Download presentation
Presentation is loading. Please wait.

1
Sling Failures Jerry G. Blaivas, MD Clinical Professor of Urology
Weil-Cornell Medical Center Adjunct Professor of Urology SUNY Downstate Medical Center

2
Why Do Operations Fail? Too tight Too loose Wrong position
Detrusor overactivity De-novo Persistent Erosion Wrong indication

3
Too Tight Urethral obstruction Detrusor overactivity Erosion
Devascularization > recurrent SUI

4
Urethral Obstruction Clinical: Urodynamics: De-novo symptoms
Weak stream OAB negative Q-tip angle Urodynamics: High detrusor pressure / low flow: pdetmax > 20 cm H20 Qmax < 12 ml/S Blaivas Groutz nomogram

5
- 45O

6
High pressure (pdetmax = 75)
Low flow (0) High pressure (pdetmax = 75) MSCO
 High pressure (pdetmax = 75) MSCO.")
7
Blaivas - Groutz Nomogram
Figure 1.Blaivas-Groutz Nomogram divides woman into 4 groups. Blaivas & Groutz, Neurourol & Urodynam 19: , 2000

8
Rx of Post op Urinary Retention
Depends on type of sling Initial Rx intermittent catheterization Synthetic sling early intervention days – weeks Autologous slings Delayed intervention – months

9
Rx of Post op Urinary Retention
? Need for further workup Q-tip cystoscopy urodynamics

10
Surgical Rx of Sling Obstruction
Sling incision midline lateral Urethrolysis antero-lateral circumferential +/- Martius flap interposition Technique determined intraop

11
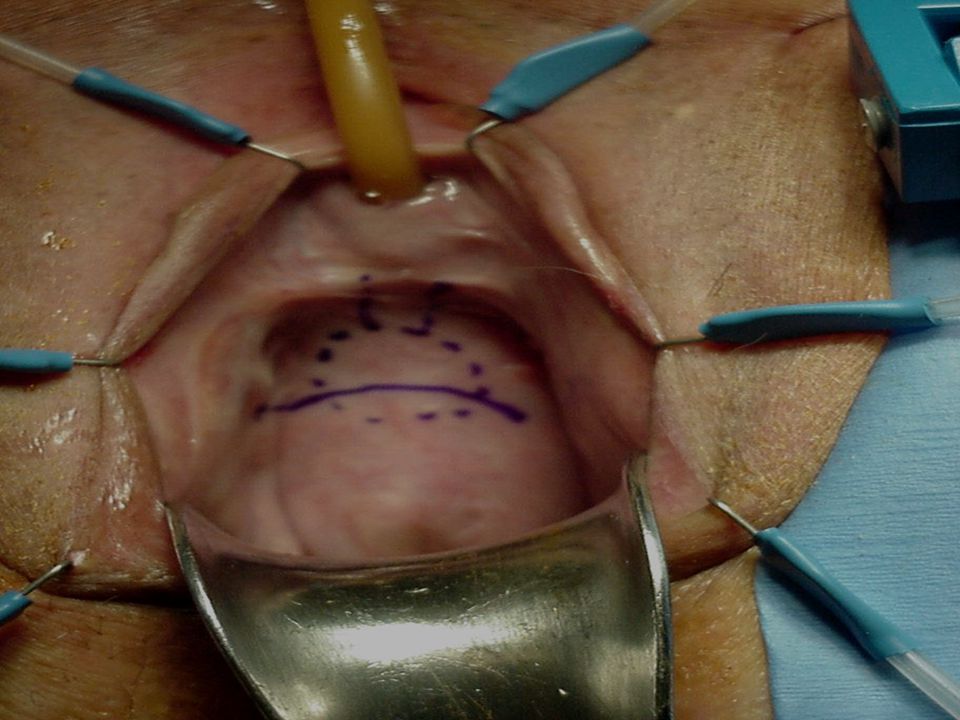
Transvaginal Incision of Sling
Slightly curved/horizontal incision over sling Dissect superficial to sling Identify normal urethra Mobilize small vaginal wall flap & identify sling

13
Transvaginal Incision of Sling
Grasp sling with Allis clamps & pull outward Dissect between sling & urethra Incise sling in midline Sling should spring apart

16
Sling Incision Results
Type Success % SUI % Nitti, et al 19 Midline Incision 84% 17% Amundsen, et al 32 Various 94% 9% Goldman, et al 14 93% 21% Nitti et al. Early results of pubovaginal sling lysis by midline sling incision. Urology 2002. Amundsen et al. Variations in strategy for the treatment of urethral obstruction after a pubovaginal sling procedure. J Urol Goldman et al. Simple sling incision for the treatment of iatrogenic urethral obstruction. Urology 2003

17
Urethrolysis Vaginal Supra-meatal Retropubic

18
Urethrolysis Vaginal Supra-meatal Retropubic

19
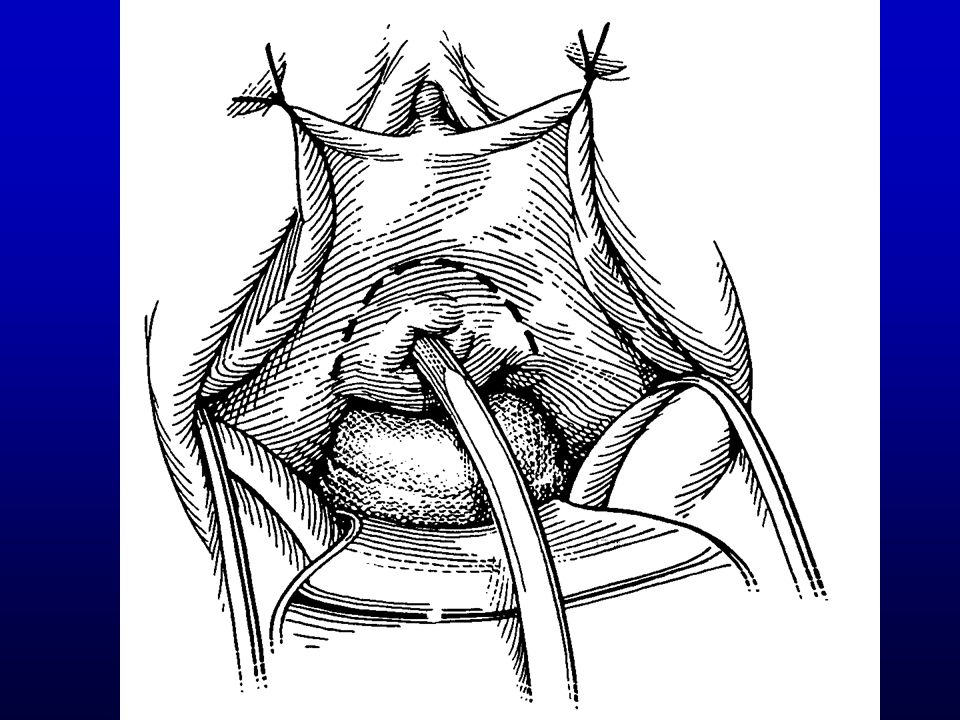
Transvaginal Urethrolysis
Inverted “U” incision over point of obstruction Dissect superficial to obstructing tissue Incise sling laterally on either side

20
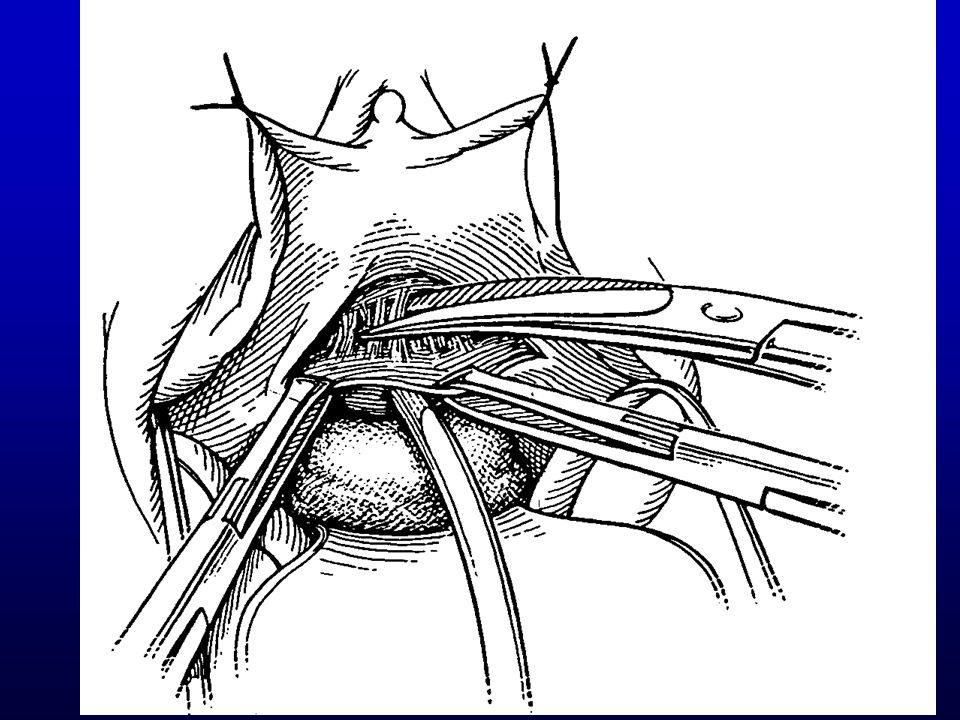
Transvaginal Urethrolysis
Perforate endopelvic fascia at lateral margin of dissection Mobilize vesical neck & urethra +/- Circumferential mobilization of urethra +/- Omental or Martius interposition

26
Circumferential Urethrolysis

27
Urethrolysis Vaginal Supra-meatal Retropubic

28
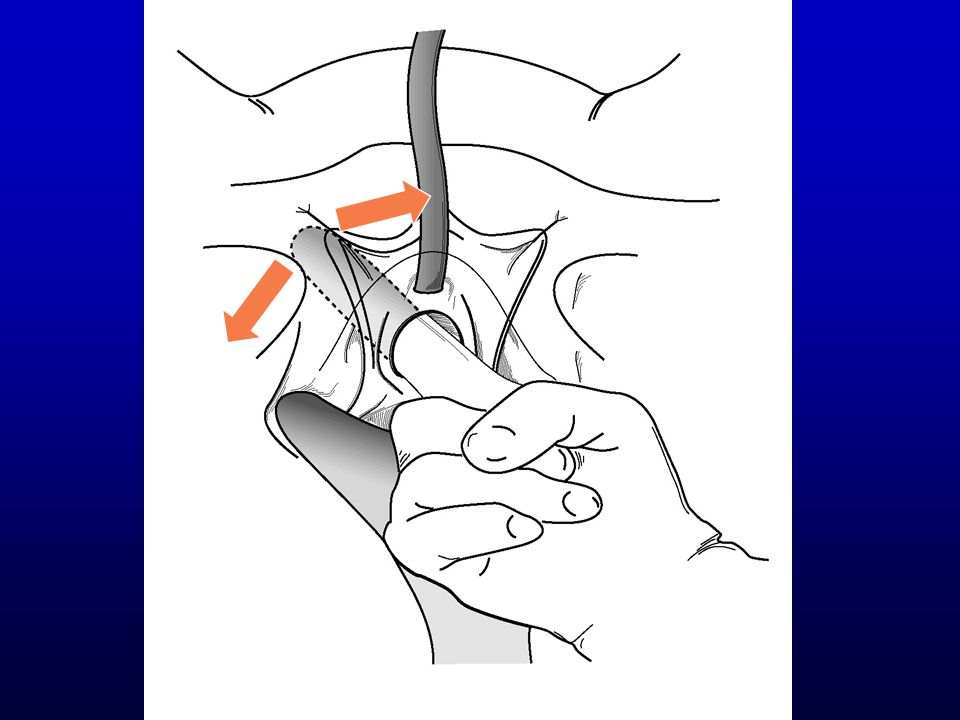
Supra-meatal Urethrolysis
Transverse incision just above urethral meatus Dissect in midline above urethra Press down on urethra with index finger

30
Supra-meatal Urethrolysis
Incise sling/sutures under direct vision +/- circumferential urethral mobilization +/- Martius or omental interposition

35
Urethrolysis Vaginal Supra-meatal Retropubic

36
Retropubic Urethrolysis
Transverse incision just above the pubis Enter retropubic space Downward pressure on bladder neck & urethra

37
Retropubic Urethrolysis
Incise sling/sutures under direct vision Open bladder if necessary +/- circumferential urethral mobilization +/- Martius or omental interposition

38
Urethrolysis Results N Type Success % SUI (%) Foster & McGuire 48
Transvaginal 65% 0% Nitti & Raz 42 71% Cross, et al 39 72% 3% Goldman, et al 32 84% 19% Petrou, et al Suprameatal 67% Petrou & Young 12 Retropubic 83% 18% Carr & Webster 54 Mixed 78% 14%

39
Too Tight Urethral obstruction Detrusor overactivity Erosion
Devascularization > recurrent SUI

40
Too Tight Urethral obstruction Detrusor overactivity Erosion
Devascularization > recurrent SUI

41
Bladder neck Bladder neck Eroded mesh

42
VLPP Barbara Jankowski UDS December 2005
Barbara Jankowski is a 65-year-old married woman who underwent urethral diverticulectomy in 10/04 by Judy Siegel. The diverticulum was very large and extended from the meatus to bladder neck. “The repair was buttressed with a Pelivichol patch.” .12/5/05 – incision of urethral stricture; 8/05 “stricture lasered.” on 11/10 she underwent collagen injection at the bladder neck and, at that time, a “distal urethovaginal fistula was diagnosed. She was referred to Basil Kocur and was diagnosed with multiple vesicovaginal fistulas and needed abdominal surgery. Her chief complaint is daily incontinence, but she doesn’t know for sure exactly when it happens other that to say, its worst when she is physically active and does not occur at night when she is in bed. She denies classic stress or urge incontinence. She ordinarily feels the urge to void about once an hour, but does not actually void each time. On average, the longest time she goes without urinating during the day is about three hours. The main reason she urinates as often as she does is because of normal feelings to urinate. She ordinarily initiates micturition without difficulty. The force of her stream is usually strong. She feels that she has not emptied her bladder after urinating rarely. She wears absorbent pads daily, and she changes them 6 times per day. The pads are usually clearly wet. Her AUA symptom score is 9. CYSTOMETROGRAM: The Cystometrogram was performed using radiographic contrast and a #7 double lumen catheter via constant infusion at a 'medium' filling rate with rectal pressure monitoring and the patient sitting. Residual bladder volume was 0ml, 0 hours after voiding. Empty bladder pressure was 0cm H20. First filling sensation occurred at 240.6ml, with a detrusor pressure of 0.5cm H20. The first urge occurred at 399.7ml with a detrusor pressure of 1cm H20 and a severe urge occurred at 1,006ml, with a detrusor pressure of 2cm H20. During bladder filling there were no spontaneous involuntary detrusor contractions. Bladder capacity was 1,006 ml. Maximum filling pressure was 3cm H20. Bladder compliance was high.

44
Treatment of Erosions. remove as much of sling as possible
closure of the urethra +/ - urethral reconstruction +/ - biologic sling +/ - Martius flap

45
Too Tight Urethral obstruction Detrusor overactivity Erosion
Devascularization > recurrent SUI

46
Why Do Operations Fail? Too tight Too loose Wrong position
Detrusor overactivity De-novo Persistent Erosion Wrong indication

47
Too Loose Urethral hypermobility Intrinsic sphincter deficiency
Recurrent sphincteric incontinence

48
VLPP VLLP = 92 cm H20 Qtip = 0 > 60O AG AG AG
Figure 9. Stress incontinence with urethral hypermobility and type 1 OAB. This corresponds to Type 2 SUI according to the Blaivas/Green/McGuire classification. AG is a 51 year old white woman with a chief complaint of gradually worsening stress incontinence of 10 years duration. About once or twice a month she soaks her clothes when she has been walking or does high impact aerobics. She wears one mini-pad all day which, at the end of the day is damp; "sometimes they're wetter than others”. She also gets urgency & urge incontinence when she puts the key in her door lock, but has learned to control this by voiding beforehand. A.Urodynamic tracing. FSF = 10 ml; First urge = 251 ml; Severe urge = 492 ml. VLLP = 85 cm H2O. Bladder capacity = 585 cm H20. When asked to void, she strained a bit, but could not generate a detrusor contraction and was unable to void (light blue oval). VLPP = 50 cm H20 AG AG AG
. VLPP = 50 cm H20. AG. AG. AG.")
49
Figure 9 B. X-ray exposed at VLPP shows rotational descent of the urethra and incontinence. Q-tip angle was 65O. Comment: AG has classic type 2 stress incontinence and would likely do well after anti-incontinence surgery, but when advised of the remote possibility of urinary retention, elected behavioral therapy. AG

50
JK VLPP = 42 cm H20 Q tip = 0

52
Treatment of Recurrent SUI
no compelling data for hypermobility, surgeon choice for poorly mobile or pipe - stem urethra, biologic bladder neck sling

53
Why Do Operations Fail? Too tight Too loose Wrong position
Detrusor overactivity De-novo Persistent Erosion Wrong indication

54
Wrong Position Too far proximal Too far distal
persistent sphincteric incontinence urethral obstruction ureteral injury Too far distal urethral hypermobility

55
Sling proximal to BN VLPP = 35 cm H20 MS

56
sling

57
No flow High pdet Figure . Urethral obstruction due to autologous fascial pubovaginal sling. A. Urodyanmic tracing. There is a sustained detrusor contraction to over 75 cm H20 and no flow.This corresponds to a grade 2 urethral obstruction on the Blaivas Groutz nomogram. MSCO

58
Fig B.X-ray exposed at pdetmax shows complete obstruction of the urethra at the bladder neck (black arrow), presumably from a prior sling operation. Note the left vesicoureteral reflux (white arrows) MSCO

59
MSCO C. The vesicoureteral reflux extends into the kidney and distends the collecting system.(grade 3).
.")
60
Why Do Operations Fail? Too tight Too loose Wrong position
Detrusor overactivity De-novo Persistent Erosion Wrong indication

61
Wrong Indication Urinary fistula mistaken for sphincteric incontinence
Overactive bladder mistaken for sphincteric incontinence Sine-qua-non - Never operate on stress incontinence without actually diagnosing sphincteric incontinence with your own eyes

62
Conclusion Complications & failures after incontinence surgery are not uncommon Early evaluation to rule out remediable causes should be undertaken UTI Urethral obstruction sling erosion foreign body A successful outcome is likely in the majority of patients

Similar presentations





























. Pre-operative work up and intra-operative complications. Analysis of the BSUG database R.P. Assassa, J. Duckett,>")
