Download presentation
Presentation is loading. Please wait.

1
Endocrine dysfunction (Hormone imbalances) in Diamond Blackfan Anemia
Dr Amit Lahoti Dr Phyllis Speiser Cohen Children’s Medical Center of New York North Shore LIJ Hospital System

2
Diamond Blackfan Anemia (DBA)
is a rare condition. Really!!!

3
DBA Beta thalassemia Sickle-cell disease 5-7 per 1,000,000 live births
1 per 500 African-American live births Sickle-cell disease

4
Role of a registry For rare conditions, clear guidelines on how to manage the disease or its complications often not available. A registry provides a unique opportunity to do systematic research. Until more research data are available, doctors use best practices learned from other somewhat similar conditions.

5
Treatment course of DBA
BMT recipients In a cross-sectional analysis of the DBAR at a given timepoint, 40% of patient are receiving transfusions, 40% are on steroids, and 20% have received a BMT or are in remission. There is a 20% chance of going into remission but not 20% of the patients are in remission at any given time.

6
Pros and cons of DBA treatments
Corticosteroids Chronic Transfusions Bone marrow transplant Pros No risk of iron overload First line treatment for severe anemia under 1y Can lead to resolution of anemia Can improve quality of life Cons Risk of low bone density Frequent hospital visits for transfusions Risk of Graft versus Host Disease (GVHD), and infection Excess weight gain & impaired growth Endocrine complications of iron overload Risk of graft rejection Increased risk of diabetes (at high doses) Side-effects of immunosuppressive drugs & radiation
, and infection. Excess weight gain & impaired growth. Endocrine complications of iron overload. Risk of graft rejection. Increased risk of diabetes (at high doses) Side-effects of immunosuppressive drugs & radiation.")
7
Where do hormones come from and what do they do?

8
Risk of Hormone disorders in patients with DBA: Is it real?

9
*Unpublished data presented at Pediatric Endocrine society meeting at Washington DC, 2013

10
You or some one sitting next to you may have a similar story….
At 6 months: Diagnosed with DBA Monthly transfusions started. Subsequently developed Iron overload Chelation therapy with Desferal started At 14.5 years, 7/2004: went to ER for frequent urination, excessive thirst and 15 lb weight loss. Blood glucose markedly elevated. Diagnosed with Diabetes mellitus, Insulin therapy started Two months later, 9/2004: Thyroid function tests show Thyroid gland failure. Thyroid hormone started Desferal started by nightly subQ pump

11
In the next year… At 15 years, 12/2004: Teen non-compliant with insulin regimen & diet. Poor blood glucose control, stunted growth, despite normal GH levels. Diagnosed Growth hormone resistance. Growth hormone therapy started At years, 10/2005: Delayed puberty with evidence of Pituitary failure. Testosterone therapy started. At 16.5 years, 5/2006: Multiple seizures related to low blood glucose despite not being compliant with insulin regime. Diagnosed with Adrenal insufficiency Hydrocortisone therapy started.

12
And as time went by… Two months later, 7/2006: Complaints of frequent urination at night. Diagnosed Diabetes insipidus. DDAVP treatment started. At 17.5 years, 8/2007: Evidence of Diabetic kidney damage. Enalapril treatment started. At 18 years, 2/2008: Growth hormone therapy stopped. Adult height: 5 feet.

13
Hormone problems can start in childhood!
You are never “too young” to be tested. Early diagnosis can avoid later problems.

14
Questions? What are these conditions? How common are these? Are you at risk? How can you be tested for these? How are they treated?

15
Hypogonadism What is it? Absent or delayed puberty

16
Hypogonadism What is Delayed Puberty?
In girls, no breast development by 13 years, or no periods by 15 years or by 2 years after breast development. In boys, no testicular enlargement by 14 years

17
Hypogonadism How common? How to diagnose? How to treat?
With iron overload: % After BMT: Females- ovarian malfunction in ~100% Males- testicular dysfunction in 0-40% How common? Blood sampling for pituitary puberty-regulating hormones (LH and FSH) and sex hormones (Testosterone or Estradiol). Bone age x-ray of hand. How to diagnose? Males: Testosterone injections or skin gel. Females: Estrogen oral or skin gel. How to treat?
 and. sex hormones (Testosterone or Estradiol). Bone age x-ray of hand. How to. diagnose Males: Testosterone injections or skin gel. Females: Estrogen oral or skin gel. How to. treat")
18
Insufficient thyroid hormone
Hypothyroidism Insufficient thyroid hormone What is it?

19
Hypothyroidism Or, no symptoms at all!!! ( especially in early stages)
Feeling cold out of ordinary How you may feel? Not growing well Or, no symptoms at all!!! ( especially in early stages)
")
20
Hypothyroidism How common? How to diagnose? How to treat?
Patients with iron overload: 2-20 % Patients on steroids and after BMT: Less common, frequency unknown How common? By measuring blood levels of: Thyroid stimulating hormone (TSH); and Total and free Thyroid hormone (T4) How to diagnose? How to treat? Once a day thyroid hormone (tablets)
; and. Total and free Thyroid hormone (T4) How to. diagnose How to. treat Once a day thyroid hormone (tablets)")
21
Adrenal insufficiency
Not enough adrenal hormones What is it? Stress hormone (cortisol) Salt retaining hormone (Aldosterone) Male hormones
 Salt retaining hormone (Aldosterone) Male hormones.")
22
Adrenal insufficiency
Dark color of non-sun- exposed areas Low BP and dizziness Extreme tiredness Nausea, vomiting, abdominal pain, diarrhea, constipation Muscle weakness Although the picture I have used is of an old lady, not everybody who develops this is old Symptoms may be missed or attributed to anemia or missed!

23
Adrenal insufficiency
Patients on steroids: considered to have adrenal insufficiency Patients with iron overload: biochemical adrenal insufficiency (often partial): 18-45% How common? Blood measurements of: 8 AM cortisol level, Plasma renin activity, aldosterone, Androstenedione and DHEAS levels How to diagnose? Hydrocortisone: to replace stress hormone. May only be needed during periods of stress. Fludrocortisone: salt-retaining hormone. How to treat?
: 18-45% How. common Blood measurements of: 8 AM cortisol level, Plasma renin activity, aldosterone, Androstenedione and DHEAS levels. How to. diagnose Hydrocortisone: to replace stress hormone. May only be needed during periods of stress. Fludrocortisone: salt-retaining hormone. How to. treat")
24
Quiz Time!!!

25
Question #1 Which of the following is NOT a part of the endocrine system? Thyroid Pituitary Appendix Adrenals

26
Question #2 This gland is sometimes called the master gland, though it is only about the size of a pea Thyroid Pituitary Pineal Hypothalamus

27
Question #3 Which of the following is the largest endocrine gland in the body: Thyroid Parathyroid Pancreas Adrenal

28
Diabetes mellitus What is it? Not enough insulin hormone

31
Diabetes mellitus Both iron overload and glucocorticoids lead to:
↓in insulin secretion; and ↓ in insulin sensitivity

32
Diabetes mellitus How common? How to diagnose? How to treat?
With Iron overload: 9-14% On Chronic glucocorticoids: dose dependent. May be reversible. BMT: depends on pre-transplant factors. How common? Fasting blood glucose Fructosamine level (HbA1c may not be reliable if on transfusions) Oral glucose tolerance test How to diagnose? Diet changes, Insulin therapy and/or Oral medications How to treat?
 Oral glucose tolerance test. How to. diagnose Diet changes, Insulin therapy and/or. Oral medications. How to. treat")
33
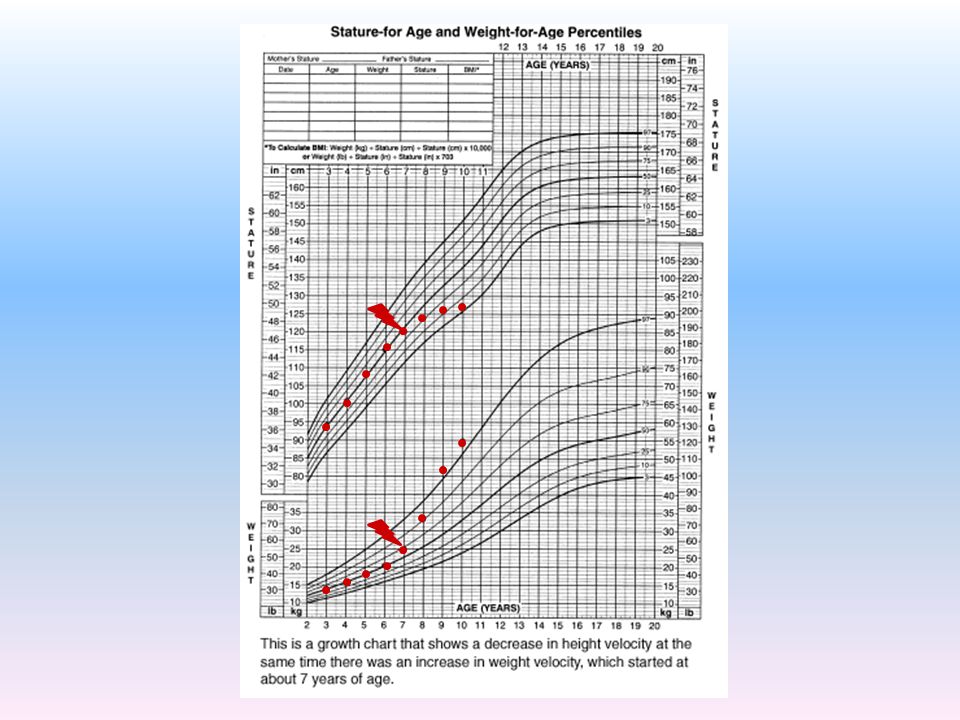
Growth Problems For patients <18 years age:
How many of you are shown your/ your child’s growth chart during the visit with the pediatrician or hematologist? How many of you have asked to see your/ your child’s growth chart during these visits? Growth chart is an important tool to detect poor growth or short stature at an early age!!!

35
Growth problems Short stature Anemia and ?DBA itself
Absent/ Abnormal puberty Iron overload Short stature Hypothyroidism Low Growth hormone Glucocorticoids Multiple causes of poor growth in DBA patients

36
Growth problems How common? How to diagnose? How to treat?
DBA itself: Reported short stature ~30% Effect on growth due to iron overload or steroids alone is hard to quantify in DBA due to this. BMT: may improve growth. How common? Regular growth monitoring for early detection Laboratory testing to rule out specific endocrine causes. How to diagnose? When to treat? Specific to the cause. However, final height may still be low for mid-parental height. How to treat?

37
Bone disorders How?

38
Bone disorders Weak bones Hypogonadism
Low Vitamin D & parathyroid gland failure Iron overload Weak bones Diabetes mellitus ? Low Growth hormone Glucocorticoids Multiple causes of poor bone density in DBA patients

39
Bone disorders How common? How to diagnose? How to treat?
With Iron overload: upto 50% On Chronic glucocorticoids: Dose and duration dependent. After Bone marrow transplant: Not known How common? Test for other endocrine problems Blood levels of Calcium, parathyroid hormone and vitamin D Bone mineral density scan How to diagnose? When to treat? Treat any co-existing hormone problem Vitamin D supplements: Adequate level? Other medications: Bisphosphonates Newer drugs being developed. How to treat?

40
Importance of Screening
Vague symptoms may also be seen with anemia itself. Often no/minimal symptoms in early stages. 14% impaired glucose tolerance 1.5% Diabetes mellitus 84.5%: normal Diabetes screening in non- diabetic otherwise asymptomatic beta thalassemia patients

42
Importance of Chelation
Impaired glucose tolerance (IGT) Years 12.4% Normal glucose tolerance ~10 Years Insulin dependent diabetes mellitus Intensive chelation in patients with IGT can improve beta-cell function, improve blood glucose values. Less effective in patients who have developed DM and in improving insulin resistance.
 Years. 12.4% Normal glucose tolerance. ~10 Years. Insulin dependent diabetes mellitus. Intensive chelation in patients with IGT can improve beta-cell function, improve blood glucose values. Less effective in patients who have developed DM and in improving insulin resistance.")
43
Treatable nature of most of these conditions
Treatable nature of most of these conditions!- That’s what I love about endocrinology!!! Timely diagnosis & treatment can prevent morbidity and possible mortality associated with some endocrine conditions. Versus possible long-term adverse effects of an untreated endocrine problem.

44
What do we need to do? The only published reports about hormone problems in DBA patients are in form of case reports or case series with few patients. Collect more information about endocrine problems in DBA patients like you. Vs

45
About our research study
SPECIFIC AIMS: To study the effects of iron overload on various endocrine glands in DBA patients receiving transfusions. To estimate how common are these hormone abnormalities in the DBA population and correlate it with measures of iron overload. To recommend a possible method to screen the at-risk DBA patients for endocrine dysfunctions at regular intervals. To compare the presence of endocrine dysfunction in chronic transfusion dependent DBA population with DBA patients not on chronic transfusions and beta thalassemia major patients on chronic blood transfusions.

46
About our research study
Eligibility Criteria: Inclusion criteria: Age 1-39 years; and Diagnosed with DBA and enrolled in DBA Registry (DBAR), or Diagnosed with beta thalassemia major and followed at NSLIJ pediatric hematology division. Exclusion criteria: Pregnant; or Having received a bone marrow transplant
, or. Diagnosed with beta thalassemia major and followed at NSLIJ pediatric hematology division. Exclusion criteria: Pregnant; or. Having received a bone marrow transplant.")
47
About our research study
Participation involves a standard endocrine evaluation. This includes blood tests that can be ordered and drawn at your primary institution. The participation consent asks for permission for us to receive the endocrine evaluation results. Our goal is 75 DBA patients and 25 thalassemia patients total for the study. THANK YOU IN ADVANCE FOR YOUR PARTICIPATION!!!

48
Thanks for listening!!!

Similar presentations











 By: Anna Heideman & Angela Mullins.>")



 are the triangle-shaped and orange- colored endocrine.>")






