Download presentation
Presentation is loading. Please wait.

1
Hypertension in Pregnancy
Ramon M. Gonzalez, MD Professor UST Medicine and Surgery

2
A 26y/o G weeks known hypertensive for 6 years was admitted because of severe hypertension VS- BP-200/100mmHg, PR- 76/min, RR-20/min, T-36.5C. She was taking calcium channel blockers for her HPN which she was taking regularly.

3
Hypertensive Disorders Complicating Pregnancy
Gestational Hypertension Systolic BP≥ 140 or diastolic ≥ 90 mmHg for the first time after 20 weeks gestation No proteinuria BP returns to normal before 12 weeks postpartum Final diagnosis made only postpartum May have other signs or symptoms of preeclampsia

4
Hypertensive Disorders Complicating Pregnancy
Preeclampsia Minimum criteria BP ≥ 140/90 mmHg after 20 weeks gestation Proteinuria ≥ 300mg/24 hours or ≥ 1+ dipstick Severe preeclampsia BP ≥ 160/110 mmHg Proteiunuria 2.0gms/24 hrs or ≥ 2+ dipstick Serum creatinine > 1.2mg/dl Platelets < 100,00/ul Elevated LDH, ALT or AST

5
Hypertensive Disorders Complicating Pregnancy
Eclampsia Seizures that cannot be attributed to other causes in women with preeclampsia Chronic Hypertension BP ≥ 140/90 mmHg before pregnancy or diagnosed before 20 weeks gestation Hypertension first diagnosed after 20 weeks gestation and persistent after 12 weeks postpartum

6
Hypertensive Disorders Complicating Pregnancy
Superimposed Preeclampsia New onset proteinuria ≥ 300mg/24 hrs in hypertensive women but no proteinuria before 20 weeks gestation

7
Pregnancy 20-21 weeks, Chronic Hypertension

8
Maternal Assessment Duration of hypertension Current therapy
Degree of BP control Other medical complications

9
Maternal Assessment Serum creatinine Quantification of urine proteins
ECG Echocardiography Blood chemistry

10
What are the effects of chronic hypertension on pregnancy?
What is the management of chronic hypertension during pregnancy? Can we prevent superimposition of preeclampsia ? What is the management of chronic hypertension with superimposed preeclampsia?

11
What are the effects of chronic hypertension on pregnancy?

13
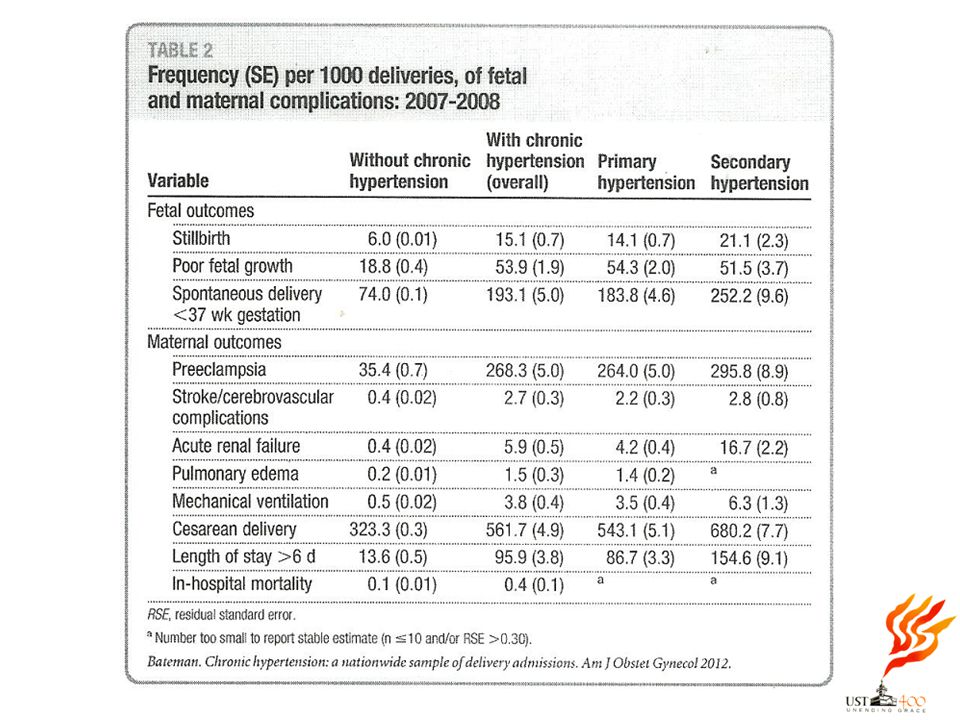
ORs for Fetal Complications: 1995-2008
Pregestational Diabetes Variable With Chronic HPN W/O Chronic HPN ________________________________________________________ Stillbirth 4.30( ) 3.05( ) Poor fetal growth 2.66( ) 1.20( ) Spontaneous delivery 4.88( ) 2.90( ) <37weeks
 3.05( ) Poor fetal growth 2.66( ) 1.20( ) Spontaneous delivery 4.88( ) 2.90( ) <37weeks")
14
ORs for Maternal Complications: 1995-2008
Pregestational Diabetes Variable With Chronic HPN W/O Chronic HPN __________________________________________________________ Preeclampsia ( ) ( ) CVA ( ) ( ) Acute renal failure ( ) ( ) Pulmonary edema ( ) ( ) Ventilation ( ) ( ) Cesarean delivery ( ) ( ) In- hospital mortality ( ) ( )
 3.80 ( ) CVA 7.14 ( ) 1.85 ( ) Acute renal failure ( ) 4.43 ( ) Pulmonary edema ( ) 4.01 ( ) Ventilation ( ) 3.34 ( ) Cesarean delivery 5.75 ( ) 3.33 ( ) In- hospital mortality 6.02 ( ) 2.58 ( )")
15
ORs for Fetal Complications: 1995-2008
Chronic Renal Disease Variable With Chronic HPN W/O Chronic HPN ________________________________________________________ Stillbirth 7.29( ) 1.74( ) Poor fetal growth 7.94( ) 2.29( ) Spontaneous delivery 8.60( ) 2.25( ) <37weeks
 1.74( ) Poor fetal growth 7.94( ) 2.29( ) Spontaneous delivery 8.60( ) 2.25( ) <37weeks")
16
ORs for Maternal Complications: 1995-2008
Chronic Renal Disease Variable With Chronic HPN W/O Chronic HPN __________________________________________________________ Preeclampsia ( ) ( ) CVA ( ) ( ) Acute renal failure ( ) ( ) Pulmonary edema ( ) ( ) Ventilation ( ) ( ) Cesarean delivery ( ) ( ) In- hospital mortality ( ) ( )
 3.28( ) CVA 13.73( ) 3.53( ) Acute renal failure 253.4( ) 62.40( ) Pulmonary edema 23.29( ) 9.06( ) Ventilation 19.29( ) 8.25( ) Cesarean delivery 5.73( ) 1.74( ) In- hospital mortality 27.02( ) 6.88( )")
17
ORs for Fetal Complications: 1995-2008
Collagen Vascular Disease Variable With Chronic HPN W/O Chronic HPN ________________________________________________________ Stillbirth 7.42( ) 2.74( ) Poor fetal growth 7.99( ) 3.87( ) Spontaneous delivery 7.19( ) 3.15( ) <37weeks
 2.74( ) Poor fetal growth 7.99( ) 3.87( ) Spontaneous delivery 7.19( ) 3.15( ) <37weeks")
18
ORs for Maternal Complications: 1995-2008
Collagen Vascular Disease Variable With Chronic HPN W/O Chronic HPN __________________________________________________________ Preeclampsia ( ) ( ) CVA ( ) ( ) Acute renal failure ( ) ( ) Pulmonary edema ( ) ( ) Ventilation ( ) ( ) Cesarean delivery ( ) ( ) In- hospital mortality ( ) ( )
 2.96 ( ) CVA ( ) 7.60 ( ) Acute renal failure ( ) ( ) Pulmonary edema ( ) 6.08 ( ) Ventilation ( ) ( ) Cesarean delivery 4.38 ( ) 1.89 ( ) In- hospital mortality ( ) ( )")
19
What is the management of chronic hypertension during pregnancy?

20
Management Blood pressure control Fetal antepartum surveillance
Prevention of preeclampsia Detection of preeclampsia

21
Blood Pressure Control
Ca Channel Blockers Adrenergic Blocking Agents Vasodilators Diuretics ACE Inhibitors/ARB contraindicated

22
El Guindy, A.A. and Nabhan, A.F. (2008) Journal of Perinatal Medicine
A randomized trial of tight vs. less tight control of mild essential and gestational hypertension in pregnancy El Guindy, A.A. and Nabhan, A.F. (2008) Journal of Perinatal Medicine Women in the tight control group Were less likely to develop severe hypertension (RR 0.32, 95% CI 0.14 to 0.74) Delivered babies with older gestational ages (36.6 ±2.2 weeks vs 35.8 ± 2.2 weeks: P<0.05) Fewer preterm deliveries (RR 0.52, 95%CI 0.28 to 0.99) No significant differences between groups regarding stillbirth or IUGR
 Journal of Perinatal Medicine. Women in the tight control group. Were less likely to develop severe hypertension (RR 0.32, 95% CI 0.14 to 0.74) Delivered babies with older gestational ages (36.6 ±2.2 weeks vs 35.8 ± 2.2 weeks: P<0.05) Fewer preterm deliveries (RR 0.52, 95%CI 0.28 to 0.99) No significant differences between groups regarding stillbirth or IUGR.")
23
Fetal Antepartum Surveillance
Fetal biometry Nonstress test Contraction stress test Biophysical profile Doppler velocimetry

24
Can we prevent superimposition of preeclampsia?

25
Preeclampsia Pregnancy specific syndrome that can affect virtually every organ system. Disorder of unknown etiology affecting 5-10% of all pregnancies. In developed countries 16% of maternal deaths were due to hypertensive disorder. POGS (2006) % maternal deaths were due to hypertensive disorder.
 % maternal deaths were due to hypertensive disorder.")
26
Pathogenesis Vasospam Increased resistance → hypertension
Endothelial cell damage → leakage of blood constituents, including platelets and fibrinogen Decreased blood flow → ischemia of tissues → necrosis, hemorrhage and other end organ disturbances

27
Pathogenesis Endothelial cell activation Increased pressor responses
Increased sensitivity to angiotensin II Prostaglandin Prostacyclin: thromboxane A2 ratio decreases Nitric oxide Decreased nitric oxide synthase expression Endothelins Potent vasoconstrictor which is increased in preeclampsia

28
Cardiovascular System
↑ Cardiac afterload hypertension ↑Cardiac preload Diminished hypervolemia ↑ intravenous crystalloids Extravasation of intravascular fluid into the extracellular space Pulmonary edema

29
Blood Volume and Coagulation
Hemoconcentration Hallmark of preeclampsia Vasospasm and endothelial leakage Thrombocytopenia Hemolysis Endothelial disruption HELLP syndrome

30
Kidneys ↓ Glomerular filtration rate and renal plasma flow
↑ Serum creatinine ↑ Uric acid Proteinuria Oliguria “Glomerular capillary endotheliosis” Acute renal failure

31
Liver Hepatic infarction Periportal hemorrhage Hepatocellular necrosis
Elevations of AST/ALT Hepatic hematoma HELLP syndrome

32
Brain Headaches, visual symptoms Convulsions Intracerebral hemorrhage
Cortical and subcortical petechial hemorrhages Subcortical edema

33
Uteroplacental Perfusion
Vasospasm ↓ Decreased uteroplacental perfusion Increased perinatal morbidity and mortality

34
Prevention of Superimposed Preeclampsia
Systematic Review by Duley et al 59 trials with 37,560 women given Aspirin 17% reduction in the risk of preeclampsia (RR 0.83, ), especially in high risk patients 8% reduction in the relative risk of preterm birth (RR 0.92, ) 14% reduction in fetal and neonatal deaths (RR 0.86, ) 10% reduction in SGA babies (0.90, )
, especially in high risk patients. 8% reduction in the relative risk of preterm birth (RR 0.92, ) 14% reduction in fetal and neonatal deaths (RR 0.86, ) 10% reduction in SGA babies (0.90, )")
35
Detection of Preeclampsia
BP monitoring 24 hour urine proteins

36
What is the management of chronic hypertension with superimposed preeclampsia?

37
Management Termination of pregnancy with the least possible trauma to mother and baby Birth of an infant who subsequently thrives Complete restoration of health to the mother

38
Severe Preeclampsia Clinical course is progressive deterioration in both maternal and fetal condition Associated with high rates of maternal and perinatal morbidity and mortality

39
Management of Severe Preeclampsia
Aggressive High neonatal mortality and morbidity due to prematurity Prolonged NICU stay Long term disability Expectant - Fetal death - Asphyxial damage in utero - Increased maternal morbidity

41
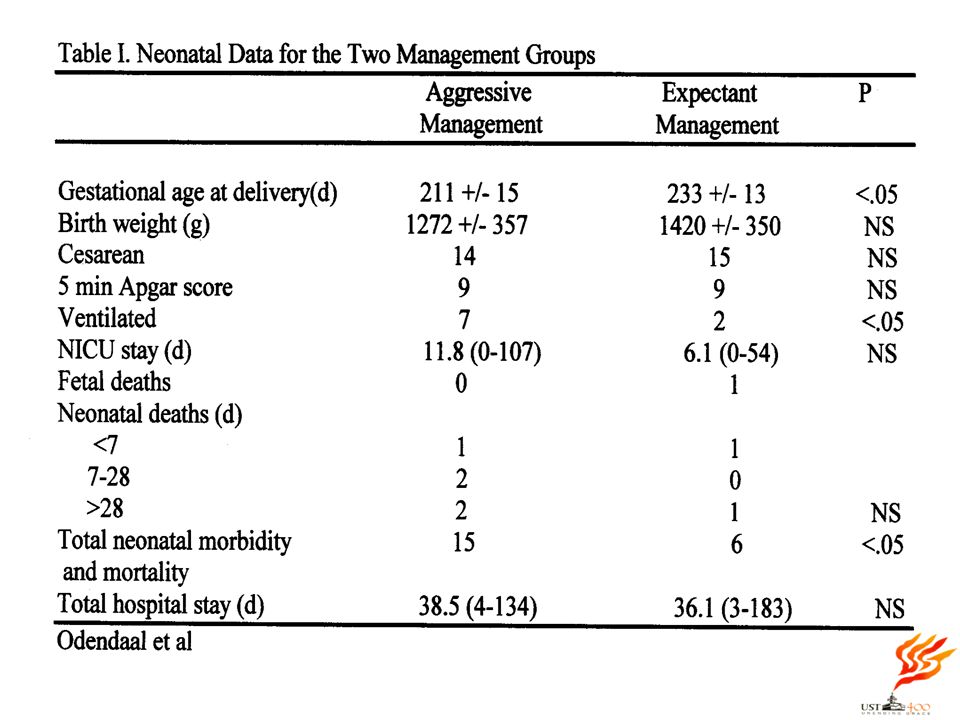
Odendaal and associates
Aggressive vs expectant management 58 patients, 20 were delivered w/in 48 hours 20 aggressive, 18 expectant 28-34 weeks Betamethasone, MgSO4, Antihypertensive drugs Maternal and fetal testing

43
Sibai and colleagues Aggressive vs expectant management 28-32 weeks
95 patients Aggressive (n=46); expectant (n=49) Bed rest, antihypertensives, MgSO4, betamethasone, maternal and fetal testing, laboratory exams
; expectant (n=49) Bed rest, antihypertensives, MgSO4, betamethasone, maternal and fetal testing, laboratory exams.")
47
Expectant Management Prolongs pregnancy Higher gestational age
Higher birth weight Lower incidence of admission to NICU Lower incidence of neonatal complication No difference in the incidence of CS, abruptio placenta, HELLP syndrome and postpartum stay

48
Guidelines for Expectant Management
Hospitalization in a tertiary hospital - Good facilities to monitor the mother and fetus - NICU facilities - Trained personnels MgSO4 Antihypertensives Corticosteroids

49
Maternal Assessment

50
Maternal Assessment Blood pressure measurement
- Systolic – 140 – 155 mmHG - Diastolic – 90 – 105 mmHG Daily 24 hour urine volume Maternal symptoms Search for imminent signs of eclampsia Sibai et al AmJOG 2007

51
Maternal Assessment CBC with platelet counts Serum creatinine
Liver function test AST/ALT Lactate dehydrogenase Sibai et al AmJOG 2007

52
Fetal Assessment

53
Fetal Assessment Fetal kick counts NST Biophysical profile scoring
Umbilical artery Doppler studies Assessment of fetal growth

54
Maternal Indications for Delivery in Women With Severe Preeclampsia
Persistent severe headache or visual changes; eclampsia Pulmonary edema Uncontrolled severe HPN Epigastric pain/RUQ pain with AST or ALT >2 times the upper limit of normal Sibai et al AmJOG 2007

55
Maternal Indications for Delivery in Women With Severe Preeclampsia
Oliguria (<500ml/24hr) HELLP syndrome Platelet counts <100,000/mm3 Deterioration of renal function (serum creatinine >/=1.5 mg/dl) Suspected abruptio placenta, progressive labor, and/or rupture of membranes Sibai et al AmJOG 2007
 HELLP syndrome. Platelet counts <100,000/mm3. Deterioration of renal function. (serum creatinine >/=1.5 mg/dl) Suspected abruptio placenta, progressive labor, and/or rupture of membranes. Sibai et al AmJOG")
56
Fetal Indications For Delivery In Women With Severe Preeclampsia
Repetitive late or severe variable deceleration Biophysical profile </=4 on 2 occasions at 6 hours apart IUGR (Estimated fetal weight <5th percentile) Umbilical artery Doppler with reverse end diastolic flow Severe oligohydramnios Sibai et al AmJOG 2007
 Umbilical artery Doppler with reverse end diastolic flow. Severe oligohydramnios. Sibai et al AmJOG")
57
Mode of Delivery Vaginal delivery - Inducible cervix
- No fetal distress Cesarean section

58
Thank You

Similar presentations






















 February, 2004 Nicolas Szecket (From New Zealand)>")