Download presentation
Presentation is loading. Please wait.

1
Sexual Health for Youth with Spina Bifida
Veronica Meneses MD, MSHS TSRHC

3
Dimensions of Sexuality
Physical Psychological Emotional Social/Cultural Spiritual Important for ALL individuals…beyond medical diagnosis or disability

4
Maslow’s Hierarchy of Human Needs

5
Learning Goals Talk to your youth about sexuality
Identify emergence of sexuality from infancy Describe typical stages of adolescence, puberty

6
Learning Goals Discuss myths about sexuality of youth with disabilities Characterize sexual development of youth with Spina Bifida -Physical Aspects and Health care needs -Social, Emotional, and Psychological functioning -Safety -Spirituality

7
From the Beginning… Humans are sexual beings from birth on
Masturbation is typical in infants May look like abdominal pain, seizures, movement disorders Infant may have irregular breathing, vocalizations, quiet grunting, facial flushing, sweating, hand movements Male infants may have erections during diapering Boorstein 2010

9
Children Ages 2-6 Positive feelings about sexuality can develop from early childhood (Labhard et al. 2010) Parents, caregivers, teachers, doctors influence how child feels about body, feelings, behaviors Model respect, privacy Reassure about body parts and functions

10
Common, Typical Sexual Behaviors in Children ages 2-6
Touching genitals, masturbation in public or private Looking at or touching peer’s or new sibling’s genitals Showing genitals to peers Standing or sitting too close Trying to look at nude peers or adults Kellogg, 2009

11
Less Usual, but still ok, for children ages 2-6
Rubbing body against another Trying to “tongue” kiss Touching genitals of peer or adult Crude imitation of movements associated with sexual acts Behaviors may sometimes disrupt others, but not persistently Temporary, usually respond to distraction Kellogg 2009

12
What does a young child know about sex?
Little sexual knowledge Basic knowledge: gender identity, genital differences, sexual body parts, non-sexual functions of genitals (pregnancy, birth, breast feeding) Knowingly or unknowingly, parents and caregivers are “getting them up to speed” by words, actions, reactions Brilleslijper-Kater 2000
 Knowingly or unknowingly, parents and caregivers are getting them up to speed by words, actions, reactions. Brilleslijper-Kater")
13
Sexual Knowledge in Young Children
By age 5-6, has limited knowledge of pregnancy, birth, reproduction, adult sexual behavior In children with learning challenges or intellectual disability, this may develop at different chronological age Boorstein 2010

14
Be open and honest, tailor to developmental level Stay calm and cool
What Parents Can Do Be open and honest, tailor to developmental level Stay calm and cool Gentle guidance Redirection and limit-setting Kellogg, 2009

16
Middle Childhood: Ages 5-8
Name each body part and its function Boys: nipples, penis, scrotum, testicles Girls: breasts, nipples, vulva, clitoris, vagina, uterus, ovaries Boys and girls: their body parts feel good when touched

17
Middle Childhood With each birthday, your body changes!
You will have many physical changes and become a teenager at puberty You must reach puberty to be able to have children

18
Middle Childhood Sperm and egg join to create a baby
Intercourse with penis inside of vagina is usually how they join Pregnancy is when the baby grows inside a woman’s body Babies come out through the vagina and can drink milk from the mother’s breasts Boorstein 2010

19
Stages of Adolescences
Early: ages 11-13 Middle: ages 14-18 Late: ages 19-21 In youth with Neurodevelopmental Differences, puberty may come earlier—”precocious puberty” ….also may come later, especially if condition affects nutrition and physical growth

20
Early Adolescence: Physical Development
Puberty-> Body hair, more perspiration and oil in hair and skin; need deodorant - Girls develop breasts, hips widen, menstruation begins -Boys have growth in penis and testicles, wet dreams, voice deepens Enormous physical growth Greater sexual interest, “crushes, early experimentation” AAP 2008

21
Early Adolescence: Cognitive
Increasing capacity for abstract thought Mostly interested in present time, limited thoughts about future Intellectual interests broaden, become more important Deeper thinking: moral

22
Early Adolescence: Social Emotional
Struggle with forming sense of identity Feel awkward about self and body: “AM I NORMAL?” Discover parents’ imperfections; more conflict with parents Peer group becomes supreme

23
Early Adolescence: Social Emotional
Regress to “childish” behavior, especially when stressed Moods Swing Test rules and limits Interested in privacy more than ever

24
Middle Adolescence: Physical
Complete puberty Girls grow more slowly, boys keep going Explore and experiment with sexuality Seek intense romantic relationships Try serial monagamy

25
Middle Adolescence: Cognitive
Continue to gain abilities in abstract thinking Set better goals; still do not full understand risks and consequences Interested in moral reasoning Think about: “What is the meaning of life?”

26
Middle Adolescence: Social-Emotional
Intensely involved with Self: change between high expectations and poor self-esteem Take risks, experiment Continue adapting to changing body “I AM STILL NOT SURE IF I AM NORMAL”

27
Middle Adolescence: Social-Emotional
Tend to distance selves from parents, drive for independence Set on making friends and rely on them more, popularity is key Feel love and passion

28
Late Adolescence: Physical
Young women usually reach full development Young men keep growing in height, weight, muscle mass, body hair Accept and enjoy sexual self with greater maturity

29
Late Adolescence: Cognitive
Think ideas through Delay gratification Examine inner experiences More concerned for future Continue to care about moral reasoning

30
Late Adolescence: Social-Emotional
Have stronger sense of Self Have more stable emotions Have greater concern for others Are more independent and self-reliant

31
Late Adolescence: Social-Emotional
Still consider peer relationships important Develop more serious relationships See more value in social and cultural tradition Improved communication and decision making skills about sex Adapted from the American Academy of Child and Adolescent’s Facts for Families. © All rights reserved. 2008 Garofalo & Forcier, 2010

32
Special Points about Youth with Spina Bifida
Wide range of cognitive and learning profiles Intellectual Disability may be present Autistic traits may be present Other diagnoses, genetic issues may be present Both over-weight and under-weight may be challenges

33
Myths about Sexuality of Youth with Disabilities (Intellectual or Physical)
Not able to participate in sexual activities or long-term, satisfying relationships Are not negatively affected by abuse Are asexual: no sexual thoughts, feelings, needs, desires OR Are hypersexual, deviant Campbell 2010

34
More Myths Need protection from society
Teaching about sexuality “will cause more problems” Their sexual behavior is aberrant/wrong

35
Research on Sexuality in Individuals with Developmental Disabilities
Very limited, small number of cases studied Reports from parents, caregivers, professionals Mismatch: -parents report little or no sexual interest except masturbation and flirting - professionals describe higher level of sexual interest and explicit sexual behavior Campbell 2010

36
Considerations for Youth with Spina Bifida
Puberty/sexual development progresses despite diagnosis Hormones trigger feelings, desires, behaviors Cognitive understanding of sexuality may be different than chronological age: Intellectual Disability, learning challenges, or Autistic features Youth may be more sexually mature, understand more, in some areas than others

37
Precocious Puberty More common in females
May begin menstruating 1 ½ - 2 years before peers Bone Age scan and doctor visit Analogues of gonadotropin releasing hormones (leuprolide) may decrease sex hormone levels, stop advancement of puberty and periods, but do not improve adult height (Liptak 2003, Labahrd 2010)
 may decrease sex hormone levels, stop advancement of puberty and periods, but do not improve adult height. (Liptak 2003, Labahrd 2010)")
38
Puberty in Boys Boys may have wet dreams 1 ½ to 2 years before peers
Higher incidence of undescended testicles (cryptorchidism), should be addressed in infancy (Liptak 2003, Labhard 2010)
, should be addressed in infancy. (Liptak 2003, Labhard 2010)")
39
Menstruation Independence in bladder care before periods start is goal
Bowels may be looser->adjust diet and bowel routine Can use pads, tampons, or both May need water soluble lubricant (KY Jelly, Astroglide) to insert tampon (sitting or standing) Change pads/tampons every 4 hours, with CIC, and clean genitals Labhard 2010
 to insert tampon (sitting or standing) Change pads/tampons every 4 hours, with CIC, and clean genitals. Labhard")
40
Management of Menstruation
Painful, irregular periods, behavioral issues: -NSAIDs before symptoms start (correct, scheduled doses) -estrogen/progesterone, progestin -surgical Estrogen contraindicated if youth or family member has history of stroke at early age or inflammatory condition (lupus) Reassurance Hornberger 2010
 -estrogen/progesterone, progestin. -surgical. Estrogen contraindicated if youth or family member has history of stroke at early age or inflammatory condition (lupus) Reassurance. Hornberger")
41
Spontaneous Erections
It is okay! Help him cope Remain seated, cover with shirt or book Do not touch self Avoid comments Briefs better than boxers; some pants hide Positioning Boorstein 2010

42
Wet Dreams Can frighten or embarrass
Reassure and explain that it is normal Prepare for this using language he can understand Teach specifics of self-care: changing pajamas, sheets, washing Boorstein 2010

43
Hygiene Emphasize importance of bath, shower, deodorant according to level of understanding As youth gets older, urine and bowel odor become less socially acceptable and may result in bullying, social isolation Independence in bladder and bowel routines promotes self-esteem and social acceptance Consider fine motor skills, adaptive and therapy needs Labhard 2010, Boorstein 2010

44
Physical Aspects of Sexuality for Youth with Spina Bifida
Males and females have decreased sensation in perineum and may have problems experiencing orgasm (higher lesions) Body may make up for lack of sensation in one area by increasing it in another area: nipple line, back of neck/ears, shoulders, elbows, armpits Develop awareness of sensitive areas with partner Liptak 2003; Labhard 2010
 Body may make up for lack of sensation in one area by increasing it in another area: nipple line, back of neck/ears, shoulders, elbows, armpits. Develop awareness of sensitive areas with partner. Liptak 2003; Labhard")
45
Physical Aspects About 75% of males can have erection
The lower the lesion the more likely that erection possible May not be able to sustain Sometimes semen may go backwards into bladder Erection aides: Viagra Couple may explore other ways to have sexual pleasure other than act of intercourse Liptak 2003; Labhard 2010

46
Physical Aspects Females with spina bifida have normal fertility and can have children Males may have fertility challenges but should assume they are fertile unless medical tests show they are not Electroejaculation may be used in men wih spinal cord injury: nerves of penis are electrically stimulated, sperm obtained and used for artificial insemination Labhard 2010

47
Sexual Activity: Planning is Important
Males and females: apply water-based or silicone based lubricant to genital areas before and during intercourse to avoid pressure ulcers and skin irritation Good hygiene prevents urinary infections Wash and empty bladder and bowel before sex Empty bladder again after sex Labhard 2010

48
Birth Control Hormonal: Birth control pills, injections, implants
Barrier: Diaphagms, Latex-free polyurethane condoms (latex allergies) Surgical Procedures: Tubal ligation, Vasectomy Labhard 2010
 Surgical Procedures: Tubal ligation, Vasectomy. Labhard")
49
Sexually Transmitted Infections
Gonorrhea, Chlamydia, HIV/AIDs, Hepatitis Polyurethane condoms are best protection for those who are sexually active Learn partner’s history, risks, testing as needed

50
Pregnancy Take Folic Acid: 4000 mcg daily for 1-3 months before trying to conceive Keep a healthy weight Talk with physicians to make sure her medications safe during pregnancy Avoid urinary tract infections (early labor and premature birth) Use home monitor device if unable to feel contractions Labhard 2010
 Use home monitor device if unable to feel contractions. Labhard")
51
Genetic Counseling If either partner has spina bifida, there is 3-5% chance of having child with spina bifida Important to consider what raising a child will mean Folic acid reduces risk Labhard 2010

52
Female Clinic Visits Does obstetrician-gynecologist or other physician have knowledge and experience about spina bifida? Are clinics accessible? Avoid positioning with stirrups Labhard 2010

53
When there is Intellectual Disability
Sexual expression may be like that of a younger child and this is normal (masturbation, crushes) May be impulsive and concrete Desires may be strong with few outlets May have little interaction with peers with ID May feel rejected in inclusive settings Boorstein 2010
 May be impulsive and concrete. Desires may be strong with few outlets. May have little interaction with peers with ID. May feel rejected in inclusive settings. Boorstein")
54
Sex Education for Youth with Spina Bifida with Intellectual Disability
Learn boundaries, modesty in social settings Switch from hugs to high fives early on Teach to cognitive and social level, culture Explicitly teach about who, when, where can touch private areas Model respect, privacy Use concrete instruction, multiple media, check comprehension and repeat Harris 2010

55
Noverbal Learning Problems and other Learning Issues
May need guidance remembering, planning, organizing self-care around sexual health and activitiy May also need concrete, visual educational methods Assessing comprehension is important

56
When There are Autistic Traits
Lack typical awareness of personal space/boundaries (socially learned) Social interests without good skills (miss cues) Rigid Behaviors may be seen as “stalking” Immaturity, Legal problems may arise Internet/social media may be used inappropriately (pornography) Boorstein 2010
 Social interests without good skills (miss cues) Rigid Behaviors may be seen as stalking Immaturity, Legal problems may arise. Internet/social media may be used inappropriately (pornography) Boorstein")
57
Sex Education for Youth with Spina Bifida who have Autisic Traits
Directly teach social rules and norms Adjust to cognitive and functional level Help understand emotions, impulses May need to cover sexual orientation and gender identity Individual Instruction is brief, concrete, specific, visual, in real-life context, repeat frequently Cambell 2010; Sullivan & Caterino 2008

58
Masturbation Significant concern for families, school
Professionals should explicitly address with youth and family Remember developmental level Redirect, give little attention to if in public Boorstein 2010

59
Masturbation If youth has problems generalizing, understanding social contexts, limit to bedroom/door closed or bathroom/shower Knock if youth’s door closed Harris 2010

60
Orientation No reason to suspect that homosexuality or bisexuality more prevalent in youth with developmental disabilites Mental health support is crucial if there is discrimination, bullying, depression, poor self-esteem

61
Paraphellias/Sexual Fetishes
May occur in both higher and lower functioning individuals May occur slightly more frequently in individuals with autism vs ID Allow fixation with stockings, underwear etc. Use redirection vs elimation Reassure parents and school Attend to safety issues Boorstein 2010

62
Dating Many parents decide age to begin, cultural
Means different things to different people May include shared recreational/leisure activities and social exchange Paying for date does not obligate sexual activity Break-ups create emotional pain, youths need support Campbell 2010

63
Supervised Dating Groups, chaperones, shadows, double dates
Independence according to needs Some youth may progress and be able to be on their own Some will need highly structured settings into adulthood Intimacy does not equate with physical acts Boorstein 2010

64
Cohabitation/Marriage
Possible for adults with spina bifida May require caregiver/parental support, intensity depends on unique needs, functioning Barriers may come from bureaucratic regulations: SSI benfit reduced if married, guardianship legalities, supported living program policies Harris 2010

65
Tips on “The Talk” Start early, before puberty
Use real names for sexual organs Learn with your child…there will always be something new for both to learn Be honest, direct, matter-of-fact Begin where child’s understanding—and interest– is (masturbation, kissing, body changes)
")
66
Tips Listen to and ACCEPT child’s feelings
Let child know it is safe to be open with you and normal for people with spina bifida to have sexual needs Teach as you go through daily life (not preach) Bring up and discuss important topics Role-play to prevent abusive situations: physically, sexually, verbally, emotionally Labhard 2010
 Bring up and discuss important topics. Role-play to prevent abusive situations: physically, sexually, verbally, emotionally. Labhard")
67
Sex Education in U.S. Schools
General Requirements: Sex Education and HIV Education 22 states and the District of Columbia mandate sex education 20 states and the District of Columbia mandate both sex education and HIV education 2 states only mandate sex education

69
New National Standards
January 2012: first-ever national standards for sexuality education in public schools published in the Journal of School Health Be Age and Developmentally Appropriate Focus on social and personal competence Minimum, essential content given for K-12

70
Seven Content Areas Anatomy & Physiology
Puberty & Adolescent Development Identity Pregnancy & Reproduction, Sexually Transmitted Diseases & HIV Healthy Relationships Personal Safety

71
FYI: Texas No Mandate for Sex or HIV Education When provided must be
-age appropriate -stress abstinence -include information on importance of sex only within marriage Requires only negative information on sexual orientation

72
FYI: Texas When sex/HIV education is provided: -parent must be notified (do not have to consent) -parent can opt-out
 -parent can opt-out")
73
Advocacy Know your state’s mandates: helps you advocate for your youth
Speak for youth’s and family’s needs and values Make it Part of ARD/IEP

74
Vulnerable to Abuse Strong reliance on others for self-care needs
Mobility/access problems Cognitive and Social Differences Communication Challenges Multiple caregivers Learned compliance Trouble knowing forced sex from consensual sex Campbell 2010, Lambhard 2010

75
Prevent Abuse Build communication/language, mobility
Build knowledge, self-esteem, independence Youth who is independent in bladder and bowel routines will need less intimate care-giving Ask about it, will not cause it Know caregivers, limit number Teach about healthy relationships, avoid isolation

76
Report Abuse National Sexual Assault Hotline, open 24 hours per day, 7 days per week You do not need all the facts, details Doctors, Schools, Churches can help Counseling/Mental Health Support is top priority, regardless of cognitive level or type of physical disability Labhard 2010

77
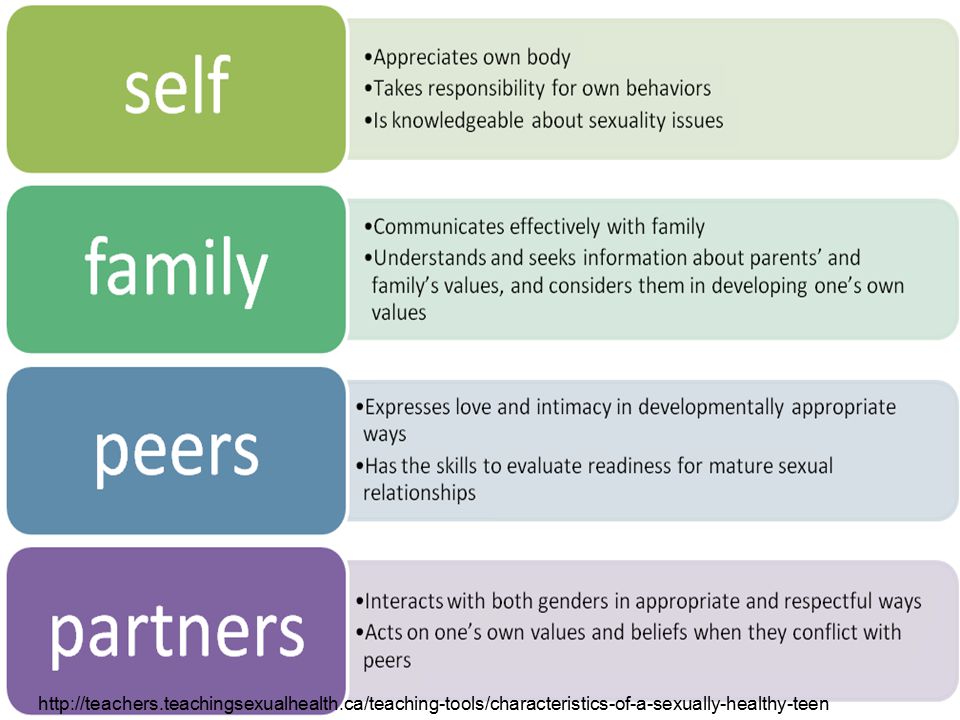
http://teachers. teachingsexualhealth
78
References Boorstein et al SDBP 2010 Workshop Puberty and Sexuality for Youth with Developmental Disabilites and their Families Labhard et al 2010 Sexuality and Spina Bifida Spina Bifida Association 2006, Health Guide for Parents of Children Living with Spina Bifida Brilleslijper-Kater 2000 Servais Kellogg 2009 Koller 2000

Similar presentations












 Chisenhale Primary School.>")









