Download presentation
Presentation is loading. Please wait.

1
The Tomotherapy Experience at Advocate Good Samaritan Hospital
Mark Pankuch

2
Today’s Discussion The History of Radiation at Good Samaritan
Quick Overview of the Tomotherapy Unit Treatment population and Statistics of our experience Results from Shielding Comparison of plans

3
Advocate Good Samaritan
Treated first patient on May 13, 2002 Single Linac Vault with a Seimens Primus Hand me down GE CT scanner from radiology Paper-less / Film-less department

4
Advocate Good Samaritan
Within two years reached capacity for a single Linac department Began offering HDR treatments Strong administrative and physician support for expansion

5
Advocate Good Samaritan
New Vault was needed Doubling current patient volumes appeared as an over estimation for potential volume Present day IGRT with OBI not commonly available

7
What did Tomotherapy Offer that Good Sam was missing?
IGRT “Top End” IMRT

8
The Answer For Good Sam?

9
Tomotherapy

10
Tomotherapy MLC

11
MLC’s Oriented in the Sagital Plane

12
The Treatment Process Patient is set up on table to moveable lasers (2 min) High energy CT scan performed in the Tx Position (3 Min) New images are fused with planning CT images (3 Min) Adjustments are made for patient position (2 min) Treatment is delivered (10 Min)
 Adjustments are made for patient position (2 min) Treatment is delivered (10 Min)")
13
Of Special Note on Hardware:
No flattening filter Output ~ 900 MU / min Tx = 10,000 MU MLC’s very, very fast (us) Capable of MVCT export MVCT ~ 2-3 cGy
 Capable of MVCT export. MVCT ~ 2-3 cGy.")
14
Planning System Single workstation for planning
Cluster of 16 computers, w/ dual processors for computing. Optimizations done on “beamlets” that can be calculated overnight Very few contouring tools, need another system for contouring and fusions No planning review station, system not multitasking

15
What type of patients have we treated?

16
Tomotherapy Not optimal for all treatment sites
Rotational / Helical Treatments Need the capability to give low doses to large areas of normal tissues Ability of “cave out” doses Very conformal, with good dose drop off

20
Simultaneous Boost

24
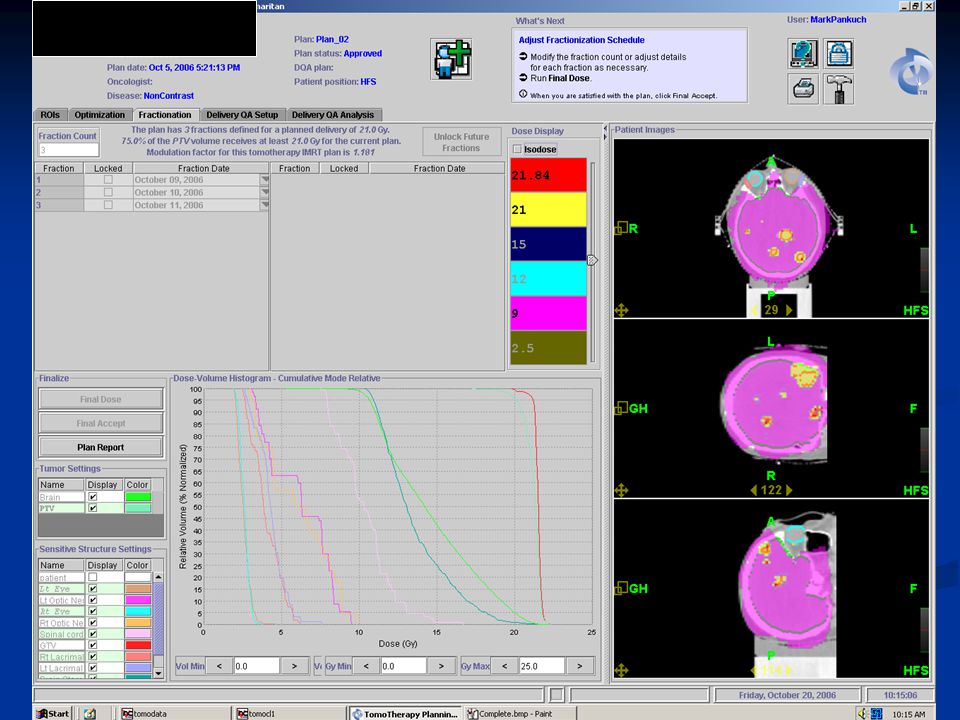
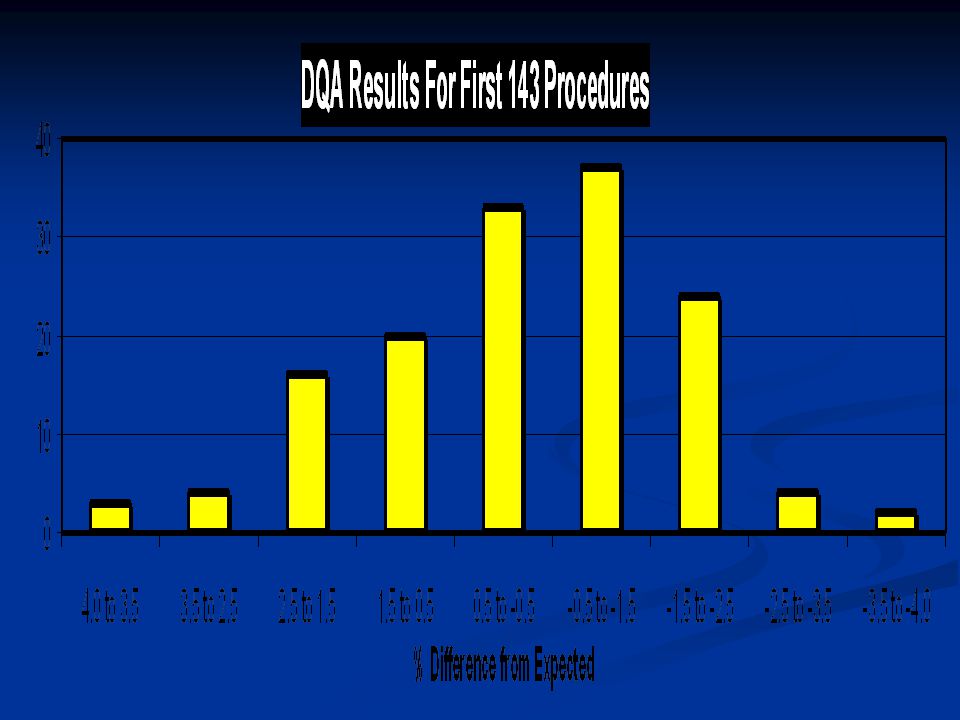
DQA Tomotherapy Supplied Phantoms
Film and Point dose taken on every patient Planning system has built-in QA tools Film analysis evaluated by calculating gamma index (Low et.al., Med Phys 25, 1998) 3% Dose 3mm DTA
 3% Dose. 3mm DTA.")
28
QA cGy / MU cGy / min Lasers coincidence Table Accuracy
Field Consistency MLC accuracy

29
Clinical Outcomes Pelvis patients decreased side effects
Prostate patients no side effects (78Gy) Brain Patients get ring shape hair loss Head / Neck patients Still have skin reactions Considerably reduces reaction in mouth Need more time for long term results
 Brain Patients get ring shape hair loss. Head / Neck patients. Still have skin reactions. Considerably reduces reaction in mouth. Need more time for long term results.")
30
Skin Reactions

31
Shielding Considerations
Large majority of shielding needed because of leakage Scatter Radiation Primary beam

32
Shielding Considerations
X = W * U * T * ISF Workload: 30 Patients/day 10 min Tx time 880MU/min 66,000,000 MU/year Usage Factors = 1 Occupancy Factor as usual Occupational areas kept to 10% of limits ISF from 3 meters

33
Shielding Considerations, Leakage
Leakage levels obtained from chart like CT scanner Leakage was measured and plotted as a function of position around the gantry and radial distance All leaves closed for measurements Leakage fraction at 3 meters was used ISF from 3 meters

34
Shielding Considerations, Scatter
Scatter levels a function of position around gantry Greatest at opening of couch With all leaves open, can be 186% of leakage exposure Clinically, the exposure can be reduced by a factor of 16 Maximum % scatter increase = 12%, I used 15%

35
Shielding Considerations, Primary
Unit has a built in Primary Beam Block, 13cm Pb The primary beam was 6.3% of the overall radiation at 2.5 cm from the isocenter Clinically, the exposure can be reduced by a factor similar to scatter due to closed leaves I ignored reduction factor, and increased exposure by 6.3%.

36
Shielding Results North Wall South Wall West Wall East Wall Ceiling
Door Calculated Exposure (mR/hr) 0.163 0.042 0.017 0.009 0.058 0.278 Measured Exposure (mR/hr) 0.288 0.012 0.005 0.013 0.188 Ratio of Measured / Calculated 141% 22% 26% 117% 17% 54% Ratio of Measured / Required 58% 12% 5% 3% 38%
 Measured Exposure (mR/hr) Ratio of Measured / Calculated. 141% 22% 26% 117% 17% 54% Ratio of Measured / Required. 58% 12% 5% 3% 38%")
37
Plan Comparison Tomotherapy CMS XIO, Step and Shoot
Varian Eclipse, Sliding Window

44
Which is best?? Depends …….. Many systems now have IGRT
Workload Needs Patient sites Many systems now have IGRT Where is IGRT going? No Breath Gateing on Tomotherapy Where is gateing doing?

45
In the future for Tomotherapy
Adaptive treatments Live time optimizations Conductivity with IMPAC Live time QC Breath Coaching Methods

46
Questions ?? Thanks for your attention!
Free tour of the Cancer Center after lunch Questions ???

Similar presentations































 Topic:>")

