, subcutaneous, and intramuscular routes.

32
mq-fig jpg

33
Parenteral absorption is much faster than Enteral
mq-fig jpg

36
mq-table jpg

37
3) The extent and rate of absorption from the area of administration
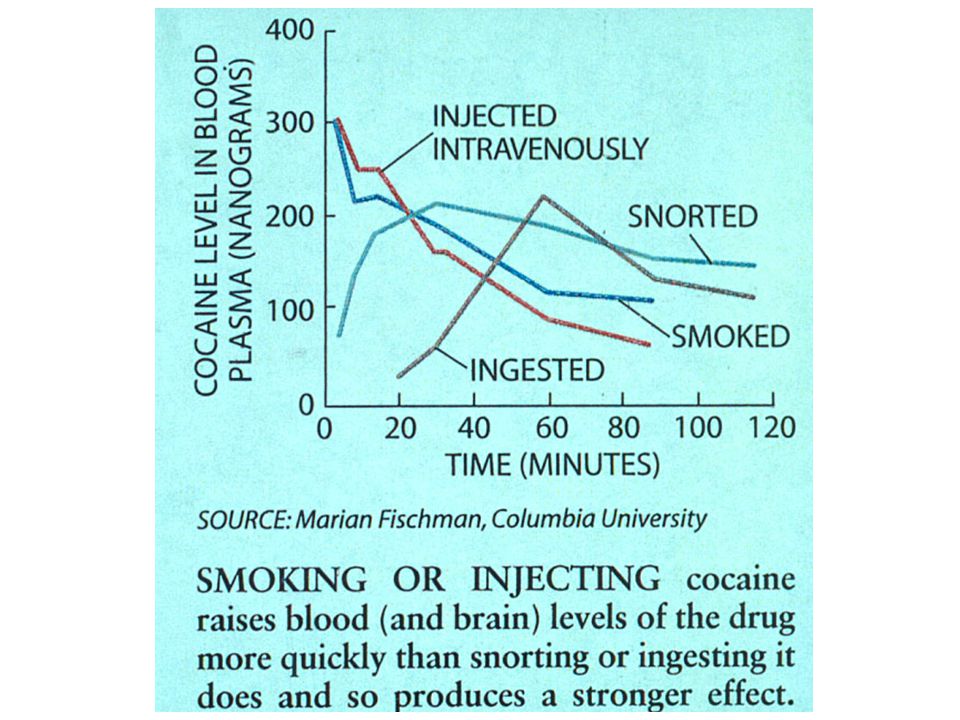
If a drug increases the blood flow into its own region, it enhances its own rate of absorption. Conversely: if a drug constricts blood vessels in the region, it closes down its own absorption into the body, e.g.. Cocaine.

38
Topical applications: Mucous vs. Skin surfaces
3) The extent and rate of absorption from the area of administration Topical applications: Mucous vs. Skin surfaces Mucous membranes - fast absorption. Skin - few drugs can readily penetrate the intact skin. Absorption is usually proportional to surface area over which they are applied and to their lipid solubility. Dermis is freely permeable to many drugs. Consequently, systemic absorption occurs more readily through abraded, burned, or denuded skin. Inflammation can also enhance absorption. Hydrated skin is more permeable than dry skin. Suspending the drug in oily vehicle and rubbing onto skin can also enhance absorption- known as inunction. (Inner forearm)
 The extent and rate of absorption from the area of administration. Topical applications: Mucous vs. Skin surfaces. Mucous membranes - fast absorption. Skin - few drugs can readily penetrate the intact skin. Absorption is usually proportional to surface area over which they are applied and to their lipid solubility. Dermis is freely permeable to many drugs. Consequently, systemic absorption occurs more readily through abraded, burned, or denuded skin. Inflammation can also enhance absorption. Hydrated skin is more permeable than dry skin. Suspending the drug in oily vehicle and rubbing onto skin can also enhance absorption- known as inunction. (Inner forearm)")
39
4) Distribution within the body
After a drug is absorbed, it must be transported to its site of action. For most behaviorally active drugs, the site is the brain. Well vascularized areas will have highest concentration of drug. -- Brain receives 20% of blood flow from heart. The elderly also have reduced cardiac output and increased circulation time all of which may impair the distribution of drugs. The consequence is an increased latency of onset, and prolonged action of the drug because it is not rapidly removed from its site of action.

40
4) Distribution within the body
Partition coefficient the relative affinity of a drug for either lipid or water environments determines how fast a drug will pass out of the gut, across barriers into the brain.

41
E.G., Heroin, (diacetylmorphine) is more soluble in lipid than is morphine, and thus penetrates into brain tissue more readily and a quicker onset of action ‑ Speed of entry into the brain is the basis of its euphoric effect.

42
4) Distribution within the body
Size and degree of ionization of a molecule effect its entry rate into the brain. Nicotine is a small, non-ionized molecule.

43
Effect of ionization on drug absorption
mq-fig jpg

44
4) Distribution within the body
Ionization factor ionization depends the properties of the drug, i.e.. How easily it is ionized by the solution it is in. This depends upon the pH of the solution. (pH is negative log of H+ ion concentration; e.g.. 10‑7m is moles/liter, the negative log is 7.0, pH is 7.0)
")
45
4) Distribution within the body
The extent of ionization of a drug is expressed as the pKa of the drug. pKa is equal to the pH of the aqueous solution in which the drug is 50% ionized. E.G., Weak acids ionize more readily in alkaline solutions, and weak bases ionize more readily in acidic solutions.

46
Effect of 50% ionization on drug absorption
mq-fig jpg

47
Principle of Ion Trapping
Drugs and their metabolites get trapped inside or outside of membranes and can not move across. This is due to the presence of an electric charge on the drug

48
Once a drug is “caught” outside of the blood, inside of the kidneys,
It is not re-absorbed and will be excreted with the urine.

49
Ionized drugs are transported out of the blood into the kidney compartment where the pH can vary due to what you’ve eaten recently. Ionized drugs carry a charge, this charge attracts water molecules and makes the drug “bigger” preventing it from getting back into the blood. mq-fig jpg Kidney

50
mq-fig jpg

51
4) Distribution within the body
Before getting to the brain, a drug must pass 2 barriers (1) plasma proteins and (2) blood‑brain barrier. They prevents drugs from diffusing out of the bloodstream.
 plasma proteins and (2) blood‑brain barrier. They prevents drugs from diffusing out of the bloodstream.")
52
The BBB is an obstacle for CNS therapy and a serious bottleneck in drug development for CNS diseases.

53
4) Distribution within the body
Blood‑brain barrier. Many drugs administered outside of the CNS are unable to enter the brain. The BBB is made up of many parts. Most important may be the peculiar type of capillaries that are in brain. Tight junctions, no fenestra, no pinocytosis, presence of thick basement membrane.

54
Blood-brain capillaries
mq-fig jpg

55
Astrocytic process (blue) cover the basement membrane (red)
 cover the basement membrane (red)")
56
The BBB is an obstacle for CNS therapy and a serious bottleneck in drug development for CNS diseases. Theoretically, the amount of randomly selected drugs having bioavailability in the CNS is less than 2% of small molecules and practically 0% of large molecules.

57
The BBB is an obstacle for CNS therapy and a serious bottleneck in drug development for CNS diseases. Theoretically, the amount of randomly selected drugs having bioavailability in the CNS is less than 2% of small molecules and practically 0% of large molecules. These numbers are also reflected by the drugs currently available for CNS diseases. Of over 7,000 potential drugs in the comprehensive medicinal chemistry database, only 5% can enter the brain.

58
The BBB is an obstacle for CNS therapy and a serious bottleneck in drug development for CNS diseases. Theoretically, the amount of randomly selected drugs having bioavailability in the CNS is less than 2% of small molecules and practically 0% of large molecules. These numbers are also reflected by the drugs currently available for CNS diseases. Of over 7,000 potential drugs in the comprehensive medicinal chemistry database, only 5% of all drugs treat the CNS. The typical CNS-active drug is very small in size with an average molecular mass of 0.36 kDa and is used for treatment of a very limited number of diseases, such as affective disorders, schizophrenia, epilepsy, and chronic pain.

59
Transport is carrier ‑ mediated. The BBB is selectively permeable.
4) Distribution into the brain Transport is carrier ‑ mediated. The BBB is selectively permeable. -- Reduces flow of water soluble or ionized molecules. -- Does not impede lipid‑soluble or un‑ionized molecules. The blood‑brain barrier is composed of a number of lipophylic elements. Therefore, drugs soluble in lipids enter the brain more easily than water-soluble drugs.
 Distribution into the brain. Transport is carrier ‑ mediated. The BBB is selectively permeable. -- Reduces flow of water soluble or ionized molecules. -- Does not impede lipid‑soluble or un‑ionized molecules. The blood‑brain barrier is composed of a number of lipophylic elements. Therefore, drugs soluble in lipids enter the brain more easily than water-soluble drugs.")
60
Astrocyte

62
Astrocytes are an important component of the blood brain barrier.

63
Astrocytes conduct nutrients and drugs from the blood to the neurons and transport waste products away to the blood and CSF.

64
The BBB is not intact everywhere.
Area postrema (vomiting center, projectile vomiting), # 9 in figure Also, the median eminence in the hypothalamus and the pineal gland
, # 9 in figure. Also, the median eminence in the hypothalamus and the pineal gland")
65
The blood‑brain barrier is not permeable to the neurotransmitters.
1) conserves transmitters within the nervous system 2) isolates brain from exogenously produced transmitter substances
 conserves transmitters within the nervous system. 2) isolates brain from exogenously produced transmitter substances.")
66
4) Distribution into the Brain out of the blood
Plasma Proteins The distribution of many drugs is slowed because they combine readily with proteins within the blood plasma. This prevents the drug from diffusing out of the bloodstream. An equilibrium is eventually reached between the unbound drug and the plasma protein drug complex. Drugs vary in their strength of binding to plasma proteins.

67
The elderly and people with impaired kidney or liver functions often have reduced levels of plasma proteins. As a result, there is less binding and the drug effects may be more intense.

68
Once a drug has entered the brain the site of action is at the synapse
5) Binding or localization in tissues Once a drug has entered the brain the site of action is at the synapse
 Binding or localization in tissues. Once a drug has entered the brain. the site of action is at the synapse.")
70
Within the synapse, the site of action is often a receptor protein.
A receptor is a physiological entity. The cells response to a drug is proportional to the number of receptors occupied = law of mass action. Receptors live on the surface of the neuron

71
Transmitter Receptor

72
5) Binding or localization in the Brain
Actions at Receptors Agonist: binds to receptors and produces pharmacological action. Antagonist: binds to receptors but produces no pharmacological action

73
Agonist and antagonist interactions with receptors
mq-fig jpg

74
mq-fig jpg

75
A drug binds to a receptor…Then what?
Intracellular action: promotes synthesis or release of an intracellular regulatory molecule - second messenger.

76
Cell Nucleus

77
A complex cascade of changes amplify the effects of the receptor within the neuron.

78
Regulation of receptors:
Desensitization - following continued stimulation of receptors. (Also called down regulation) Super sensitivity - following continued blockade of receptors or loss of neurotransmitters.
 Super sensitivity - following continued blockade of receptors or loss of neurotransmitters.")
79
Maximum Response is achieved when all receptors are fully occupied
Dose‑response at the receptor Describes the amount of pharmacological effect for a given concentration (dose). Maximum Response is achieved when all receptors are fully occupied
. Maximum Response is achieved when all receptors are fully occupied.")
80
Dose–response curve mq-fig jpg

81
Drug‑receptor Interactions
Potency determined by the affinity of drug for the receptor, as well as accessibility of drug to receptor site (which involves absorption, distribution, biotransformation, and excretion). Potency only determines the drug dose. Otherwise, not a particularly important issue.
. Potency only determines the drug dose. Otherwise, not a particularly important issue.")
82
Potency does not alter maximum effectiveness of drug
Potency does not alter maximum effectiveness of drug. Drugs of different potency that affect same receptor site will have same effect, simply give more drug. Potency does not correlate with clinical superiority.

83
Maximal efficacy: the maximal effect produced by a drug
Maximal efficacy: the maximal effect produced by a drug. Determined by drugs inherent properties, reflected as a plateau in dose-effect curve. Efficacy can be limited by undesired side effects that limit the amount or use of the drug, regardless of its efficacy. Efficacy and potency are not necessarily correlated - so don't confuse them

84
Therapeutic index Toxic dose for 50% of people/ effective dose for 50% of people. TD50/ED50.

85
Dose–response curves for four analgesic agents
mq-fig jpg

86
Comparison of ED50 and TD50 mq-fig jpg

87
Termination of drug effects:
Redistribution away from the site of action is one mechanism for terminating drug action. Most drugs are, however, metabolized within the liver and excreted by the kidneys. Metabolism may take place in the plasma, kidneys and other tissues, but most occur within the liver. Liver is the largest organ in the body and serves several functions besides metabolism. It has several different enzyme systems for metabolizing drugs.

88
mq-fig jpg

89
6) Biotransformation Primary effect of the metabolic process is to convert fat soluble substances into water soluble substances which are more easily excreted by the kidneys. Most common type of transformation is oxidation. Others include conjugation to a larger molecule which is water soluble. E.G., To glucuronide, gylcine, sulfate and acetyl groups. Oxidation by cytochrome p450 which is concentrated in the liver. Levels of p450 depend upon the need for this enzyme.

90
Only a few types of chemical transformations are actually involved.
Enormous diversity of drug types that exist. The liver does far more than convert active compounds into inactive ones that are more readily excreted. Some drugs are metabolized into more active substances E.G. Codeine - about 10% of administered codeine is metabolized to morphine which is much more powerful.

91
Certain pathological states can alter an individual's response to certain drugs.
E.G., Metabolic enzymes may be deficient in certain conditions. Infants -have a poorly develop glutathione system. Can't metabolize aspirin or Tylenol very well, so should alternate when given.

92
Some drugs influence the metabolism of other drugs.
E.G., By stimulating or inhibiting the oxidation system. In general, the more rapidly a drug is metabolized, the lower the blood levels and the smaller the drug effect. Occasionally, a non‑toxic drug may be metabolized by the liver into a carcinogenic compound. (hot dogs with sodium nitrite need ascorbic acid)
")
93
Primary excretory pathway is via the kidneys.
7) Excretion Drugs can be excreted in urine, feces, expired air, sweat, and the milk of a nursing mother. Primary excretory pathway is via the kidneys. Some drugs are excreted unchanged: E.G., Nitrous oxide via the lungs; E.G., The active agents in the hallucinogenic mushroom amanita muscaria via the kidneys -- common custom among users to collect the urine excreted by the people who have eaten the mushroom.
 Excretion. Drugs can be excreted in urine, feces, expired air, sweat, and the milk of a nursing mother. Primary excretory pathway is via the kidneys. Some drugs are excreted unchanged: E.G., Nitrous oxide via the lungs; E.G., The active agents in the hallucinogenic mushroom amanita muscaria via the kidneys -- common custom among users to collect the urine excreted by the people who have eaten the mushroom.")
94
The rate at which a substance is excreted is pH dependent.
-- Drugs that are basic are excreted most rapidly when the urine is acidic, whereas acidic drugs are excreted faster when the urine is alkaline. E.G., Cigarette smokers may regulate their nicotine intake via their food consumption. Increased excretion of nicotine leads to increased cigarette smoking. Since nicotine is excreted more slowly when the urine is alkaline (nicotine is basic). Smokers who take extra vitamin C smoke more than those who take bicarbonates for GI distress.
. Smokers who take extra vitamin C smoke more than those who take bicarbonates for GI distress.")
95
Eating also effects urinary pH
Eating also effects urinary pH. The urine becomes more acidic about 30 minutes after eating, then grows more alkaline for hours. Smokers routinely light up after meals as their nicotine levels are reduced by the acidified urine. Therefore, if you want to quit smoking and not feel the effects of low nicotine in your blood system, it helps if you take low doses of sodium bicarbonate. (...and stop eating)
")
96
Heavy breathing also blows off CO2 and increases blood pH.
This accelerates the removal of nicotine from the brain. Three blood pH buffers. Plasma proteins, hemoglobin and carbonic acid : HCO3- + H+ <=> H2CO3 <=> CO2 + H2O loosing CO2 moves equation to the right and lowers H+ ion concentration, pH increases.

97
7) Excretion Excretion rate is given as half-life of drug in body – The time required for body to reduce plasma concentration by half.
 Excretion Excretion rate is given as half-life of drug in body – The time required for body to reduce plasma concentration by half.")
98
7) Excretion mq-fig jpg
 Excretion mq-fig jpg")
99
mq-table jpg

100
Rebound Effects The withdrawal of drugs that modify physiological or behavioral systems is often accompanied by changes in the opposite direction of the original compound. The always brain pushes back. E.G. The euphoria induced by cocaine and amphetamine is often a prelude to severe depression. E.G. Alcohol and barbiturates suppress dreaming and REM sleep and also reduce the vividness of dreams. During withdrawal, dream time and vividness of the dreams are increased.

101
Responsiveness to Drugs:
4 Important Influences Our response to drugs is influenced not only by our metabolism of them, but also our compliance with the prescriptions as written by the physician. However, there are 4 important factors which influence responsiveness to drugs that are important for compounds which have behavioral effects.

102
First Organismic Factor is Age
Children are often hyperactive to drugs because of incomplete development of metabolic enzyme systems. Older people may be hyperactive because of impaired metabolic excretory mechanisms. In some young species, there may also be an undeveloped blood‑brain barrier.

103
According to US government: 120,000 older people are afflicted annually by mental impairment induced by psychoactive drugs given to them by their physician. 32,000 fall and break hips because they are dizzy from prescription tranquilizers and sleeping pills. According to the inspector general Richard Kusserow of the US Health & Human Services Dept. At least 200,000 elderly are hospitalized each year because of the drugs they take!! Older people also take a greater number of drugs

104
Second Organismic Factor is Weight
Dose must be adjusted to the weight of the drug recipient. This is usually calculated on the basis on the number of milligrams of drug/kg of body wt.

105
Third Organismic Factor is Biological Rhythms
Physiological systems undergo rhythmic variations and activity. This is true in single cell organisms. Responsiveness to drugs is rhythmic in nature. Humans that are on a typical 24 hour schedule where they sleep between midnight and 8 am are maximally susceptible to drugs between the hours of 9:30 and 11:30 in the evening. I.E., A dose which that is effective or non‑toxic in the morning, could be lethal if given during the evening.

106
Fourth Factor Is Personality
Many personality variables effect responsiveness to drugs. This argument was best described by Wilder in his law of initial value. Each person has an initial level of excitation; the degree of response depends upon this initial level. E.G., euphoria is observed in patients suffering from pain, anxiety, or tension when they are given small doses of morphine.

107
A similar dose given to a happy, pain‑free individual often precipitates mild anxiety and fear.
Stuporous catatonic patients often respond with a burst of animation and spontaneity to intravenous injections of barbiturates. Finally, sedative drugs create more anxiety in outgoing, athletic people, as compared to passive intellectual types.

108
The tendency is that people who respond strongly to one drug tend to respond strongly to others.
Response of patient is also affected by importance of symptom being treated. Treatment of trivial symptoms of syndrome may be worse than not treating the patient.

109
Physiological state: pathological and physiological conditions modify drug actions. Alterations in renal or hepatic functioning are likely to have an effect as well as our vitamin deficiencies. However, even normal alterations of physiological function influence drug activity. Examples are as follows. Aspirin lowers body temperature in febrile individuals, but does not effect body temperature when it is normal.

110
The toxicity of both caffeine and amphetamine is increased in mice when they have been deprived of water. Respiratory depression that is produced by morphine is reduced by pain, so much so, that pain is often inflicted on victims of morphine overdose as a therapy, at which time it acts as an antidote to morphine in the same way that during pain morphine is an antidote to the pain.

111
Genetics: different strains of mice metabolize drugs at different rates.
There is also an obvious sex difference in metabolism of compounds. Morphine controls pain much better in men than women. Ibuprofen is more effective in men than women. Anti-rejection drugs are cleared from women faster so they reject more organs than men. Sometimes, certain individuals may possess a genetic complement which will have tragic consequences under normal conditions. E.G., A case of a young boy who died after receiving general anesthetic. When his sister subsequently required an operation, she was given the same anesthetic and also died.

112
Drug variables A very important drug variable is the (1) dose response curve. Many compounds have vastly different effects when administered at different concentrations. E.G., Although barbiturates are effective for inducing sleep, small doses induce excitement and increase sensitivity to pain. Repeated administrations of the same drugs. If a drug is administered chronically in doses that exceed the amount removed from the body by metabolism and excretion, cumulative effects can occur.

113
Tolerance may also develop with many drugs.
Tolerance is the progressive requirement with chronic use for higher drug doses to produce a given effect. Tolerance can be viewed as an attempt by the body to return to homeostasis, equivalent to the drug free condition. Cross tolerance- develops among related drugs. E.G. between mescaline and LSD. (The reverse is also true.)
")
114
mq-table jpg

115
Sensitization - when responsiveness to a drug increases with repeated administrations.
E.G. Marijuana, amphetamine, cocaine, barbiturates, and morphine.

116
Withdrawal: the abstinence syndrome.
Set of behaviors and physiologic symptoms that occur when drug treatment is withdrawn from a person who has developed a tolerance to the drug.

117
Psychological Dependence:
Physical Dependence: Craving for substances as a result of pharmacodynamic tolerance. (Neurochemical adjustment of brain to presence of drug.) Physical dependence is defined as an adaptive state that manifests itself by intense physical disturbances when the administration of a drug is suspended. Psychological Dependence: Psychological dependence is defined as a condition in which a drug produces a feeling of satisfaction and a psychic drive that requires periodic or continuous administration of the drug to reduce pleasure or to avoid discomfort.
 Physical dependence is defined as an adaptive state that manifests itself by intense physical disturbances when the administration of a drug is suspended. Psychological Dependence: Psychological dependence is defined as a condition in which a drug produces a feeling of satisfaction and a psychic drive that requires periodic or continuous administration of the drug to reduce pleasure or to avoid discomfort.")
118
Physical and psychological dependence is typically called addiction
Physical and psychological dependence is typically called addiction. Over time these effects can have cumulative negative effects on physiology and general health related to changes in lifestyle and diet and due to legality of the drug being used. Why do you think the appearance of these people changed so much?

119
Bioavailability Refers to the effectiveness with which a drug is absorbed. All preparations that contain identical amounts of active ingredients are not equally utilized. Bioavailability depends significantly upon the manufacturer of a drug. (Remember: 250 ingredients with 200,000 variations)
")
121
Dosage Regimen To maintain a steady state level of a drug, administration should be at uniform intervals equal to the drug's biological half life. Drug levels that are too low will be ineffective while those that are too high may be toxic. E.G. A drug with a half life of 8 hours should be given at 8 hour intervals.

122
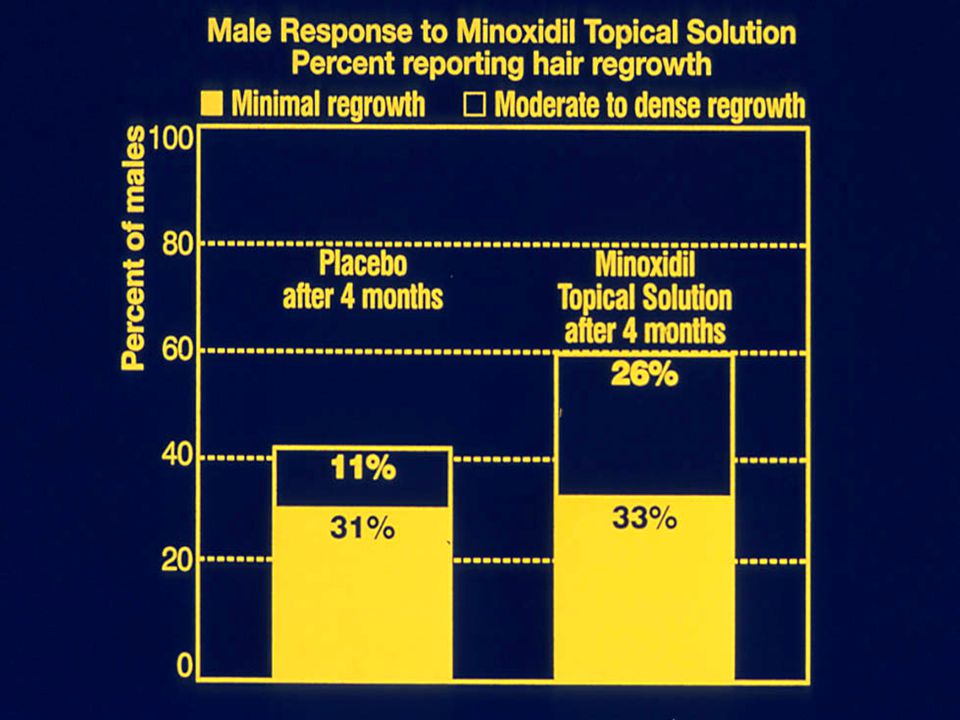
Expectation plays an important role in how we respond to drugs that affect the brain: We call this…
THE PLACEBO EFFECT

127
The Placebo Effect Size and Color are Important

128
Placebo Effect Placebos play an important part in medical practice. Placebo effect may have greater implications for psychotherapy than any other form of treatment because both psychotherapy and the placebo effect function primarily through psychological mechanisms. Placebos influence both selective and objective measures. E.G., Study of patients with bleeding ulcers: half were told by a doctor that they were given a new drug which would undoubtedly produce relief; The other half was told by nurses that they would receive a new experimental drug with uncertain effects. In fact, both groups received a placebo.

129
The dopamine being released leads to reduced binding of the radioactive drug to the dopamine receptors in the caudate nucleus. Treatment with placebo increased the release of dopamine and decreased the number of dopamine receptors within the caudate nucleus of patients with Parkinson’s Disease. de la Fuente-Fernandez et al.,2001.

130
Placebo effects depend in part on the condition that’s being treated.
Placebo doesn’t affect diabetes; there’s no placebo effect on blood sugar levels. Pain reducing placebo seems to be about half of the response to active pain reducing medications. This is true regardless of whether the active medication is aspirin or morphine, meaning that placebo morphine is significantly more powerful than placebo aspirin. For depression the placebo response ranges from 60 to 80 percent of the response to the medication. Placebo effects occur faster than “real” drug effects!

131
Figure 1. Areas in which the magnitude of placebo analgesia correlated with gray matter density
Schweinhardt, P. et al. J. Neurosci. 2009;29: Copyright ©2009 Society for Neuroscience

132
Figure 2. Areas in which the dopamine-related trait variable correlated significantly with gray matter density Schweinhardt, P. et al. J. Neurosci. 2009;29: Copyright ©2009 Society for Neuroscience

133
NIH Press Release May 2002 Placebo, Antidepressant May Lift Depression Via Common Mechanism Both groups, placebo (top) and drug (bottom) shared a pattern of increased activity in the cortex (e.g., prefrontal, posterior cingulate) and decreased activity in limbic regions (e.g., subgenual cingulate), which the researchers suggest is necessary for therapeutic response.
 and drug (bottom) shared a pattern of increased activity in the cortex (e.g., prefrontal, posterior cingulate) and decreased activity in limbic regions (e.g., subgenual cingulate), which the researchers suggest is necessary for therapeutic response.")
134
Participants viewed images taken from paintings either of a woman depicted by Leonardo da Vinci, left, or of the Virgin Mary, right, before and during applications of painful electrical pulses. Devout Catholics reported feeling peaceful and secure, as well as thinking about compassion and other religious concepts, while viewing the Virgin Mary. They rated that image as especially helpful in coping with pain. Non-religious participants reported no advantage from either image in dealing with pain. Pain relief for Catholics was accompanied by activity in the right ventrolateral prefrontal cortex, a brain region linked to pain relief associated with emotional detachment and perceived control over pain. This brain response was not observed in the non-religious volunteers. Wiech, K., et al. In press. An fMRI study measuring analgesia enhanced by religion as a belief system. Pain.2008

135
"cure for Dyspepsia, Low Spirits, Nervousness, Heartburn, Colic Pains, Wind in the Stomach or Pains in the Bowels, Headache, Drowsiness, Kidney and Liver Complaints, Melancholy, Delirium Tremens, and Intemperance."

137
Next: Acetylcholine

Similar presentations










 drugs to polar metabolites easily excreted in urine. The liver.>")
 Potential for abuse Accepted medical.>")
 Absorption Distribution Metabolism Excretion Toxicology.>")


 Oral Administration - substance is ingested through the mouth - digested and absorbed in gastrointestinal tract - passes through.>")










