Download presentation
Presentation is loading. Please wait.

1
Anxiety, Obsessive-compulsive, and Post-traumatic Stress Disorders
Chapter 6 Anxiety, Obsessive-compulsive, and Post-traumatic Stress Disorders

2
Anxiety: the unpleasant feeling of fear and apprehension
Anxiety Disorders Anxiety: the unpleasant feeling of fear and apprehension Anxiety has two major components: the physiological the heightened level of arousal and physiological activation the cognitive the subjective perception of the anxious arousal and the associated cognitive processes: worry and rumination.

3
Anxiety disorders tend to be comorbid
Anxiety tends to be future-focused The emphasis is on things that could happen. The negative reinforcement problem Anxiety and worry can be reinforced by the avoidance of feared outcomes and possible experiences that never happen. Anxiety disorders tend to be comorbid The most common psychological disorders in Canada (2006)
")
4
When does anxiety become a problem?
The anxiety must be chronic, relatively intense, associated with role impairment, and causing significant distress for self or others. there is a subjective element to the diagnosis What tends to distinguish chronically anxious people is their propensity to perceive threat and to be concerned/worried when there is no objective threat or the situation is ambiguous

5
Prevalence of anxiety disorders
Anxiety disorders are the most common psychological disorders A majority of Canadians who met criteria for an anxiety disorder report that it interfered with their home, school, work, and social life (Government of Canada, 2006). According to the Ontario Mental Health Supplement study (Ontario Ministry of Health, 1994), a clear gender difference exists, with 16% of women and 9% of men having suffered from anxiety disorders in the preceding year. The highest one-year prevalence rates (i.e., almost 1 in 5) were found in women 15 to 24 years of age. Anxiety disorders were more common in women than in men across all age groups. Similar results were found in 15 countries around the world (see Seedat et al., 2009).
. According to the Ontario Mental Health Supplement study (Ontario Ministry of Health, 1994), a clear gender difference exists, with 16% of women and 9% of men having suffered from anxiety disorders in the preceding year. The highest one-year prevalence rates (i.e., almost 1 in 5) were found in women 15 to 24 years of age. Anxiety disorders were more common in women than in men across all age groups. Similar results were found in 15 countries around the world (see Seedat et al., 2009).")
6
International Prevalence
Somers, Goldner, Waraich, and Hsu (2006) pooled the results of 41 international epidemiological studies: one-year prevalence: 10.6% lifetime prevalence: 16.6% These disorders have an early age of onset, typically during childhood.
 pooled the results of 41 international epidemiological studies: one-year prevalence: 10.6% lifetime prevalence: 16.6% These disorders have an early age of onset, typically during childhood.")
7
U.S. Prevalence Kessler et al. (2012) surveyed existing U.S. data lifetime morbid risk (LMR) major depressive episode (29.9%) specific phobia (18.4%) social phobia (13.0%) post- traumatic stress disorder (10.1%) generalized anxiety disorder (9.0%) separation anxiety disorder (8.7%) panic disorder (6.8%) one-year prevalence specific phobia (12.1%), Major depressive episode (8.6%) social phobia (7.4%). The two disorders with the earliest median age of onset (15–17 years old) were phobias and separation anxiety.
 social phobia (13.0%) post- traumatic stress disorder (10.1%) generalized anxiety disorder (9.0%) separation anxiety disorder (8.7%) panic disorder (6.8%) one-year prevalence. specific phobia (12.1%), Major depressive episode (8.6%) social phobia (7.4%). The two disorders with the earliest median age of onset (15–17 years old) were phobias and separation anxiety.")
8
Summary of Major Anxiety Disorders
Description Phobia Fear and avoidance of objects or situations that do not present any real danger. Panic Disorder Recurrent panic attacks involving a sudden onset of physiological symptoms, such as dizziness, rapid heart rate, and trembling, accompanied by terror and feelings of impending doom; sometimes accompanied with agoraphobia, a fear of being in public places. Generalized Anxiety Disorder Persistent, uncontrollable worry, often about minor things. Separation anxiety The anxious arousal and worry about losing contact with and proximity to other people, typically significant others.

9
Changes in DSM-5 Post-Traumatic Stress Disorder (PTSD) is now recognized in DSM-5 as a stress disorder Obsessive-Compulsive Disorder (OCD) is now classified under “Obsessive-Compulsive and Related Disorders”
 is now classified under Obsessive-Compulsive and Related Disorders")
10
Separation Anxiety Separation anxiety is the anxiety that results from not having contact or the possibility of losing contact with attachment figures. It is seen generally as a type of anxiety that is prevalent among children of various ages but not relevant among older people.

11
Adult Separation Anxiety
There is a growing focus on separation anxiety disorder in adults. adults who cannot stand to be alone and are cognitively preoccupied with losing contact with loved ones It is intriguing that in a recent study conducted with 520 patients from an anxiety disorders clinic in Australia, the separation anxiety disorder diagnosis was the most prevalent when all anxiety disorder diagnoses were considered; in fact, almost 1 in 4 adult patients were diagnosed with an adult form of separation anxiety disorder (Silove et al., 2010). These data suggest that the separation anxiety disorder diagnosis in adults deserves much more consideration than it currently receives.
. These data suggest that the separation anxiety disorder diagnosis in adults deserves much more consideration than it currently receives.")
12
Phobias Phobia—disrupting, fear-mediated avoidance that is out of proportion to the danger actually posed and is recognized by the sufferer as groundless Many specific fears do not cause enough hardship to compel an individual to seek treatment. an urban dweller with an intense fear of snakes will probably have little direct contact with the feared object and may therefore not believe that anything is seriously wrong. The term “phobia” usually implies that the person suffers intense distress and social or occupational impairment because of the anxiety.

13
Naming Phobias For phobias the suffix phobia is preceded by a Greek word for the feared object or situation. The suffix is derived from the name of the Greek god Phobos, who frightened his enemies. Claustrophobia , fear of closed spaces agoraphobia , fear of public places acrophobia , fear of heights ergasiophobia , fear of working Pnigophobia, fear of choking taphephobia , fear of being buried alive mysophobia , the fear of contamination and dirt

14
Is there precision in treating phobias?
These authoritative terms convey the impression that we understand how a particular problem originated and how it can be treated. As with so much in the field of abnormal psychology, there are more theories and jargon pertaining to phobias than there are firm findings.

15
Changing Phobias New phobias tend to emerge in keeping with societal changes. nomophobia a pathological fear of remaining out of touch with technology that is experienced by people who have become overly dependent on using their mobile phones (nomophobia meaning no mobile phone phobia) or personal computers.
 or personal computers.")
16
Phobias Considered From Different Paradigms
Psychoanalysts focus on the content of the phobia and see the phobic object as a symbol of an important unconscious fear. the content of phobias has important symbolic value. Behaviourists focus on the function of phobias.

17
Specific Phobias Specific phobias— unwarranted fears caused by the presence or anticipation of a specific object or situation Evidence to support the grouping of fears into five factors: Agoraphobia Fears of heights or water Threat fears (e.g., blood/needles, storms/thunder) Fears of being observed Speaking fears These fears reflect two higher-order categories: specific fears and social fears.
 Fears of being observed. Speaking fears. These fears reflect two higher-order categories: specific fears and social fears.")
18
Specific Phobias Specific phobias tend to be long-lasting
mean duration of 20 years only 8% of people with a specific phobia received treatment. The most common specific phobia subtypes in order were: (1) animal phobias (including insects, snakes, and birds); (2) heights; (3) being in closed spaces; (4) flying; (5) being in or on water; (6) going to the dentist; (7) seeing blood or getting an injection; (8) storms, thunder, or lightning.
 animal phobias (including insects, snakes, and birds); (2) heights; (3) being in closed spaces; (4) flying; (5) being in or on water; (6) going to the dentist; (7) seeing blood or getting an injection; (8) storms, thunder, or lightning.")
19
Specific Phobias: Culture
The specific fear focused on in a phobia can vary cross culturally. China: Pa-leng (a fear of the cold) worries that loss of body heat may be life-threatening. This fear appears to be related to the Chinese philosophy of yin and yang: yin refers to the cold, windy, energy-sapping, and passive aspects of life, while yang refers to hot, powerful, and active aspects. Japan: taijin kyofusho (TKS), fear of other people. it is an extreme fear of embarrassing others—for example, by blushing in their presence, glancing at their genital areas, or making odd faces. It is believed that this phobia arises from elements of traditional Japanese culture, which encourages extreme concern for the feelings of others yet discourages direct communication of feelings (McNally, 1997).
 worries that loss of body heat may be life-threatening. This fear appears to be related to the Chinese philosophy of yin and yang: yin refers to the cold, windy, energy-sapping, and passive aspects of life, while yang refers to hot, powerful, and active aspects. Japan: taijin kyofusho (TKS), fear of other people. it is an extreme fear of embarrassing others—for example, by blushing in their presence, glancing at their genital areas, or making odd faces. It is believed that this phobia arises from elements of traditional Japanese culture, which encourages extreme concern for the feelings of others yet discourages direct communication of feelings (McNally, 1997).")
20
Social Phobia or Social Anxiety Disorder
Social phobias— persistent, irrational fears linked generally to the presence of other people. People with a social phobias try to avoid situations in which they might be evaluated because they fear that they will reveal signs of anxiousness or behave in an embarrassing way Examples: Speaking or performing in public Eating in public Using public lavatories

21
Social Phobia or Social Anxiety Disorder (cont.)
Social phobias can be either generalized or specific Generalized Social Phobia involve many different interpersonal situations an earlier age of onset often comorbid with other disorders such as depression and alcohol use more severe impairment than specific phobia Specific SP involve intense fear of one particular situation (e.g., public speaking). Lifetime prevalence in Canada 7.5% in men 8.7% in women DSM-5 SAD criteria were modified to allow for a performance only specifier.
. Lifetime prevalence in Canada. 7.5% in men. 8.7% in women. DSM-5 SAD criteria were modified to allow for a performance only specifier.")
22
Social Phobia or Social Anxiety Disorder: Onset and Duration
Onset generally takes place during adolescence The lifetime prevalence of social phobia in the CCHS 1.2 was 7.5% in men and 8.7% in women. The average age of onset was 13 years and average duration of symptoms was 20 years (see Stansfeld et al., 2008). The prevalence of social phobia was higher among people who had never married or were divorced, had not completed secondary education, had lower income or were unemployed, reported lacking adequate social support, reported low quality of life, or had a chronic physical condition (see Stansfeld et al., 2008).
. The prevalence of social phobia was higher among people who had never married or were divorced, had not completed secondary education, had lower income or were unemployed, reported lacking adequate social support, reported low quality of life, or had a chronic physical condition (see Stansfeld et al., 2008).")
23
Aetiology of Phobias Behavioural Theories Focus on learning
Avoidance Conditioning — reactions are learned avoidance responses Phobias develop from two related sets of learning: 1. Via classical conditioning 2. Person learns to reduce conditioned fear by escaping from or avoiding the CS (operant conditioning)
")
24
Behavioural Theories (cont.)
Modelling person can learn fear through imitating the reactions of others (vicarious learning). Prepared Learning Some fears may reflect classical conditioning, but only to stimuli to which an organism is physiologically prepared to be sensitive People fear spiders, snakes, and heights but not lambs Is a diathesis needed? Cognitive diathesis such as the tendency to believe that similar traumatic experiences will occur in the future or not being able to control the environment may be important in developing a phobia.
. Prepared Learning. Some fears may reflect classical conditioning, but only to stimuli to which an organism is physiologically prepared to be sensitive. People fear spiders, snakes, and heights but not lambs. Is a diathesis needed Cognitive diathesis such as the tendency to believe that similar traumatic experiences will occur in the future or not being able to control the environment may be important in developing a phobia.")
25
Behavioural Theories (cont.)
Social Skills Deficits in Social Phobias Inappropriate behaviour or a lack of social skills the cause of social anxiety The individual has not learned how to behave so that he or she feels comfortable with others or the person repeatedly commits faux pas, is awkward and socially inept, and is often criticized by social companions. Socially anxious people are indeed rated as being low in social skills (Twentyman & McFall, 1975) The timing and placement of socially anxious responses in a social interaction, such as saying thank you at the right time and place, are impaired (Fischetti, Curran, & Wessberg, 1977).
 The timing and placement of socially anxious responses in a social interaction, such as saying thank you at the right time and place, are impaired (Fischetti, Curran, & Wessberg, 1977).")
26
Aetiology of Phobia (cont.)
Cognitive Theories Focus on how people’s thought processes can serve as a diathesis and on how thoughts can maintain a phobia Anxiety is related to being more likely to: Attend to negative stimuli Interpret ambiguous information as threatening Believe that negative events are more likely than positive ones to re-occur

27
Social Anxiety Socially anxious people are:
more concerned about evaluation than are people who are not socially anxious (Goldfried, Padawer, & Robins, 1984) are highly aware of the image they present to others (Bates, 1990) high in public self-consciousness preoccupied with a need to seem perfect and not make mistakes in front of other people (Flett, Coulter, & Hewitt, 2012; Hewitt et al., 2003). tend to view themselves negatively even when they have actually performed well in a social interaction (Wallace & Alden, 1997) are less certain about their positive self-views relative to people without social phobia, they see their positive attributes as being less important (Moscovitch et al., 2009).
 are highly aware of the image they present to others (Bates, 1990) high in public self-consciousness. preoccupied with a need to seem perfect and not make mistakes in front of other people (Flett, Coulter, & Hewitt, 2012; Hewitt et al., 2003). tend to view themselves negatively even when they have actually performed well in a social interaction (Wallace & Alden, 1997) are less certain about their positive self-views. relative to people without social phobia, they see their positive attributes as being less important (Moscovitch et al., 2009).")
28
Aetiology of Phobia (cont.)
Cognitive-behavioural models of social phobia link social phobia to certain cognitive characteristics: Attentional bias to focus on negative social information Perfectionistic standards for accepted social performances High degree of public self-consciousness People with social phobia have a tendency to interpret ambiguous social situations as negative and a reflection of their personal shortcomings, they also have a memory bias linked to this interpretation bias (Hertel, Brozovich, Joormann, & Gotlib, 2008).
.")
29
Cognitive-behavioural models of social phobia
David Moscovitch (2009) concluded that the fundamental core thematic fear in social phobia is “the self is deficient.” Moscovitch maintains that the key situational triggers are those situations and circumstances that will publicly reveal the self as inadequate. Related research has shown that social phobia is linked with excessive self-criticism (Cox, Walker, Enns, & Karpinski, 2002).
 concluded that the fundamental core thematic fear in social phobia is the self is deficient. Moscovitch maintains that the key situational triggers are those situations and circumstances that will publicly reveal the self as inadequate. Related research has shown that social phobia is linked with excessive self-criticism (Cox, Walker, Enns, & Karpinski, 2002).")
30
Post-event Processing (PEP) of negative social experiences
a form of rumination about previous experiences and responses to these situations, especially experiences involving other people that did not turn out well. There is a link between social anxiety and PEP.

31
Aetiology of Phobia (cont.)
Predisposing Biological Factors People with specific phobia, PTSD, and SAD, relative to comparison subjects, have greater activity in two areas associated with negative emotional responses: the amygdala and the insula (Etkin & Wager, 2007). 1. Autonomic Nervous System Lacey (1967): stability-lability. Labile, or jumpy, individuals are those whose autonomic systems are readily aroused by a wide range of stimuli. Because of the extent to which the autonomic nervous system is involved in fear and hence in phobic behaviour, a dimension such as autonomic lability assumes considerable importance. Since there is reason to believe that autonomic lability is to some degree genetically determined (Gabbay, 1992), heredity may very well have a significant role in the development of phobias.
. 1. Autonomic Nervous System. Lacey (1967): stability-lability. Labile, or jumpy, individuals are those whose autonomic systems are readily aroused by a wide range of stimuli. Because of the extent to which the autonomic nervous system is involved in fear and hence in phobic behaviour, a dimension such as autonomic lability assumes considerable importance. Since there is reason to believe that autonomic lability is to some degree genetically determined (Gabbay, 1992), heredity may very well have a significant role in the development of phobias.")
32
Predisposing Biological Factors
Genetic factors Jerome Kagan has focused on the trait of behavioural inhibition or shyness (Kagan, 1997). Some infants as young as four months become agitated and cry when they are shown toys or other stimuli. This behaviour pattern, which may be inherited, may set the stage for the later development of phobias. no specific susceptibility genes have been found thus far.
. Some infants as young as four months become agitated and cry when they are shown toys or other stimuli. This behaviour pattern, which may be inherited, may set the stage for the later development of phobias. no specific susceptibility genes have been found thus far.")
33
Aetiology of Phobias (cont.)
Psychoanalytic Theory Phobias are a defence against the anxiety produced by repressed id impulses anxiety is displaced from the feared id impulse and moved to an object or situation that has some symbolic connection to it. These objects or situations then become the phobic stimuli. By avoiding them the person is able to avoid dealing with repressed conflicts.

34
Panic Disorder Panic Attack—person suffers a sudden and often inexplicable attack of alarming symptoms: Laboured breathing, heart palpitations, Nausea and chest pain; Feelings of Choking and smothering; Dizziness, sweating, and trembling; Intense apprehension, terror, and feelings of impending doom. May also experience depersonalization (a feeling of being outside one ’s body) and derealization (a feeling of the world ’s not being real, as well as fears of losing control, of going crazy, or even of dying).
 and derealization (a feeling of the world ’s not being real, as well as fears of losing control, of going crazy, or even of dying).")
35
Panic Disorder (cont.) Other features of panic attacks:
may occur frequently May be situationally predisposed May be uncued Panic attacks can also occur in seemingly benign states, such as relaxation or sleep, and in unexpected situations Recurrent uncued attacks and worry about having attacks in the future are required for the diagnosis of panic disorder. The exclusive presence of cued attacks most likely reflects the presence of a phobia.

36
Prevalence: Panic Disorder
Among Canadians. The 12-month prevalence of panic attacks was 6.4%. Panic attacks were related to numerous psychological and physical function variables, including poor overall functioning, suicidal ideation, psychological distress, activity restriction, chronic physical conditions, and self-rated physical and mental health (Kinley et al., 2009). The authors concluded that panic attacks may be a marker of severe psychopathology independent of a diagnosis of panic disorder. Among the Inuit of Northern Canada and west Greenland, kayak-angst occurs among seal hunters who are alone at sea. Attacks involve intense fear, disorientation, and concerns about drowning.
. The authors concluded that panic attacks may be a marker of severe psychopathology independent of a diagnosis of panic disorder. Among the Inuit of Northern Canada and west Greenland, kayak-angst occurs among seal hunters who are alone at sea. Attacks involve intense fear, disorientation, and concerns about drowning.")
37
Agoraphobia Panic disorder is diagnosed as with or without agoraphobia Agoraphobia (from the Greek agora, meaning “marketplace”) is a cluster of fears centring on public places and being unable to escape or find help should one become incapacitated. Fears of shopping, crowds, and travelling are often present. Many people with agoraphobia are unable to leave the house or do so only with great distress
 is a cluster of fears centring on public places and being unable to escape or find help should one become incapacitated. Fears of shopping, crowds, and travelling are often present. Many people with agoraphobia are unable to leave the house or do so only with great distress.")
38
Panic Disorder People who have panic disorder typically avoid the situations in which a panic attack could be dangerous or embarrassing. If the avoidance becomes widespread, panic with agoraphobia is the result. Panic disorder with agoraphobia and agoraphobia without a history of panic disorder are both much more common among women than among men.

39
Aetiology of Panic Disorder
Biological Theories Mitral valve prolapse syndrome Inner ear disease causes dizziness Panic disorder runs in families and has greater concordance in identical-twin pairs than in fraternal twins (Smoller et al., 2008). An increased risk of 5–16% among relatives of those with panic disorder. Early onset of panic disorder is associated with increased risk for family members. May be linked to “Val158Met COMT polymorphism” or other loci within or near the COMT gene (on chromosome 22)
. An increased risk of 5–16% among relatives of those with panic disorder. Early onset of panic disorder is associated with increased risk for family members. May be linked to Val158Met COMT polymorphism or other loci within or near the COMT gene (on chromosome 22)")
40
Aetiology of Panic Disorder (cont.)
Noradrenergic activity theory Panic is caused by overactivity in the noradrenergic system Stimulation of the locus ceruleus causes monkeys to have “panic attack” in humans yohimbine (drug that stimulates activity in the locus ceruleus) can elicit panic attacks Drugs that block firing in the locus ceruleus have not been found to be very effective in treating panic attacks (McNally, 1994). Problem in gamma-aminobutyric acid (GABA) GABA generally inhibit noradrenergic activity Positron emission tomography study found fewer GABA- receptor binding sites in people with PD therapeutic improvement involves changes in GABA receptors, but this applies to both anxiety and depression (Mohler, 2012).
 can elicit panic attacks. Drugs that block firing in the locus ceruleus have not been found to be very effective in treating panic attacks (McNally, 1994). Problem in gamma-aminobutyric acid (GABA) GABA generally inhibit noradrenergic activity. Positron emission tomography study found fewer GABA- receptor binding sites in people with PD. therapeutic improvement involves changes in GABA receptors, but this applies to both anxiety and depression (Mohler, 2012).")
41
Aetiology of Panic Disorder (cont.)
Cholecystokinin (CCK) Peptide that occurs in the cerebral cortex, amygdala, hippocampus, and brain stem, induces anxiety-like symptoms in rats and effect can be blocked with benzodiazepines Bradwejn hypothesized that panic disorder is, at least in part, due to hypersensitivity to CCK Exposure to CCK-4 induces panic attacks and patients with panic disorder have a clear sensitivity to CCK-4. There is genetic basis to CCK-4 and its role in panic disorder (Zwanzger et al., 2012).
 Peptide that occurs in the cerebral cortex, amygdala, hippocampus, and brain stem, induces anxiety-like symptoms in rats and effect can be blocked with benzodiazepines. Bradwejn hypothesized that panic disorder is, at least in part, due to hypersensitivity to CCK. Exposure to CCK-4 induces panic attacks and patients with panic disorder have a clear sensitivity to CCK-4. There is genetic basis to CCK-4 and its role in panic disorder (Zwanzger et al., 2012).")
42
Aetiology of Panic Disorder (cont.)
Psychological Theories The fear-of-fear hypothesis Suggests that agoraphobia is not a fear of public places per se, but a fear of having a panic attack in public. Misinterpretation of physiological arousal symptoms an ANS that is predisposed to be overly active (Barlow, 1988) coupled with a psychological tendency to become very upset by these sensations.
 coupled with a psychological tendency to become very upset by these sensations.")
43
A Vicious Circle: Panic Attacks
When high physiological arousal occurs, some people construe these unusual autonomic reactions (such as rapid heart rate) as a sign of great danger or even as a sign that they are dying. After repeated occurrences, the person comes to fear having these internal sensations and, by worrying excessively, makes them worse and panic attacks more likely. Thus, the psychology of the person takes over from where the biology began. The person becomes more vigilant about even subtle signs of an impending panic attack, and this, too, makes an attack more probable. The result is a vicious circle: fearing another panic attack leads to increased autonomic activity; symptoms of this activity are interpreted in catastrophic ways; and these interpretations in turn raise the anxiety level, which eventually blossoms into a full-blown panic attack (Craske & Barlow, 1993).
 as a sign of great danger or even as a sign that they are dying. After repeated occurrences, the person comes to fear having these internal sensations and, by worrying excessively, makes them worse and panic attacks more likely. Thus, the psychology of the person takes over from where the biology began. The person becomes more vigilant about even subtle signs of an impending panic attack, and this, too, makes an attack more probable. The result is a vicious circle: fearing another panic attack leads to increased autonomic activity; symptoms of this activity are interpreted in catastrophic ways; and these interpretations in turn raise the anxiety level, which eventually blossoms into a full-blown panic attack (Craske & Barlow, 1993).")
44
Anxiety Sensitivity There is converging evidence that anxiety sensitivity acts as a risk factor for anxiety psychopathology (see Schmidt, Zvolensky, & Maner, 2006, for review). Anxiety sensitivity predicts the development of spontaneous panic attacks. More importantly, independent of a history of anxiety problems and baseline trait anxiety, anxiety sensitivity predicted the development of anxiety diagnoses and overall Axis I clinical diagnoses, including anxiety, mood, and alcohol-use disorders.
. Anxiety sensitivity predicts the development of spontaneous panic attacks. More importantly, independent of a history of anxiety problems and baseline trait anxiety, anxiety sensitivity predicted the development of anxiety diagnoses and overall Axis I clinical diagnoses, including anxiety, mood, and alcohol-use disorders.")
45
Generalized Anxiety Disorder (GAD)
People with GAD are persistently anxious and often about minor items. Chronic, uncontrollable worry about everything Most frequent worries concern their health and the hassles of daily life

46
Generalized Anxiety Disorder (GAD)
Other features include: Difficulty concentrating, Tiring easily, restlessness, Irritability, A high level of muscle tension People with GAD do not typically seek psychological treatment GAD typically begins in mid-teens Stressful life events play role in onset There is a high level of comorbidity with other anxiety disorders and with mood disorders (Brown, Barlow, & Liebowitz, 1994). It is difficult to treat GAD successfully. In one five-year follow-up study, only 18% of clients had achieved a full remission of symptoms (Woodman et al., 1999).
. It is difficult to treat GAD successfully. In one five-year follow-up study, only 18% of clients had achieved a full remission of symptoms (Woodman et al., 1999).")
47
Cognitive-Behavioural Perspectives
Aetiology of GAD Cognitive-Behavioural Perspectives Learning view Anxiety regarded as having been classically conditioned to external stimuli, but with a broader range of conditioned stimuli. Cognitive This model focuses on control and helplessness. Cognitive theory emphasizes the perception of not being in control as a central characteristic of all forms of anxiety (Mandler, 1966).
.")
48
Intolerance Of Uncertainty & GAD
Related to this idea of control is the fact that predictable events produce less anxiety than do unpredictable events (see Mineka, 1992). Extensive research has shown the role of an intolerance of uncertainty in the experience of chronic worry and GAD (e.g., Ladouceur, Gosselin, & Dugas, 2000). Uncertainty intolerance is particularly relevant when assessing ambiguous situations, and appraisals of ambiguous situations mediate the association between uncertainty intolerance and worry (Koerner & Dugas, 2008).
. Extensive research has shown the role of an intolerance of uncertainty in the experience of chronic worry and GAD (e.g., Ladouceur, Gosselin, & Dugas, 2000). Uncertainty intolerance is particularly relevant when assessing ambiguous situations, and appraisals of ambiguous situations mediate the association between uncertainty intolerance and worry (Koerner & Dugas, 2008).")
49
Two-Factor Model Linking GAD With Approach-Avoidance Conflict
two factors are: intolerance of uncertainty and a fear of anxiety. GAD-prone people with an intolerance of uncertainty have a desire to engage in approach behaviours to reduce their feelings of uncertainty. However, they are also characterized simultaneously by a fear of anxiety that promotes the use of avoidance strategies designed to limit the experience of anxious arousal.

50
Worry Is Potentially Negatively Reinforcing
Worry distracts people from negative emotions. worry does not produce much emotional arousal. It does not produce the physiological changes that usually accompany emotion, and it actually blocks the processing of emotional stimuli. Therefore, by worrying, people with GAD are avoiding certain unpleasant images and so their anxiety about these images does not extinguish.

51
Aetiology of GAD (cont.)
Biological Perspectives GAD may have a genetic component. Neurobiological model for GAD based on fact that benzodiazepines are often effective in treating anxiety Receptor in the brain for benzodiazepines has been linked to the inhibitory neurotransmitter GABA Benzodiazepines may anxiety by release of GABA Drugs that block or inhibit the GABA system anxiety

52
Aetiology of GAD (cont.)
Psychoanalytic Perspective Unconscious conflict between the ego and id impulses The impulses, usually sexual or aggressive in nature, are struggling for expression, but the ego cannot allow their expression because it unconsciously fears that punishment will follow. Since the source of the anxiety is unconscious, the person experiences apprehension and distress without knowing why. The true source of anxiety—namely, desires associated with previously punished id impulses seeking expression—is ever-present.

53
Obsessive-Compulsive Disorder
No longer an anxiety disorder in DSM5

54
Obsessive-Compulsive Disorder
Obsessive-compulsive disorder (OCD)—a disorder in which the mind is flooded with persistent and uncontrollable thoughts (obsessions) and the individual is compelled to repeat certain acts again and again (compulsions)
—a disorder in which the mind is flooded with persistent and uncontrollable thoughts (obsessions) and the individual is compelled to repeat certain acts again and again (compulsions)")
55
Obsessions vs. Compulsions
Obsession— intrusive and recurring thoughts, impulses, and images Most frequent obsessions: fears of contamination, fears of expressing some sexual or aggressive impulse, and hypochondriacal fears of bodily dysfunction can take the form of extreme doubting, procrastination, and indecision. Most people with OCD keep the content and frequency of their obsessions secret for many years (Newth & Rachman, 2001).
.")
56
Obsessions vs. Compulsions
Compulsion — a repetitive behaviour or mental act that the person feels driven to perform to reduce the distress caused by obsessive thoughts or to prevent some calamity from occurring The activity is not realistically connected with its apparent purpose and is clearly excessive. Often an individual who continually repeats some action fears dire consequences if the act is not performed. Examples: checking, cleanliness and orderliness, avoiding particular objects, performing protective practices or a particular act primary obsessional slowness. when the slowness is the central problem and is not secondary to other OCD symptoms (eg checking)
")
57
What Makes Compulsions Worse?
According to Rachman (2002), three “multipliers” that increase the intensity and frequency of compulsive checking are: A sense of personal responsibility, the probability of harm if checking does not take place the predicted seriousness of harm.
, three multipliers that increase the intensity and frequency of compulsive checking are: A sense of personal responsibility, the probability of harm if checking does not take place. the predicted seriousness of harm.")
58
Behavioural and Cognitive Theories
Aetiology of OCD Behavioural and Cognitive Theories Learned behaviours reinforced by fear reduction Compulsive checking may result from a memory deficit. An inability to remember some action accurately (such as turning off the stove) or to distinguish between an actual behaviour and an imagined behaviour (“Maybe I just thought I turned off the stove”) could cause someone to check repeatedly. General research on OCD suggests inconsistent evidence of memory deficits for verbal information, but there is stronger evidence for impairments in memory for non-verbal information (Muller & Roberts, 2005).
 or to distinguish between an actual behaviour and an imagined behaviour ( Maybe I just thought I turned off the stove ) could cause someone to check repeatedly. General research on OCD suggests inconsistent evidence of memory deficits for verbal information, but there is stronger evidence for impairments in memory for non-verbal information (Muller & Roberts, 2005).")
59
Rachman’s Theory of Obsessions in OCD
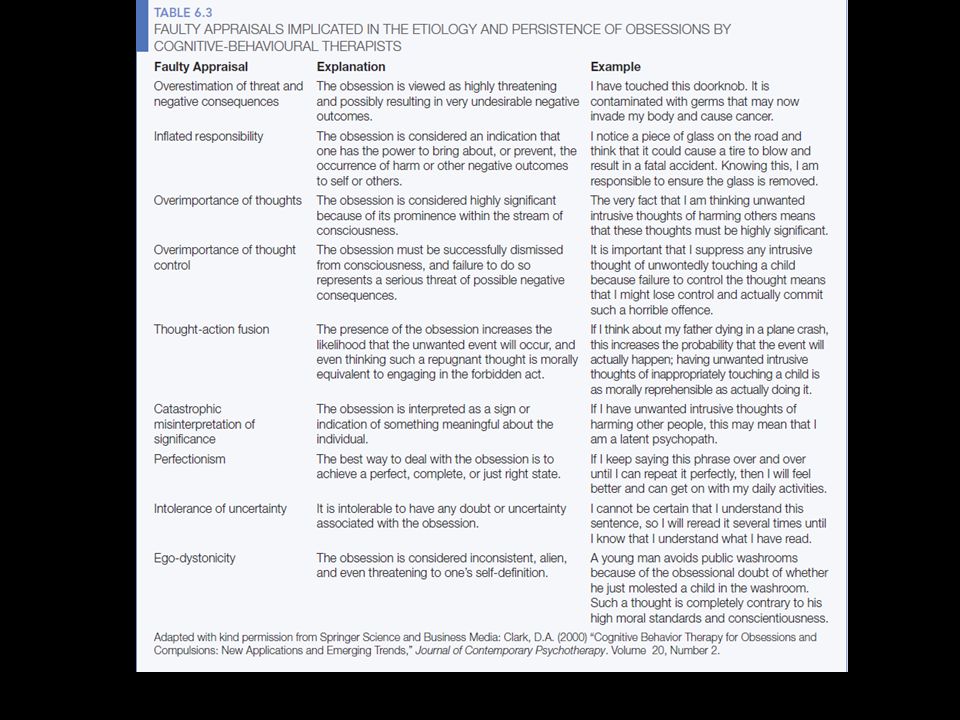
Obsessions often involve catastrophic misinterpretations of negative intrusive thoughts Rachman and Shafran (1998) identified a range of cognitive factors involved in OCD in addition to the obsessions themselves, including an inflated sense of personal responsibility for outcomes and a cognitive bias involving thought-action fusion. Thought-action-fusion involves two beliefs: (1) the mere act of thinking about unpleasant events increases the perceived likelihood that they will actually happen; (2) at a moral level, thinking something unpleasant (e.g., imagining the self hurting others) is the same as actually having carried it out.
 identified a range of cognitive factors involved in OCD in addition to the obsessions themselves, including an inflated sense of personal responsibility for outcomes and a cognitive bias involving thought-action fusion. Thought-action-fusion involves two beliefs: (1) the mere act of thinking about unpleasant events increases the perceived likelihood that they will actually happen; (2) at a moral level, thinking something unpleasant (e.g., imagining the self hurting others) is the same as actually having carried it out.")
61
Meta-Cognition In OCD There are meta-cognitive differences in OCD:
people with OCD have such highly developed cognitive self-consciousness that they reflect excessively on their cognitive processes (Janeck, Calamari, Riemann, & Heffelfinger, 2003).
.")
62
Aetiology of OCD (cont.)
Biological Factors Genetic evidence High rates of anxiety disorders occur among the first- degree relatives (10.3%) than control relatives (1.9%) Brain structure Encephalitis, head injuries, and brain tumours associated with the development of OCD PET scan studies shown activation in the frontal lobes The is a link to the basal ganglia a system linked to the control of motor behaviour Tourette ’s syndrome is marked by both motor and vocal tics and has been linked to basal ganglia dysfunction. People with Tourette ’s often have OCD as well (Sheppard et al., 1999).
 than control relatives (1.9%) Brain structure. Encephalitis, head injuries, and brain tumours associated with the development of OCD. PET scan studies shown activation in the frontal lobes. The is a link to the basal ganglia. a system linked to the control of motor behaviour. Tourette ’s syndrome is marked by both motor and vocal tics and has been linked to basal ganglia dysfunction. People with Tourette ’s often have OCD as well (Sheppard et al., 1999).")
63
Aetiology of OCD (cont.)
Biological Factors con’t. Hypothesized to be related to serotonin However, 40-60% of OCD clients treated with SSRIs do not show improvement

64
Aetiology of OCD (cont.)
Psychoanalytic Theory Classical psychoanalysis: Obsessions and compulsions are viewed as similar Result from instinctual forces, sexual or aggressive, that are not under control because of overly harsh toilet training (fixation at the anal stage) Alfred Adler viewed OCD as a result of feelings of incompetence due to an inferiority complex when children are kept from developing a sense of competence by doting or excessively dominating parents, they develop an inferiority complex and may unconsciously adopt compulsive rituals in order to carve out a domain in which they exert control and can feel proficient.
 Alfred Adler viewed OCD as a result of feelings of incompetence due to an inferiority complex. when children are kept from developing a sense of competence by doting or excessively dominating parents, they develop an inferiority complex and may unconsciously adopt compulsive rituals in order to carve out a domain in which they exert control and can feel proficient.")
65
Therapies For Anxiety Disorders
Those with an anxiety disorder are much less likely than people with other disorders (including depression) to seek treatment (Johnson & Coles, in press). many people who could be diagnosed by a clinician as having a phobia do not feel they have a problem that merits attention and this applies especially to those with social phobia.
 to seek treatment (Johnson & Coles, in press). many people who could be diagnosed by a clinician as having a phobia do not feel they have a problem that merits attention and this applies especially to those with social phobia.")
66
Behavioural Approaches To Anxiety Treatment
Systematic desensitization was the first major behavioural treatment to be used widely in treating phobias (Wolpe, 1958). The individual with a phobia imagines a series of increasingly frightening scenes while in a state of deep relaxation. Clinical and experimental evidence indicates that this technique is effective in eliminating, or at least reducing, phobias.
. The individual with a phobia imagines a series of increasingly frightening scenes while in a state of deep relaxation. Clinical and experimental evidence indicates that this technique is effective in eliminating, or at least reducing, phobias.")
67
In Vivo Exposure: Anxiety
In vivo exposure is often seen as superior using imagination In a meta-analytic review of 33 RCTs of the treatment of specific phobias, Wolitzky-Taylor, Horowitz, Powers, and Telch (2008) concluded that exposure- based treatment produced large effect sizes relative to no treatment and outperformed both placebo conditions and other psychotherapeutic approaches. In vivo exposure outperformed other modes of exposure (e.g., imaginal exposure and virtual reality) at post-treatment (but not at follow-up). in vivo exposure is associated with a high dropout rate and low treatment acceptance.
 concluded that exposure- based treatment produced large effect sizes relative to no treatment and outperformed both placebo conditions and other psychotherapeutic approaches. In vivo exposure outperformed other modes of exposure (e.g., imaginal exposure and virtual reality) at post-treatment (but not at follow-up). in vivo exposure is associated with a high dropout rate and low treatment acceptance.")
68
Virtual Reality (VR) Exposure
A meta-analysis of 23 studies comparing in vivo exposure with virtual reality (VR) exposure treatments has found VR exposure to be just as effective as in vivo exposure (Opris et al., 2012). VR exposure therapy has a powerful real-life impact and yields stable outcomes comparable to other treatment interventions. VR exposure treatment has comparatively better efficacy for the fear of flying. VR exposure has been dubbed in virtuo exposure (see Côté & Bouchard, 2008).
 exposure treatments has found VR exposure to be just as effective as in vivo exposure (Opris et al., 2012). VR exposure therapy has a powerful real-life impact and yields stable outcomes comparable to other treatment interventions. VR exposure treatment has comparatively better efficacy for the fear of flying. VR exposure has been dubbed in virtuo exposure (see Côté & Bouchard, 2008).")
69
Tailoring Treatment For Specific Phobias
Blood-and-injection phobias are distinguished from other phobias due to the distinctive reactions that people with these phobias have to the usual behavioural approach of relaxation paired with exposure (Page, 1994). Relaxation tends to make matters worse for people with blood-and- injection phobias. After the initial fright, accompanied by dramatic increases in heart rate and blood pressure, a person with a blood-and-injection phobia often experiences a sudden drop in blood pressure and heart rate and faints (McGrady & Bernal, 1986). By trying to relax, clients with these phobias may well contribute to the tendency to faint, increasing their already high levels of fear and avoidance, as well as their embarrassment (Ost, 1992). Clients with blood-and- injection phobias are now encouraged to tense rather than relax their muscles when confronting the fearsome situation (e.g., Hellstrom, Fellenius, & Ost, 1996).
. Relaxation tends to make matters worse for people with blood-and- injection phobias. After the initial fright, accompanied by dramatic increases in heart rate and blood pressure, a person with a blood-and-injection phobia often experiences a sudden drop in blood pressure and heart rate and faints (McGrady & Bernal, 1986). By trying to relax, clients with these phobias may well contribute to the tendency to faint, increasing their already high levels of fear and avoidance, as well as their embarrassment (Ost, 1992). Clients with blood-and- injection phobias are now encouraged to tense rather than relax their muscles when confronting the fearsome situation (e.g., Hellstrom, Fellenius, & Ost, 1996).")
70
Exposure With Response Prevention (ERP) for OCD
In this method the person exposes himself or herself to situations that elicit the compulsive act—such as touching a dirty dish—and then refrains from performing the accustomed ritual—hand washing. The assumption is that the ritual is negatively reinforcing because it reduces the anxiety that is aroused by some environmental stimulus or event, such as dust on a chair. Preventing the person from performing the ritual (response prevention) will expose him or her to the anxiety provoking stimulus, thereby allowing the anxiety to be extinguished.
 will expose him or her to the anxiety provoking stimulus, thereby allowing the anxiety to be extinguished.")
71
Exposure With Response Prevention (ERP) for OCD
the ERP treatment is arduous and unpleasant for clients. It typically involves exposures lasting upwards of 90 minutes for 15 to 20 sessions within a three-week period, with instructions to practise between sessions, as well. 17 to 19% of clients refuse treatment (for a review, see Clark, 2005), and refusal to enter treatment and dropping out are generally recognized problems for many interventions for OCD.
, and refusal to enter treatment and dropping out are generally recognized problems for many interventions for OCD.")
72
Social Skills Training With Social Phobia
Learning social skills can help people with social phobias who may not know what to do or say in social situations Some CBT therapists encourage clients to role-play interpersonal encounters in the consulting room or in therapy groups and several studies attest to the long-term effectiveness of this approach (e.g., Garcia- Lopez et al., 2006).
.")
73
Therapies With Phobias
Modelling therapy: fearful clients are exposed to filmed or live demonstrations of other people interacting fearlessly with the phobic object (e.g., handling snakes). Flooding a client is exposed to the source of the phobia at full intensity. Often a last resort
. Flooding. a client is exposed to the source of the phobia at full intensity. Often a last resort.")
74
Behavioural Treatment of GAD
It is difficult to find specific causes of the anxiety suffered by clients with GAD tend to prescribe more generalized treatment (intensive relaxation training), in the hope that if clients learn to relax when beginning to feel tense, their anxiety will be kept from spiralling out of control (Borkovec & Mathews, 1988). Clients are taught to relax away low-level tensions, to respond to incipient anxiety with relaxation rather than alarm. This strategy is quite effective in alleviating GAD (see Borkovec & Whisman, 1996).
, in the hope that if clients learn to relax when beginning to feel tense, their anxiety will be kept from spiralling out of control (Borkovec & Mathews, 1988). Clients are taught to relax away low-level tensions, to respond to incipient anxiety with relaxation rather than alarm. This strategy is quite effective in alleviating GAD (see Borkovec & Whisman, 1996).")
75
Cognitive Approaches to Phobias
Cognitive treatments for specific phobias have been viewed with scepticism because of a central defining characteristic of phobias: the phobic fear is recognized by the individual as excessive or unreasonable. If the person already acknowledges that the fear is of something harmless, what use can it be to alter the person ’s thoughts about it? There is no evidence that the elimination of irrational beliefs alone, without exposure to the fearsome situations, reduces phobic avoidance (e.g., Turner et al., 1992).
.")
76
Exposure-based Treatments Panic Disorders
One well-validated therapy developed by Barlow and his associates (e.g., Barlow & Craske, 1994) has three principal components: (1) relaxation training (2) a combination of Ellis- and Beck-type CBT interventions, including cognitive restructuring (3) exposure to the internal cues that trigger panic.
 has three principal components: (1) relaxation training. (2) a combination of Ellis- and Beck-type CBT interventions, including cognitive restructuring. (3) exposure to the internal cues that trigger panic.")
77
How Effective Is CBT For Treating OCD?
OCD is difficult to treat CBT conducted in clinical settings with well-trained clinicians has proven effective (see Hunsley & Lee, 2007; van Ingen et al., 2009). Jonsson and Hougaard (2008) conducted a meta- analysis of 13 trials of group CBT/ERP for OCD and concluded that the group treatments are effective; however, additional studies are required to compare the effectiveness of group and individual formats. In two studies, better results were achieved by group CBT relative to pharmacological treatment.
. Jonsson and Hougaard (2008) conducted a meta- analysis of 13 trials of group CBT/ERP for OCD and concluded that the group treatments are effective; however, additional studies are required to compare the effectiveness of group and individual formats. In two studies, better results were achieved by group CBT relative to pharmacological treatment.")
78
Dropout Rates In The Treatment of OCD?
While CBT is effective in treating OCD, Foa (2010) observed that it is still the case that about 20% of patients drop out and another 20% are not treated successfully. we know very little about what might work best for someone who has OCD but is a checker vs. an orderer or a compulsive washer.
 observed that it is still the case that about 20% of patients drop out and another 20% are not treated successfully. we know very little about what might work best for someone who has OCD but is a checker vs. an orderer or a compulsive washer.")
79
What Are The Key Processes Involved In Change in OCD?
Research is increasingly supporting the role of threat reappraisal in symptom improvement but the definitive study is still needed to establish threat reappraisal as the main factor vs. other mechanisms (see Smits, Julian, Rosenfi eld, & Powers, 2012).
.")
80
Behavioural Therapy Generally: The Need For Homework
All the behavioural and cognitive therapies for phobias have a recurrent theme—namely, the need for the client to begin exposing himself or herself to what has been deemed too terrifying to face. It should be noted that homework or between- session learning is considered to be an essential component of CBT.

81
Biological Approaches To Treatment Of Anxiety
Drugs that reduce anxiety are referred to as sedatives, tranquilizers, or anxiolytics (the suffix - lytic comes from the Greek word meaning to loosen or dissolve). Barbiturates the first major category of drugs used to treat anxiety disorders highly addictive great risk of a lethal overdose
. Barbiturates. the first major category of drugs used to treat anxiety disorders. highly addictive. great risk of a lethal overdose.")
82
Biological Approaches To Treatment Of Anxiety
Barbiturates they were supplanted in the 1950s by two other classes of drugs: propanediols (e.g., Miltown) benzodiazepines (e.g., Valium and Xanax).
 benzodiazepines (e.g., Valium and Xanax).")
83
Biological Approaches To Treatment Of Anxiety
Valium and Xanax are still used today, although they have been largely supplanted by newer benzodiazepines, such as Ativan and Clonapam. These drugs are of demonstrated benefit with some anxiety disorders; however, they are not used extensively with the specific phobias.

84
Biological Approaches To Treatment Of Anxiety
Drugs originally developed to treat depression (antidepressants) have become popular in treating many anxiety disorders, phobias included. monoamine oxidase (MAO) inhibitors Better in treating social phobias than benzodiazepine (Gelernter et al., 1991) as effective as CBT at a 12-week follow-up (Heimberg et al., 1998). The selective serotonin reuptake inhibitors (SSRIs), such as fluoxetine (Prozac), were also originally developed to treat depression. shown some promise in reducing social phobia in double-blind Canadian studies (Stein et al., 1999), and a meta-analysis of past studies initially confirmed their effectiveness (Federoff & Taylor, 2001).
 have become popular in treating many anxiety disorders, phobias included. monoamine oxidase (MAO) inhibitors. Better in treating social phobias than benzodiazepine (Gelernter et al., 1991) as effective as CBT at a 12-week follow-up (Heimberg et al., 1998). The selective serotonin reuptake inhibitors (SSRIs), such as fluoxetine (Prozac), were also originally developed to treat depression. shown some promise in reducing social phobia in double-blind Canadian studies (Stein et al., 1999), and a meta-analysis of past studies initially confirmed their effectiveness (Federoff & Taylor, 2001).")
85
Biological Approaches To Treatment Of Anxiety
Koen and Stein (2011) noted that up to 50% of people with OCD or social anxiety disorder do not respond to SRI treatment. there is little information about what to do for the patient with GAD who fails to respond to drug treatment. many drugs have undesirable side effects, ranging from nausea, dizziness, drowsiness, memory loss, and depression to physical addiction and damage to body organs (see Ryan et al., 2008).
 noted that up to 50% of people with OCD or social anxiety disorder do not respond to SRI treatment. there is little information about what to do for the patient with GAD who fails to respond to drug treatment. many drugs have undesirable side effects, ranging from nausea, dizziness, drowsiness, memory loss, and depression to physical addiction and damage to body organs (see Ryan et al., 2008).")
86
Psychosurgery For OCD Used occasionally
Cingulotomy - involves destroying two to three centimetres of white matter in the cingulum, an area near the corpus callosum. this intervention is viewed as a treatment of last resort, given its permanence, the risks of psychosurgery, and the poor understanding of how it works. Deep brain stimulation is also possible

87
Psychoanalytic Approaches
Attempt to uncover the repressed conflicts believed to underlie the extreme fear and avoidance characteristic of these disorders. Because the phobia itself was regarded as symptomatic of underlying conflicts, it was usually not dealt with directly. Indeed, direct attempts to reduce phobic avoidance were contraindicated because the phobia is assumed to protect the person from repressed conflicts that are too painful to confront.

88
Psychoanalytic Approaches
Many analytically oriented clinicians recognize the importance of exposure to what is feared, although they often regard any subsequent improvement as merely symptomatic and not as a resolution of the underlying conflict that was assumed to have produced the phobia (Wolitzky & Eagle, 1990).
.")
89
Post-Traumatic Stress Disorder
Extreme response to a severe stressor, including increased anxiety, avoidance of stimuli associated with the trauma, and a numbing of emotional responses. Note. Unlike the definitions of other psychological disorders, the definition of PTSD includes part of its presumed aetiology: a traumatic event or events that the person has directly experienced or witnessed involving the deaths of others, threatened death to oneself, serious injury, or a threat to the physical integrity of self or others. The event must have created intense fear, horror, or helplessness. PTSD is often experienced by first responder emergency workers, including police officers and firefighters.

90
PTSD In previous editions of the DSM, the traumatic event was defined as “outside the range of human experience.” This definition of being outside the range of human experience was considered too restrictive, as it would have ruled out the diagnosis of PTSD following such events as automobile accidents or the death of a loved one, or even prolonged exposure to abuse.

91
Acute Stress Disorder There is a difference between PTSD and acute stress disorder (a diagnosis introduced in DSM-IV) Nearly everyone who encounters a trauma experiences stress, sometimes to a considerable degree. This is normal. If the stressor causes significant impairment in social or occupational functioning that lasts for less than one month, an acute stress disorder is diagnosed.

92
Acute Stress Disorder The proportion of people who develop an acute stress disorder varies with the type of trauma they have experienced. Rape: over 90% motor vehicle accident 13% Some people get over an acute stress disorder, many go on to develop PTSD (Harvey & Bryant, 2002).
.")
93
PTSD The inclusion in the DSM of severe stress as a significant causal factor of PTSD was meant to reflect a formal recognition that the cause of PTSD is primarily the event, not some aspect of the person. However: most people who encounter traumatic life events do not develop PTSD. One study - only 25% of people who experienced a traumatic event leading to physical injury subsequently developed PTSD (Shalev et al., 1996); thus, the event itself cannot be the sole cause of PTSD.
; thus, the event itself cannot be the sole cause of PTSD.")
94
Three Major Clusters Of Symptoms In PTSD
Re-experiencing the traumatic event Avoidance of stimuli associated with the event or numbing of responsiveness Symptoms of increased arousal

95
Prevalence lifetime prevalence of PTSD in Canada is almost 1 in 10
one-month prevalence is about 1 in 25 Canadians (Van Ameringen et al., 2008). Prevalence varies depending on the severity of the trauma experienced
. Prevalence varies depending on the severity of the trauma experienced.")
96
Risk Factors of PTSD Risk Factors
Exposure to trauma and severity of trauma Gender (more females) Perceived threat to life Family history of psychiatric disorders Presence of pre-existing psychiatric disorders Early separation from parents Previous exposure to traumas Dissociative symptoms (including amnesia and out-of-body experiences) at the time of the trauma trying to push memories of the trauma out of one ’s mind (Ehlers et al., 1998). Tendency to take personal responsibility for failures Coping with stress by focusing on emotions (“I wish I could change how I feel”) Attachment style (insecure attachment style)
 Perceived threat to life. Family history of psychiatric disorders. Presence of pre-existing psychiatric disorders. Early separation from parents. Previous exposure to traumas. Dissociative symptoms (including amnesia and out-of-body experiences) at the time of the trauma. trying to push memories of the trauma out of one ’s mind (Ehlers et al., 1998). Tendency to take personal responsibility for failures. Coping with stress by focusing on emotions ( I wish I could change how I feel ) Attachment style (insecure attachment style)")
97
Protective Factors being exposed to less severe events
having high intelligence (an IQ of 115 or greater) (see Breslau, Lucia, & Alvarado, 2006).
 (see Breslau, Lucia, & Alvarado, 2006).")
98
Aetiology of PTSD Psychological Theories
PTSD arises from a classical conditioning of fear avoidances are built up, and they are negatively reinforced by the reduction of fear that comes from not being in the presence of the CS. Anxiety sensitivity Cognitive theorists characterize PTSD as a disorder of memory the hallmark feature being the constant involuntary recollection of the traumatic event (McNally, 2006). it has been shown across several studies that PTSD is associated with impaired memory of emotionally neutral stimuli. there is a robust association between PTSD and memory impairment and this tendency is stronger for verbal memory than visual memory (Brewin, Kleiner, Vasterling, & Field, 2007).
. it has been shown across several studies that PTSD is associated with impaired memory of emotionally neutral stimuli. there is a robust association between PTSD and memory impairment and this tendency is stronger for verbal memory than visual memory (Brewin, Kleiner, Vasterling, & Field, 2007).")
99
Psychodynamic theory proposed by Horowitz (1990)
memories of the traumatic event occur constantly in the person ’s mind and are so painful that they are either consciously suppressed (by distraction, for example) or repressed.
 or repressed.")
100
Aetiology of PTSD Biological theories Genetics
Specific domains of noradrenergic system Trauma may raise levels of norepinephrine Evidence for increased sensitivity of noradrenergic receptors in patients with PTSD

101
When to intervene? Many experts on trauma agree that it is best to intervene in some fashion as soon as possible after a traumatic event, well before PTSD has a chance to develop. The Psychological First Aid Field Operations Guide was developed to provide guidance to frontline practitioners who must respond immediately to mental health needs following a disaster or terrorist event (see Vernberg et al., 2008).
.")
102
Crisis intervention A promising approach for people who have been sexually assaulted is a CBT strategy that involves, in combination, exposing clients to trauma-related cues in imagination, teaching them relaxation, and helping them think differently about what happened (e.g., to not blame themselves) (Foa et al., 1995).
 (Foa et al., 1995).")
103
Prolonged Exposure Therapy
developed specifically to treat PTSD. It is a combined CBT approach that involves a step-by-step process of being exposed to imagery reflecting traumatic memories as well as actual life situations reflecting trauma. Exposure is accompanied by changing thoughts and cognitive appraisals as well as being taught specific skills such as regulating and controlling breathing (see Foa, Hembree, & Rothbaum, 2007). Research indicates that prolonged exposure therapy is effective. How does exposure work? possibility that it leads to the extinction of the fear response. it may also change the meaning that stimuli have for people.
. Research indicates that prolonged exposure therapy is effective. How does exposure work possibility that it leads to the extinction of the fear response. it may also change the meaning that stimuli have for people.")
104
Virtual reality exposure treatment
Virtual Iraq Virtual Iraq is a three-dimensional program that allows the therapist to gradually introduce a variety of sensations including audio cues, visual cues, vibrations, and even smells.

105
Eye Movement Desensitization and Reprocessing (EMDR).
purported to be extremely rapid—often requiring only one or two sessions— and more effective than the standard exposure procedures the client imagines a situation related to his or her problem, such as the sight of a horrible automobile accident. Keeping the image in mind, the client follows with his or her eyes the therapist ’s fingers as the therapist moves them back and forth about a foot in front of the client. This process continues for a minute or so or until the client reports that the horror of the image has been reduced.

106
Eye Movement Desensitization and Reprocessing (EMDR).
Then the therapist has the client verbalize whatever negative thoughts are going through his or her mind, again while following the moving target with his or her eyes. Finally, the therapist encourages the client to think a more positive thought, such as “I can deal with this,” and this thought, too, is held in mind as the client follows the therapist ’s moving fingers eye movements do not add anything to what may be happening as a result of exposure itself (e.g., Cahill, Carrigan, & Frueh, 1999), as well as a study showing that exposure therapy appears to be more effective than EMDR (Taylor et al., 2003).
, as well as a study showing that exposure therapy appears to be more effective than EMDR (Taylor et al., 2003).")
108
MMDA and PTSD One controversial development is the recent use of ecstasy (MMDA) in the treatment of PTSD. Mithoefer et al. (2011) conducted an RCT with 12 PTSD patients receiving ecstasy and 8 PTSD patients in the control condition receiving a placebo. Ten of the 12 patients (83%) in the treatment condition had clinically significant improvement vs. only two people in the control group.
 conducted an RCT with 12 PTSD patients receiving ecstasy and 8 PTSD patients in the control condition receiving a placebo. Ten of the 12 patients (83%) in the treatment condition had clinically significant improvement vs. only two people in the control group.")
109
Whatever the specific mode of intervention, experts in PTSD agree that social support is critical.
Sometimes finding ways to lend support to others can help the giver as well as the receiver (Hobfoll et al., 1991). Belonging to a religious group, having family, friends, or fellow traumatized individuals listen non-judgementally to one ’s fears and recollections of the trauma, and having other ways to feel that one belongs and that others wish to help ease the pain may spell the difference between post-traumatic stress and PTSD.
. Belonging to a religious group, having family, friends, or fellow traumatized individuals listen non-judgementally to one ’s fears and recollections of the trauma, and having other ways to feel that one belongs and that others wish to help ease the pain may spell the difference between post-traumatic stress and PTSD.")
110
Copyright Copyright © 2014 John Wiley & Sons Canada, Ltd. All rights reserved. Reproduction or translation of this work beyond that permitted by Access Copyright (The Canadian Copyright Licensing Agency) is unlawful. Requests for further information should be addressed to the Permissions Department, John Wiley & Sons Canada, Ltd. The purchaser may make back-up copies for his or her own use only and not for distribution or resale. The author and the publisher assume no responsibility for errors, omissions, or damages caused by the use of these programs or from the use of the information contained herein.
 is unlawful. Requests for further information should be addressed to the Permissions Department, John Wiley & Sons Canada, Ltd. The purchaser may make back-up copies for his or her own use only and not for distribution or resale. The author and the publisher assume no responsibility for errors, omissions, or damages caused by the use of these programs or from the use of the information contained herein.")
Similar presentations



 Anxiety Disorders.>")
















