Download presentation
Presentation is loading. Please wait.

1
Constipation, Encopresis, Diarrhea
Abbey Rupe, MD 2.7.12

2
Definitions “Rome III” diagnostic categories of functional disorders of defecation in children: Functional constipation In infants and preschool children In children 4-18 years of age Infant dyschezia Nonretentive fecal incontinence

3
Functional constipation--Dx
Infants and toddlers: 2 or more of the following present for at least 1 month: 2 or fewer defecations/week At least 1 episode of incontinence after being toilet trained Hx of excessive stool retention Hx of painful or hard bowel movements Presence of large fecal mass in the rectum Hx of large-diameter stools that may obstruct the toilet

4
Functional constipation--Dx
Children w/ developmental age 4-18 yrs; at least 2 of the following present for at least 2 months: 2 or fewer defecations/week At least 1 episode of fecal incontinence/week Hx of retentive posturing or excessive volitional stool retention Hx of painful or hard bowel movements Presence of a large fecal mass in the rectum Hx of large-diameter stools that may obstruct the toilet

5
Functional vs Organic constipation
Organic causes: < 5% of cases Anatomic: anal stenosis, imperforate anus Metabolic/GI: hypothyroidism, CF, diabetes mellitus, celiac disease Neuropathic: spinal cord abnormalities, tethered cord Intestinal nerve/muscle disorders: Hirschsprung disease, neuropathies Misc: cow’s milk protein intolerance, lead ingestion, vit D intoxication, botulism

6
Functional constipation-etiology
3 periods when kids prone to develop constipation: Introduction of cereals and solid food to infant’s diet Toilet training Starting school

7
Functional constipation--causes
Painful defecation Can start a vicious cycle Toilet training Stool is held for longer periods between BMs Power struggles can develop Diet Highly processed foods consumed at the expense of fruit, veggies, and fiber Cow’s milk and constipation???? controversial

8
Evaluation History Delayed passage of meconium Painful defecation
Blood on stool Toilet training issues Voiding dysfunction and enuresis Diet Changes at home/school Family hx

9
Evaluation Hx: signs suggesting possible organic cause:
Weight loss or poor weight gain Anorexia Delayed growth Delayed passage of meconium (after 48 hours) Urinary incontinence Passage of blood (unless due to anal fissure) Constipation present since birth/early infancy Acute constipation Fever, vomiting, diarrhea Extraintestinalsx
 Urinary incontinence. Passage of blood (unless due to anal fissure) Constipation present since birth/early infancy. Acute constipation. Fever, vomiting, diarrhea. Extraintestinalsx.")
10
Evaluation Physical exam Abdominal distention Mass in suprapubic area
Anal fissure Soiled underwear Anal sphincter tone Size of rectal vault Impacted stool Lower back skin defects

11
Evaluation PE findings suggestive of organic cause: FTT
Abdominal distention Lower spine abnormalities Anteriorly displaced anus Tight, empty rectum in presence of palpable fecal mass Absent anal wink Absent cremasteric reflex Decreased lower extremity tone or strength

12
Evaluation Laboratory (if indicated) KUB CBC Thyroid
Celiac disease panel Barium enema Anorectalmanometry Rectal biopsy Motility studies Sweat chloride

14
Evaluation Findings supportive of functional etiology:
Onset coincides with dietary changes, toilet training, or painful bowel movements Stool withholding behavior Good response to conventional treatment

15
Infants: Constipation vs normal stooling
Breast-fed infants: average 3 stools/day Range: BM with every feed to BM every 7-10 days Formula-fed infants: Average 2/day Can vary with formula Soy-based—tend to produce harder stools; hydrolyzed casein formulas tend to produce looser stools

16
Infants Grunting, apparent straining, turning red in the face, etc does not necessarily mean an infant is constipated More appropriate measure is consistency of the stool Efforts >10 minutes to produce soft stool: “infant dyschezia” – failure to relax pelvic floor during defecation effort; resolves spontaneously with time

17
Infants “normal” stools Constipated: Reassure, reassure, reassure
Press on feet, press knees to belly, raise vertical, etc Constipated: 1 tsp dark Karo syrup bid Miralax Glycerin suppository Juice—pear, apple, prune If on solids: increase pear, prune, plums, beans, peas, peaches Decrease rice cereal, applesauce, bananas

18
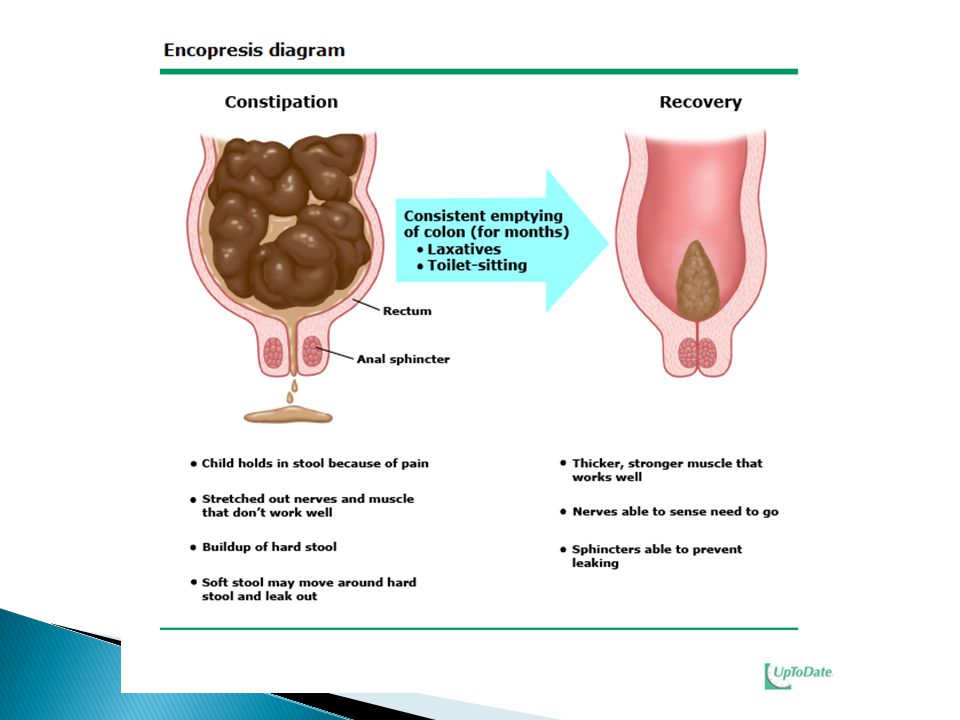
Treatment of Children Goal: 1 soft, easily passed stool daily
Education “cycle” of constipation Length of treatment Safety of medication used 3 phases: Disimpaction Maintenance Follow-up

19
Disimpaction Options: oral or NG medications, rectal medications, or combination Inpatient vs outpatient Oral: Polyethylene glycol (Miralax) Polyethylene glycol-electrolyte solution Mineral oil (don’t use if at risk for GER) Other: magnesium hydroxide, magnesium citrate, lactulose, sorbitol, senna, bisacodyl
 Polyethylene glycol-electrolyte solution. Mineral oil (don’t use if at risk for GER) Other: magnesium hydroxide, magnesium citrate, lactulose, sorbitol, senna, bisacodyl.")
20
Disimpaction Rectal Phosphate sodium enema (2 yrs and older)
Mineral oil enema Bisacodyl suppository (older children) Glycerin suppository (infants)
 Glycerin suppository (infants)")
21
Maintenance Polyethylene glycol Magnesium hydroxide Lactulose
Mineral oil

22
Medications Polyethylene glycol (PEG 3350, Miralax) Osmotic laxative
OTC grams/kg/day Mix in 4-8 ounces liquid Increase or decrease by ½ to 1 tsp every other day until stools soft and daily

23
Medications Mineral oil Lubricant laxative
? Interfere with absorption of fat soluble vitamins Administer in mid-afternoon and bedtime +/- give multivitamin More palatable if chilled and served with a fat- containing food the child likes (pudding, yogurt, ice cream, chocolate syrup) Avoid in kids < 1 yr of age and those at risk for GER (aspiration pneumonitis)
 Avoid in kids < 1 yr of age and those at risk for GER (aspiration pneumonitis)")
24
Medications Other osmotic laxatives: Stimulant laxatives
Milk of magnesia Lactulose Stimulant laxatives Senna, bisacodyl

25
Maintenance Behavior modification: “Poop Journal”
“scheduled sitting” on the toilet for 5-10 minutes at same time each day (preferable within 30 minutes after a meal) Provide footstool for support if needed Reward system “Poop Journal”
 Provide footstool for support if needed. Reward system. Poop Journal")
27
Maintenance/prevention
Dietary changes Increase intake of fruit, raw veggies, bran, whole- grain breads, cereals, and fluids other than milk Cow’s milk Consider 1-2 week trial of elimination in atopic children whose constipation is unresponsive to other measures ?probiotics

28
Maintenance/prevention
When to discontinue medications? Depends on child and severity of constipation Taper gradually, resume if constipation returns

29
Encopresis/fecal incontinence
Constipation with fecal incontinence—80- 95% Nonretentive fecal incontinence—5-20% Rome III criteria: Children with developmental age of >4 yrs, with all the following present for at least 2 months: Defecation into places inappropriate to the social context at least once/month No underlying disease process to explain the symptoms No evidence of constipation

30
Constipation-associated fecal incontinence
Manage as you would for severe constipation

32
Non-retentive fecal incontinence
Causes: unclear Some association w/ behavioral and attention problems as well as anxiety and depressive symptoms Soiling episodes often linked to certain persons or situations Up to 40% have never been fully toilet trained

33
Non-retentive Treatment: Outcome: No widely effect treatments
Behavior modification Highly structured toilet training protocol aimed at frequent efforts at defecation Reward system Psychosocial diagnosis and support Outcome: one study found 29% resolution at 2 yrs, 65% after 5 yrs, and 90% after 10 years

34
Indications for referral
Consider when oral and/or rectal medications are ineffective for disimpaction or when dietary and laxative therapy are ineffective Complete laboratory data prior to consultation (thyroid, calcium, celiac disease, lead) Referral options: Wichita: 2 peds gastroenterologists Children’s Mercy: peds GI, BRICK clinic
 Referral options: Wichita: 2 peds gastroenterologists. Children’s Mercy: peds GI, BRICK clinic.")
35
Constipation questions?

36
Diarrhea Acute Chronic
Passage of loose or watery stools at least 3x/day in a 24-hour period Lasts <14 days Chronic Stool volume of >10 gm/kg/day (infants/toddlers) or >200gm/day (older children) x14 or more days Typically means: loose or watery stools occurring at least 3x/day
 or >200gm/day (older children) x14 or more days. Typically means: loose or watery stools occurring at least 3x/day.")
37
Acute diarrhea Etiology Infectious gastroenteritis
Acute watery diarrhea Rotavirus (infants/young children) E. coli (older children) Invasive (bloody) diarrhea—frank blood in stool + fever Shigela Salmonella Campylobacter EHEC EIEC Other: influenza, HIV, pneumonia, UTI, meningitis, sepsis
 E. coli (older children) Invasive (bloody) diarrhea—frank blood in stool + fever. Shigela. Salmonella. Campylobacter. EHEC. EIEC. Other: influenza, HIV, pneumonia, UTI, meningitis, sepsis.")
38
Acute diarrhea Assessment:
Type of diarrheal illness (watery, invasive, chronic) Assess hydration Assess comorbid conditions
 Assess hydration. Assess comorbid conditions.")
39
Assess hydration status (WHO)
Clinical feature < 5 % dehydrated 5-10 % dehydration >10% dehydration Gen. appearance Well, alert Restless, irritable Lethargic or unconscious Eyes Normal Sunken Thirst Drinks normally, not thirsty Thirsty, drinks eagerly Drinks poorly or unable to drink Skin pinch Goes back quickly Goes back slowly Goes back very slowly Estimated fluid deficit < 50 ml/kg ml/kg >100 ml/kg

40
Diagnostic studies Not indicated in most cases
Dehydration requiring IVF Stool studies: Viral antigen (rota) Culture (bloody diarrhea) O and P (recent travel) C. diff (recent abx)
 Culture (bloody diarrhea) O and P (recent travel) C. diff (recent abx)")
41
Treatment—acute watery diarrhea
Fluid and electrolytes Replacement Maintenance < 2 yrs: ml ORS/episode of V/D > 2 yrs: ml ORS/episode of V/D Oral Rehydration Solution Mixture of water, salts, and glucose Pedialyte, etc IVF Rehydrate with NS boluses (20 ml/kg), followed by dextrose-containing IVF
, followed by dextrose-containing IVF.")
42
Treatment--AGE Refeeding
Feeding can be resumed as soon as rehydration is complete Feed age-appropriate diet BRAT is unnecessarily restrictive

43
Treatment--AGE Pharmacotherapy Antibiotics—not indicated
Antidiarrheal—not recommended Antimotility (i.e. loperamide)—not recommended due to side effects (lethargy, CNS depression, etc) Antisecretory (i.e. bismuth)—contain salicylates (EVEN Children’s PeptoBismol) Probiotics Reduce stool output and diarrhea duration Antiemetics--controversial
—not recommended due to side effects (lethargy, CNS depression, etc) Antisecretory (i.e. bismuth)—contain salicylates (EVEN Children’s PeptoBismol) Probiotics. Reduce stool output and diarrhea duration. Antiemetics--controversial.")
44
Chronic diarrhea Post-enteritis syndrome
Most acute enteric infections resolve within 14 days Occasionally, acute GE can cause mucosal damage to small intestine and trigger chronic diarrhea ? Secondary to transient lactase deficiency Probiotics may speed recovery

45
Chronic diarrhea DDx list is HUGE! Functional Enteric infection
Excessive juice/osmotically active carb intake Idiopathic Enteric infection Postentereitis syndrome Parasites Bacteria Viruses CMV, rota, HIV

46
Chronic diarrhea DDx, cont’d CF Immune deficiency
Abnormal immune response Celiac disease Food allergic enteropathy IBD Protein losing gastroenteropathy Factitious diarrhea

47
Chronic diarrhea Lab Celiac serology (anti-tTG)
Stool pH, electrolytes, reducing substances Occult blood and leukocytes Stool fat Concern for IBD: CBC, albumin, ESR Sweat chloride Fecal elastase

48
“Toddler’s Diarrhea” Aka Functional Diarrhea or Chronic nonspecific diarrhea of childhood: Painless passage of 3 or more large, unformed stools during waking hours for 4 or more weeks Onset in infancy or preschool years Without FTT or specific definable cause

49
Toddler’s Diarrhea Early morning stools: large and semi-formed
Stools become progressively looser as day progresses Nearly all will develop normal bowel patterns by 4 yrs of age

50
Toddler’s Diarrhea Sometimes due to excessive intake of fruit juice
Improves if intake is decreased No other dietary modification needed

51
Diarrhea—questions?

Similar presentations