Download presentation
Presentation is loading. Please wait.

1
Meeting 6 Disease Manifestations Virulence Factors Antimicrobial resistance
1 Aug 2009

2
Manifestations of infectious disease
Classic Signs Fever, swelling, rashes, vomiting, diarrhea Skin signs: lesions, erythema, papule (pimple), vesicles, pustule, ulcer or erosion or abscess Symptoms Pain, headache, nausea, malais Inflammation Result of Immune reactions Hematologic ( leukocytosis, anemia ) Cardiac (tachycardia to heart failure) Respiratory (hyperventilation) Renal Hepatic Upper GI bleeding
, vesicles, pustule, ulcer or erosion or abscess. Symptoms. Pain, headache, nausea, malais. Inflammation. Result of Immune reactions. Hematologic ( leukocytosis, anemia ) Cardiac (tachycardia to heart failure) Respiratory (hyperventilation) Renal. Hepatic. Upper GI bleeding.")
3
Manifestations of infectious disease
Table 1 Types of skin lesions Flat lesions (in the plane of the skin) Elevated lesions (above the plane of the skin) Depressed lesions (below the plane of the skin) Macule IInfarct Sclerosis• Telangiectasis† Vesicle and bulla Pustule Abscess‡ Cyst‡ Papule Wheal plague Nodule‡ Vegetation Keratosis Desquamation (scales) Exudate• (crusts) Lichenification Atrophy§ Sclerosis§ Erosion Excoriation Scar† Ulcer Sinus‡ Gangrene§ • May also be below the plane of skin † May also be above the plane of skin ‡ May also be in or below the plane of skin § May also be in the plane of skin Classic Signs Fever, swelling, rashes, vomiting, diarrhea Skin signs: lesions, erythema, papule (pimple), vesicles, pustule, ulcer or erosion or abscess Symptoms Pain, headache, nausea, malaise Inflammation
 Elevated lesions (above the plane of the skin) Depressed lesions (below the plane of the skin) Macule IInfarct Sclerosis• Telangiectasis† Vesicle and bulla Pustule Abscess‡ Cyst‡ Papule Wheal plague Nodule‡ Vegetation Keratosis Desquamation (scales) Exudate• (crusts) Lichenification. Atrophy§ Sclerosis§ Erosion Excoriation Scar† Ulcer Sinus‡ Gangrene§ • May also be below the plane of skin † May also be above the plane of skin ‡ May also be in or below the plane of skin § May also be in the plane of skin. Classic. Signs. Fever, swelling, rashes, vomiting, diarrhea. Skin signs: lesions, erythema, papule (pimple), vesicles, pustule, ulcer or erosion or abscess. Symptoms. Pain, headache, nausea, malaise. Inflammation.")
4
Flat lesion MACULE A macule is a change in the color of the skin. It is flat, if you were to close your eyes and run your fingers over the surface of a purely macular lesion, you could not detect it. A macule greater than 1 cm. may be referred to as a patch.

5
Elevated lesion PAPULE
is a solid raised lesion that has distinct borders and is less than 1 cm in diameter. Papules may have a variety of shapes in profile (domed, flat-topped, umbilicated) and may be associated with secondary features such as crusts or scales.
 and may be associated with secondary features such as crusts or scales.")
6
Elevated lesion TUMOR is a solid mass of the skin or subcutaneous tissue; it is larger than a nodule.

7
Elevated lesion PAPULE
is a solid raised lesion that has distinct borders and is less than 1 cm in diameter. Papules may have a variety of shapes in profile (domed, flat-topped, umbilicated) and may be associated with secondary features such as crusts or scales.
 and may be associated with secondary features such as crusts or scales.")
8
Depressed lesion ATROPHY
Atrophy is thinning or absence of the epidermis or subcutaneous fat.

9
Depressed lesion EROSION
Erosions are slightly depressed areas of skin in which part or all of the epidermis has been lost

10
Depressed lesion ULCERATION
occur when there is necrosis of the epidermis and dermis and sometimes of the underlying subcutaneous tissue.

11
FEVER 1. Fever increases the environmental temperature above the optimum growth temperature for many microorganisms. If the microorganisms are growing more slowly, the body's defenses have a better chance of removing them all. 2. Fever leads to the production of heat shock proteins that are recognized by some intraepithelial T-lymphocytes (delta gamma T-cells) resulting in the production of inflammation-promoting cytokines. 3. Fever elevates the temperature of the body increasing the rate of enzyme reactions, and speeding up metabolism within the body. can increase the production and activity of phagocytes, speed up the multiplication of lymphocytes, increase the rate of antibody and cytokine production, increase the rate at which leukocytes are released from the bone marrow into the bloodstream, and speed up tissue repair. Too high of a body temperature, however, may cause damage by denaturing the body's enzymes.
 resulting in the production of inflammation-promoting cytokines. 3. Fever elevates the temperature of the body increasing the rate of enzyme reactions, and speeding up metabolism within the body. can increase the production and activity of phagocytes, speed up the multiplication of lymphocytes, increase the rate of antibody and cytokine production, increase the rate at which leukocytes are released from the bone marrow into the bloodstream, and speed up tissue repair. Too high of a body temperature, however, may cause damage by denaturing the body s enzymes.")
12
FEVER Fever may have certain signs in relation to its course.
Fever in infectious diseases usually is of short duration Long duration (weeks or months) is always a very serious problem. If it is not possible to determine the cause of fever at the beginning, it is called the fever of unknown origin (FUO). This term is used to describe fever lasting at least 2 weeks, reaching temperatures above 38,2 , and the cause of the origin is uncertain. Fever may last long in some infections with subacute or chronic course.
 is always a very serious problem. If it is not possible to determine the cause of fever at the beginning, it is called the fever of unknown origin (FUO). This term is used to describe fever lasting at least 2 weeks, reaching temperatures above 38,2 , and the cause of the origin is uncertain. Fever may last long in some infections with subacute or chronic course.")
13
Stages in the Progression of Disease
No signs or symptoms Prodormal illness Mild signs or symptoms Some chilling occur Acute identifiable signs and symptoms Intermittent fever Recovery Action of immune system Action of antibiotics Convalescence

14
Stages in the Progression of Disease

17
Manifestations of infectious disease
Result of Immune reactions Hematologic ( leukocytosis, anemia ) Cardiac (tachycardia to heart failure) Respiratory (hyperventilation) Renal Hepatic Upper GI bleeding
 Cardiac (tachycardia to heart failure) Respiratory (hyperventilation) Renal. Hepatic. Upper GI bleeding.")
18
Case study 1 S. T. was seen by you in the Emergency Room in December
23 y/o medical student in Southern California c/o sudden onset of fever, chills, malaise, headache, myalgia, sore throat, runny nose, sneezing Room-mate has same symptoms Exam: erythematous, inflammed tonsils, no pharyngeal exudates Throat culture: Group A streptococci

19
Case study 1 erythematous, inflammed tonsils

20
Case study 2 P. A. is a patient in the Intensive Care Unit 65 y/o man
Intubated, on respirator: good oxygenation Nurse says that he hasn’t had fever or purulent sputum Exam: clear breath sounds, no rhonchi nor rales CXR: clear without infiltrates or effusions Sputum Gram stain: mixed flora with Gram positive cocci; thin, long Gram negative rods Sputum culture: normal respiratory flora, Pseudomonas aeruginosa

21
Case study 3 T. M. was referred to you by the Public Health Department
38 y/o woman Private cook in Manhattan In the past 10 years, 7 of the 8 families she has worked for have had outbreaks of illness: Fever, malaise, headache, myalgia, maculopapular rash, bradycardia, constipation, bloody diarrhea T. M. denies h/o similar illness and denies current symptoms “But, Doctor, I’m not sick!”

22
Case study 3 maculopapular rash

23
Disease state: complex interaction between pathogen and host
1. If a bacterium is present, is it causing disease? a. Normal flora b. Colonization c. Carrier state d. Infection: i. Asymptomatic ii. Symptomatic 2. Is the bacterium capable of causing disease? a. Nonpathogen b. Opportunistic pathogen c. Primary pathogen

24
Case study 1: Viral pharyngitis + Group A strep normal respiratory flora
S. T. was seen by you in the Emergency Room in December 23 y/o medical student in Southern California c/o sudden onset of fever, chills, malaise, headache, myalgia, sore throat, runny nose, sneezing Room-mate has same symptoms Exam: erythematous, inflammed tonsils, no pharyngeal exudates Throat culture: Group A streptococci

25
Case study 2: Colonization with Pseudomonas aeruginosa
P. A. is a patient in the Intensive Care Unit 65 y/o man Intubated, on respirator: good oxygenation Nurse says that he hasn’t had fever or purulent sputum Exam: clear breath sounds, no rhonchi nor rales CXR: clear without infiltrates or effusions Sputum Gram stain: mixed flora with Gram positive cocci; thin, long Gram negative rods Sputum culture: normal respiratory flora, Pseudomonas aeruginosa

26
Case study 3: Typhoid Mary Salmonella typhi carrier
T. M. was referred to you by the Public Health Department 38 y/o woman Private cook in Manhattan In the past 10 years, 7 of the 8 families she has worked for have had outbreaks of illness: Fever, malaise, headache, myalgia, maculopapular rash, bradycardia, constipation, bloody diarrhea T. M. denies h/o similar illness and denies current symptoms “But, Doctor, I’m not sick!”

27
Outbreak 2001

30
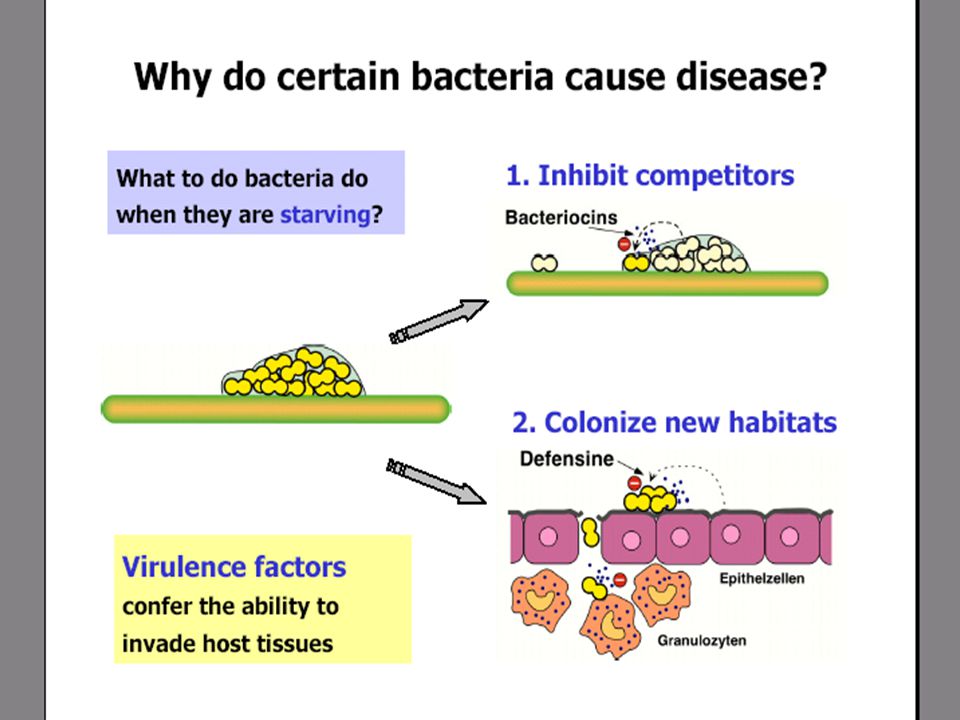
Virulence Factors that Promote Colonization and Invasion
Virulence factors that damage the host Exotoxins Endotoxins Ability to resist innate immunity Ability to evade adaptive immunity Ability to induce autoimmune response

31
Virulence Factors that Promote Colonization and Invasion
Basic requirements: receptor + adhesin Receptor Specific carbohydrate or peptide residues on the cell surface Adhesin or adherence factor A macromolecular component of the bacterial cell surface interacting to the receptor

32
Virulence Factors that Promote Colonization and Invasion
Surface proteins called adhesins in the bacterial cell wall bind to receptor molecules on the surface of a susceptible host cell enabling the bacterium to make intimate contact with the host cell, adhere, colonize, and resist flushing.

33
Virulence Factors that Promote Colonization and Invasion
Specific adherence of bacteria to cell and tissue surfaces Tissue tropism Strep mutans in dental plaque but not in the tongue Species specificity Neisseria gonorrheae limited to humans Genetic specificity within a species Mechanism of specific adherence Reversible attachment – “docking” Non-reversible attachment – “anchoring”

34
Virulence Factors that Promote Colonization and Invasion: Example
(Tabulate according to the ff: Bacterium:Adherence Factor:Receptor (optional):Attachment Site: Disease) Streptococcus pyogenes: Protein F Aminoterminus of fibronectin Pharyngeal Epithelium Sore Throat
:Attachment Site: Disease) Streptococcus pyogenes: Protein F. Aminoterminus of fibronectin. Pharyngeal Epithelium. Sore Throat.")
35
S. pyogenes F-protein lipoteichoic acid fibronectin

36
Virulence Factors that Promote Colonization and Invasion:
Fimbriae Adhesins Protein F Capsules Invasins Cleaves secretory IgA (Glycosyl transferase) Spreading factors: Hyaluronidase – attacks the interstitial cement of connective tissue by depolymerizing hyaluronic acid Collagenase Neuraminidase Streptokinase and staphylokinase Siderophores Low molecular weight compounds that chelate iron with very high affinity Competing for iron and other nutrients
 Spreading factors: Hyaluronidase – attacks the interstitial cement of connective tissue by depolymerizing hyaluronic acid. Collagenase. Neuraminidase. Streptokinase and staphylokinase. Siderophores. Low molecular weight compounds that chelate iron with very high affinity. Competing for iron and other nutrients.")
37
Virulence Factors that Promote Colonization and Invasion

38
Virulence Factors that Promote Colonization and Invasion

39
Virulence Factors that Promote Colonization and Invasion
Glycocalyx Polysaccharide or peptide slime Capsule Slime layer Functions: Resists phagocytosis Enhanced attachment

40
Virulence Factors that Promote Colonization and Invasion
A proposed model for invasion of epithelial cells of the colon. 1) The Shigella first cross the mucosa by passing through specialized cells called M cells. The M cell passes the Shigella on to a macrophage from which it subsequently escapes - possibly by inducing apoptosis, a programmed cell suicide. 2) The Shigella then uses its invasins to enter the mucosal epithelial cells from underneath. The invasins cause actin polymer rearrangements in the cell's cytoskeleton resulting in the bacterium being engulfed and placed in an endocytic vesicle in a manner similar to phagocytic cells. Once inside, the Shigella escape from the vacuole into the cytoplasm and multiply. 3) The Shigella are able to move through the host cell and spread to adjacent host cells by a unique process called actin-based motility. In this process, actin filaments polymerize at one end of the bacterium, producing comet-like tails that propel the Shigella through the cytoplasm of the host cell. 4) When they reach the boundary of that cell, the actin filaments push the Shigella across that membrane and into the adjacent cell. Shigella Passing Through the Mucous Membrane and Invading Mucosal Epithelial Cells
 The Shigella first cross the mucosa by passing through specialized cells called M cells. The M cell passes the Shigella on to a macrophage from which it subsequently escapes - possibly by inducing apoptosis, a programmed cell suicide. 2) The Shigella then uses its invasins to enter the mucosal epithelial cells from underneath. The invasins cause actin polymer rearrangements in the cell s cytoskeleton resulting in the bacterium being engulfed and placed in an endocytic vesicle in a manner similar to phagocytic cells. Once inside, the Shigella escape from the vacuole into the cytoplasm and multiply. 3) The Shigella are able to move through the host cell and spread to adjacent host cells by a unique process called actin-based motility. In this process, actin filaments polymerize at one end of the bacterium, producing comet-like tails that propel the Shigella through the cytoplasm of the host cell. 4) When they reach the boundary of that cell, the actin filaments push the Shigella across that membrane and into the adjacent cell. Shigella Passing Through the Mucous Membrane and Invading Mucosal Epithelial Cells.")
41
Virulence Factors that Promote Damage to the Host: EXOTOXINS
Properties Secreted during exponential growth Protein toxins High biological activity Exhibits specificity of action Components A = active B = binding

42
A-B toxins Cell surface Active Binding A B

43
Binding and Entry of an A-B Toxin
A-B toxins consist of two parts, an A (active) component and a B (binding) component. The B component of the exotoxin binds to a receptor on the surface of a susceptible host cell. The exotoxin now enters the host cell, in this case by endocytosis, and causes harm by inactivating a host cell target protein through ADP-ribosylation.
 component and a B (binding) component. The B component of the exotoxin binds to a receptor on the surface of a susceptible host cell. The exotoxin now enters the host cell, in this case by endocytosis, and causes harm by inactivating a host cell target protein through ADP-ribosylation.")
44
Virulence Factors that Promote Damage to the Host: EXOTOXINS
Based on structure A-B prototype Botulinum toxin, diphtheria toxin, shiga toxin, tetanus toxin Membrane disrupting toxin Lacks A & B Pore forming Phospholipase Superantigens

45
Superantigens 1. Some exotoxins are superantigens
2. Produced by bacteria and viruses 3. Action: polyclonal stimulation of subset of lymphocytes to divide and produce cytokines 4. Best known example: Staph Toxic Shock Syndrome Toxin-1 (TSST-1) 5. Also Strep exotoxins 6. Pyrogenic toxins cause fever (unlike other exotoxins)
 5. Also Strep exotoxins. 6. Pyrogenic toxins cause fever (unlike other exotoxins)")
46
2-subunit A-B exotoxin Neurotoxin: Clostridium botulinum
Murray, P.R. et al. Medical Microbiology, 3rd edition, 1998, p. 156

47
Botulism Exotoxin Blocking Acetylcholine Release
The botulism exotoxin binds to the presynaptic neuron and blocks its release of acetylcholine. This causes a flaccid paralysis, a weakening of the involved muscles.

48
Membrane damaging exotoxins
Proteases Phospholipases Detergent-like action

49
Virulence Factors that Promote Damage to the Host: EXOTOXINS
Based on modes of action Breaks down cells Alpha toxins, hemolysins, leukocidins Enhance microbial spread Spreading factors: hyaluronidase, mucinase etc Interfere in cellular metabolism Tetanus toxin, botulinum toxin

50
Virulence Factors that Promote Damage to the Host: EXOTOXINS
3 ways this can contribute to the progression of disease: Ingestion of preformed toxin Colonization of wound or mucosal surface followed by exotoxin production Colonization of wound followed by local exotoxin production

51
Neutralization of Exotoxins

52
Evasion of host immune response: IgA protease
1. Cleaves IgA, which is important for mucosal immunity 2. An enzyme produced by Neisseria gonorrhoeae, Neisseria meningitidis, Haemophilus influenzae, Streptococcus pneumoniae

53
Requirement for iron 1. Most iron in the body is intracellular
In hemoglobin and myoglobin 2. There is very little free iron Extracellular iron is bound to transferrin (in plasma) and lactoferrin (in milk and other secretions) 3. Some bacteria produce siderophores to capture iron e.g. Escherichia coli Siderophores bind iron with high affinity
 and lactoferrin (in milk and other secretions) 3. Some bacteria produce siderophores to capture iron e.g. Escherichia coli. Siderophores bind iron with high affinity.")
54
Virulence Factors that Promote Damage to the Host: ENDOTOXINS
Outer membrane of the gram negative cell wall Lipid A:polysaccharide:O antigen Toxicity is associated with Lipid A Immunogenicity is associated with the polysaccharide component Less potent, less specific Does not form antitoxin Released when the bacterial cell is damaged

55
Periplasmic binding protein
GRAM NEGATIVE CELL ENVELOPE Outer Membrane (Major permeability barrier) Lipopolysaccharide Porin Braun lipoprotein Periplasmic space Degradative enzyme Periplasmic binding protein Permease Inner (cytoplasmic) membrane Cytoplasm
 Lipopolysaccharide. Porin. Braun lipoprotein. Periplasmic space. Degradative enzyme. Periplasmic binding protein. Permease. Inner (cytoplasmic) membrane. Cytoplasm.")
56
Septic shock Septic shock hypotension (tissue pooling of fluids)
disseminated intravascular coagulation fever lack of effective oxygenation overall system failure Septicemia

57
Exotoxin vs Endotoxin

58
Bacterial Pathogenesis
1. Microbial pathogens and their hosts have often co-evolved 2. Clinical disease a. Non-adapted host/pathogen b. May promote pathogen’s survival and transmission c. Can result from host response to pathogen 3. Extracellular bacteria produce toxins and enzymes

59
Bacterial Pathogenesis
4. Bacteria secrete proteins into host cells to modify host cell function 5. Intracellular bacteria must bind, enter and survive inside host cells 6. Pathogenic bacteria can evade the host immune response and have mechanisms for antibiotic resistance 7. Expression of virulence factors is often regulated in response to the environment and other signals

60
Bacterial Pathogenesis: Concepts
1. Virulence genes that encode virulence factors A virulence gene confers on a bacterium the ability to cause disease Pathogenic strains have acquired virulence genes that allow them to exploit the host as an environmental niche Examples of virulence factors are toxins, enzymes, type III secreted proteins, adhesins, siderophores Virulence factors are obvious targets for prevention or treatment strategies

61
Bacterial Pathogenesis: Concepts
2. Bacteria have found many way to modulate host cell function Exotoxins and type III secreted proteins are virulence factors with specific functions such as to kill host cells or induce the uptake of bacteria by the host cell Knowledge of these mechanisms can help explain the clinical disease caused by a particular bacterium, and the basis for prevention and treatment strategies

62
Bacterial Pathogenesis: Concepts
3. Toxins vs. toxoids vs. antitoxin (antitoxoid) Toxins are made by bacteria and have harmful effects on host cells A toxoid is the inactivated form of an exotoxin that can be used as a vaccine to elicit an immune response Toxoids were traditionally inactivated by heat or formaldehyde, but now can be genetically engineered Antitoxin is the antisera produced in response to the toxoid (can be from animals or humans) and can be given as treatment
 Toxins are made by bacteria and have harmful effects on host cells. A toxoid is the inactivated form of an exotoxin that can be used as a vaccine to elicit an immune response. Toxoids were traditionally inactivated by heat or formaldehyde, but now can be genetically engineered. Antitoxin is the antisera produced in response to the toxoid (can be from animals or humans) and can be given as treatment.")
63
Bacterial Pathogenesis: Concepts
4. Mechanisms of pathogenesis are conserved among bacteria Virulence genes that provide a selective advantage are spread among different bacterial genera and species by horizontal transfer These virulence genes are often located on mobile DNA elements such as plasmids or bacteriophages

64
… refresh...

65
Antibiotics Antibiotics and vaccines are among the biggest medical advances since (Culver Pictures) For lecture only BC Yang

66
A brief history of antibiotics
1495, mercury to treat syphilis. 1630, quinine (chinchona tree) for malarial fever by South American Indians. 1889, Buillemin defined antibiosis. 1910, Paul Ehrlich developed arsenical compound (Salvarsan) for syphilis, term: the chemical knife. 1929, Alexander Fleming found penicillin. 1935, Gerhard Domagk showed the value of sulfonamides. 1940, Ernst Chain and Howard Flory demonstrated the effect of penicillin. , then searching for new antibiotics ~ recent year: modifying old drugs, finding new discipline in antibacterial combats Early time in war: thanks penicillin, we can go home now Now a day……….Oh eh?!
 for malarial fever by South American Indians. 1889, Buillemin defined antibiosis. 1910, Paul Ehrlich developed arsenical compound (Salvarsan) for syphilis, term: the chemical knife. 1929, Alexander Fleming found penicillin. 1935, Gerhard Domagk showed the value of sulfonamides. 1940, Ernst Chain and Howard Flory demonstrated the effect of penicillin , then searching for new antibiotics. ~ recent year: modifying old drugs, finding new discipline in antibacterial combats. Early time in war: thanks penicillin, we can go home now. Now a day……….Oh eh !")
67
Thanks to work by Alexander Fleming ( ), Howard Florey ( ) and Ernst Chain ( ), penicillin was first produced on a large scale for human use in At this time, the development of a pill that could reliably kill bacteria was a remarkable development and many lives were saved during World War II because this medication was available. E. Chain H. Florey A. Fleming

68
A tale by A. Fleming He took a sample of the mold from the contaminated plate. He found that it was from the penicillium family, later specified as Penicillium notatum. Fleming presented his findings in 1929, but they raised little interest. He published a report on penicillin and its potential uses in the British Journal of Experimental Pathology.

69
An ideal antibiotic Broad-spectrum Does not induce resistance
Selective toxicity, low side effects Preserve normal microbial flora

70
Definitions Antimicrobial Antibacterial Antibiotic
Inhibits growth of micro-organisms Antibacterial Inhibits growth of bacteria Antibiotic Made by other micro-organisms Usually extended to include synthetic drugs

71
Susceptibility test Tube dilution method Disk diffusion method
Minimal inhibitory concentration (MIC): the smallest amount of chemotherapeutic agent required to inhibit the growth of organism in vitro Disk diffusion method Zone of inhibition (ZOI): the correlation of ZOI and MIC has been established by FAD ETest. This commercially-prepared strip creates a gradient of antibiotic concentration when placed on an agar plate
: the smallest amount of chemotherapeutic agent required to inhibit the growth of organism in vitro. Disk diffusion method. Zone of inhibition (ZOI): the correlation of ZOI and MIC has been established by FAD. ETest. This commercially-prepared strip creates a gradient of antibiotic concentration when placed on an agar plate.")
72
Bacteriostatic vs Bactericidal
Reversible inhibition of growth When the antibiotic is removed, almost all of the bacteria can replicate Bactericidal Irreversible inhibition of growth When the antibiotic is removed, almost none of the bacteria (10-7 to 10-3) can replicate
 can replicate.")
73
Guidance of antimicrobial therapy
Minimum inhibitory concentration: lowest concentration of antibiotic that inhibits visible growth Minimum bactericidal concentration: lowest concentration of antibiotic that kills 99.9% of the inoculum Serum bactericidal title: dilution of serum that kills 99.9% of the inoculum Synergy test: synergistic activity of multiple antibiotics

74
Use of antibiotics; is it properly applied?
Acute infections in outpatients Acute infections in hospitalized patients Chronic infection (tuberculosis, AIDS) Agriculture/veterinary medicine
 Agriculture/veterinary medicine.")
75
In vitro: Factors for optimal antibiotic action
pH of environment: Nitrofurantoin is more active in acid pH; sulfonamides and aminoglycoside are more active in alkaline pH. Components of medium: Anionic detergents inhibit aminoglycosides, serum proteins bind to penicillin in varying degrees. Stability of drug: Aminoglycosides and chloramphenical are stable for long period in vivo. Size of inoculums: The larger the bacterial inoculum, the greater the chance for resistnat mutant to emerge. Metablic activity of microorganisms: Actively and rapidly growing organisms are more susceptible to drug action BC Yang

76
Affecting factors in vivo
Abscess: circulation is blocked off. Foreign bodies: obstruction of the urinary, biliary or respiratory tracts etc. Immunity.

77
Sites of action BC Yang

78
Modes of action (1) Inhibitors of cell wall synthesis. Penicillins, cephalosporin, bacitracin, carbapenems and vancomycin. Inhibitors of Cell Membrane. Polyenes - Amphotericin B, nystatin, and condicidin. Imidazole - Miconazole, ketoconazole and clotrimazole. Polymixin E and B. Inhibitors of Protein Synthesis. Aminoglycosides - Streptomycin, gentamicin, neomycin and kanamycin. Tetracyclines - Chlortetracycline, oxytetracycline, doxycycline and minocycline. Erythromycin, lincomycin, chloramphenicol and clindamycin. vancomycin Amphotericin Aminoglycosides Tetracyclines For lecture only BC Yang

79
Modes of action (2) Inhibitors of metabolites (Antimetabolites). Sulfonamides - Sulfanilamide, sulfadiazine silver and sulfamethoxazole. Trimethoprim, ethambutol, isoniazid. Inhibitors of nucleic acids (DNA/RNA polymerase). Quinolones - Nalidixic acid, norfloxacin and ciprofloxacin. Rifamycin and flucytosine. rifamycin For lecture only BC Yang
. Sulfonamides - Sulfanilamide, sulfadiazine silver and sulfamethoxazole. Trimethoprim, ethambutol, isoniazid. Inhibitors of nucleic acids (DNA/RNA polymerase). Quinolones - Nalidixic acid, norfloxacin and ciprofloxacin. Rifamycin and flucytosine. rifamycin. For lecture only. BC Yang.")
80
Resistance Natural (inherent) resistance Structural barrel
Lack of target Transport system Acquired resistance Mutation Gene exchange (conjugation in most)
")
81
Transferable antibiotic resistance in bacteria
Reduced uptake into cell (chloramphenicol) Active efflux from cell (tetracycline) Modification of antibiotic targets (b-lactam, erythromycin) inactivation of antibiotic by anzymic modification: hydrolysis (b-lactam, erythromycin); derivatization (aminoglycosides) Sequestration of antibiotic by protein binding (b-lactam) Metabolic bypass (sulfonamides) Overproduction of antibiotic target (titration: sulfonamides)
 Active efflux from cell (tetracycline) Modification of antibiotic targets (b-lactam, erythromycin) inactivation of antibiotic by anzymic modification: hydrolysis (b-lactam, erythromycin); derivatization (aminoglycosides) Sequestration of antibiotic by protein binding (b-lactam) Metabolic bypass (sulfonamides) Overproduction of antibiotic target (titration: sulfonamides)")
82
Spread of resistance In most:
Day-care, nursing homes, correctional facilities Sanitation, animal feeds (fecal-oral) Sexual/ Respiratory transmission International travel Immunosuppression
 Sexual/ Respiratory transmission. International travel. Immunosuppression.")
83
Some probable overuse/misuse of antibiotics
Prophylatic use before surgery Empiric use (blinded use) Increased use of broad spectrum agents Pediatric use for viral infections Patients who do not complete course (chronic disease, eg. TB, AIDS) Antibiotics in animal feeds For lecture only BC Yang
 Increased use of broad spectrum agents. Pediatric use for viral infections. Patients who do not complete course (chronic disease, eg. TB, AIDS) Antibiotics in animal feeds. For lecture only. BC Yang.")
84
Policy to deal drug resistance (1)
Ideally, bacteriological management of clinical infection should involve: Identification of causative organism Sensitivity test Follow-up the drug effect Monitor antibiotic level to avoid toxicity. In reality, most patients requiring antimicrobial therapy are treated empirically. In serious infections immediate chemotherapy may be life-saving.

85
Policy to deal drug resistance (2)
Periodic changes of antibiotics used might change selective pressure and thus avoid the emergence of resistance and retain the therapeutic value of antibiotics over a longer period. The unnecessary prophylactic or animal feeds use should be discouraged. Distribution of information on current/updated infectious microbes (consult microbiologists): use more targeted antibiotics Patient education
: use more targeted antibiotics. Patient education.")
86
New antibiotics development
Pharmaceutical industry putting resources back into discovery Liaisons with university researches Discoveries in microbial physiology and genetics offering new targets, new disciplines Combinational chemistry (mass screening) For lecture only BC Yang
 For lecture only. BC Yang.")
Similar presentations








 Lecture 18 Bacterial Pathogenesis (Based on other textbooks such as Madigan’s)>")



>")









