Download presentation
Presentation is loading. Please wait.

1
Cerebrovascular Disease
William R. Rooney, MD VP & Medical Director Generali USA Life Reassurance

2
Welcome & Webinar Guidelines
Thanks for attending!! Phones will be locked during the presentation Please submit questions by using the question “?” function in the lower right corner to type in your question Question & Answers will be discussed at the end (time permitting) Your comments are important; please complete the survey at the end of the webinar
 Your comments are important; please complete the survey at the end of the webinar.")
3
Introduction: William Rooney, M.D. FAAFP, EMBA
Joined Generali USA in April, 2012 20 year history of direct patient care. Eight years of insurance industry experience. Board certified in Family Medicine

4
Primary and secondary treatment Another look at Mortality numbers
Overview Stroke Facts Mortality numbers Definitions Anatomy review Types of strokes Diagnosis Primary and secondary treatment Another look at Mortality numbers CIMT, Carotid US, and Silent strokes

5
CASE 2 cases arrive for underwriter review. Which has the worst mortality risk based upon the following limited information provided? Case 1: 66 y/o female with hx. of a “TIA-like” event 4 years ago with no subsequent symptoms. Hx. of hypertension and hyperlipidemia. BMI 30 MRI of the brain WNL. US of the carotids WNL. ECG WNL. CIMT abnormal at 90th percentile for age. Case 2: 65 y/o female with no known neurological complaints—past or present Hx. of hypertension and hyperlipidemia. BMI 30 MRI of the brain shows 2 small lacunar infarcts—age unknown US of the carotids WNL ECG WNL CIMT normal

6
795,000 Americans suffer strokes each year
Stroke Facts 795,000 Americans suffer strokes each year 134,000 deaths each year 6,400,000 stroke survivors 34% of people hospitalized for stroke in 2009 were under 65 years of age. References: American Heart Association. Heart Disease and Stroke Statistics 2010 Update At-a-Glance. At:

7
Prevalence of stroke by age and sex
Chart 4-1. Prevalence of stroke by age and sex (NHANES: 1999–2004). Source: NCHS and personal communication with NHLBI. Rosamond W et al. Circulation 2007;115:e69-e171 Copyright © American Heart Association
. Source: NCHS and personal communication with NHLBI. Rosamond W et al. Circulation 2007;115:e69-e171. Copyright © American Heart Association.")
8
Annual stroke death rate fell 35%. Actual number of deaths fell 19%.
Stroke Facts Women are twice as likely to die from stroke than breast cancer annually. African Americans have almost twice the risk of first ever stroke compared to whites. Hispanic Americans’ risk falls between those of whites and African Americans. A leading cause of death in the United States : Annual stroke death rate fell 35%. Actual number of deaths fell 19%. Stroke is a leading cause of death in the United States behind heart disease and all forms of cancer combined. Approximately 795,000 Americans have a new or recurrent stroke each year. Stroke kills approximately 134,000 Americans each year. From 1996 to 2006, the stroke death rate fell 33.5% and actual number of stroke deaths fell by 18.4%. There are more than 6 million stroke survivors living in the United States. Men make up about 2,500,000 of survivors and women make up 3,900,000. About one-third have mild impairments, another third are moderately impaired and the remainder are severely impaired. References: American Heart Association. Heart Disease and Stroke Statistics 2010 Update At-a-Glance. At:

9
Temporal trends in age-adjusted death rates for the top 10 causes of death in the United States from 1931 to 2008. 2nd most common cause of death world wide In 2008 CVA dropped from the 3rd most common cause of death in the US to the 4th. Temporal trends in age-adjusted death rates for the top 10 causes of death in the United States from 1931 to 2008. Towfighi A , and Saver J L Stroke 2011;42: Copyright © American Heart Association

10
Mortality rate from Stroke
Similar downward trend noted in the European Union. Point #1 The stroke mortality rate in the Western countries is declining. Decreased incidence Decreased case-fatality rate Point #2 The projected total number of US deaths from strokes is not expected to decline through 2030 however because of the aging population Trend between 1980 and 2005 stroke mortality rates (rates per 100,000 person-years, standardized using the European Union comprising 25 member states [EU25] population by 5 years as the standard population). Men and women in 7 European countries. Kunst A E et al. Stroke 2011;42: Copyright © American Heart Association
. Men and women in 7 European countries. Kunst A E et al. Stroke 2011;42: Copyright © American Heart Association.")
11
Definitions TIA Classic Definition: Rapidly developing clinical signs of focal or global disturbance of cerebral function lasting fewer than 24 hours, with no apparent non-vascular cause. June 2009 AHA/ASA scientific statement definition: A transient episode of neurologic dysfunction caused by focal brain, spinal cord, or retinal ischemia, without acute infarction CVA An infarction of the central nervous system tissue References: Definition and Evaluation of Transient Ischemic Attack. A Scientific Statement for Healthcare Professionals From the American Heart Association/American Stroke Association Stroke Council; Easton, Donald J et al Stroke :40: Definition and Evaluation of Transient Ischemic Attack. A Scientific Statement for Healthcare Professionals From the American Heart Association/American Stroke Association Stroke Council; Easton, Donald J et al Stroke :40:

12
Consequences of the definition change
Anticipate a drop in annual incidence of TIA’s by 33% Increase in diagnosis of CVA’s by 7%. There has been a change in the enrollment of members into studies Potential change in treatment guidelines in the future Mortality statistics impact Comparison of old statistics to newer and future statistics won’t be apples to apples Potential improvement in CVA morbidity and mortality results from earlier treatment. Decreased “wait and see” approach. References: American Heart Association. Heart Disease and Stroke Statistics 2010 Update At-a-Glance. At:

13
Consequences of definition change---Consider 3 diagnosis outcomes
TIA No longer is this the poor prognostic event that it was 90 day risk of stroke with residual symptoms is <1% Image-positive transient event 90 day risk of stroke with residual symptoms is ~14% ~15 x the chance of having a stroke with residual symptoms in the next 7 days as compared to those with a stroke that already have residual neurological symptoms Ischemic stroke with residual neurological symptoms

14
Brain cells have different functions in different locations
Frontal Lobe Personality Memory Reasoning Temporal Lobe Speech Hearing Parietal Lobe Language Sensation Telling right from left Occipital Lobe Vision Cerebellum Balance Fine motor control Coordination Brain Stem Breathing Swallowing Blood Pressure Smell Hearing Speech Fingers Arm Hip Hand Language Vision Balance Coordination

15
Anatomy of the cerebrovascular system

16
The size of the emboli impacts the size of the infarction
The vascular “tree” Strokes from atrial fibrillation are typically associated with more brain tissue involved when compared to carotid artery disease-induced strokes. Presumably due to larger emboli.

17
Two Major Types of Stroke
Ischemia Thrombosis (local obstruction of an artery) Embolism (Debris or blood clot traveling from elsewhere and lodging in an artery causing obstruction) Systemic hypo-perfusion (general medical condition with lack of blood supply reaching the brain Hemorrhage Subarachnoid hemorrhage (bleeding into the CSF within the subarachnoid space around the brain) Intra-cerebral hemorrhage (bleeding directly into the brain tissue) 80% of strokes are secondary to ischemic cerebral infarction 20% of strokes due to hemorrhage
 Embolism (Debris or blood clot traveling from elsewhere and lodging in an artery causing obstruction) Systemic hypo-perfusion (general medical condition with lack of blood supply reaching the brain. Hemorrhage. Subarachnoid hemorrhage (bleeding into the CSF within the subarachnoid space around the brain) Intra-cerebral hemorrhage (bleeding directly into the brain tissue) 80% of strokes are secondary to ischemic cerebral infarction. 20% of strokes due to hemorrhage.")
19
CVA’s are caused by anything that can cause vascular compromise
Heart Atrial fibrillation/rhythm disturbances VSD/PFO/Endocarditis Large Blood Vessels Thrombus Atherosclerosis Takayasu arteritis Giant cell arteritis Fibromuscular dysplasia Emboli Dissection Marfan’s syndrome and other similar conditions Intracranial Blood Vessels Same as large blood vessels but also includes Moya-Moya Rupture of the Blood vessel and bleeding

20
Vascular Compromise Blood itself Bleeding Tendencies
Complication of anticoagulation medications Hemophilia Clotting Tendencies Protein C or S deficiency Prothrombin gene mutation Factor V Leiden Antithrombin III deficiency Hyperhomocysteinemia Antiphospholipid syndrome Essential thrombocytosis Sickle cell anemia Polycythemia Vera

21
TIA—Making the diagnosis

22
TIA—Making the diagnosis
The important point here is that there are several potential etiologies for transient neurological events If vascular compromise is of concern there ideally will be results of a typical diagnostic work-up for underwriter review to assess mortality risk

23
CVA—Making the diagnosis
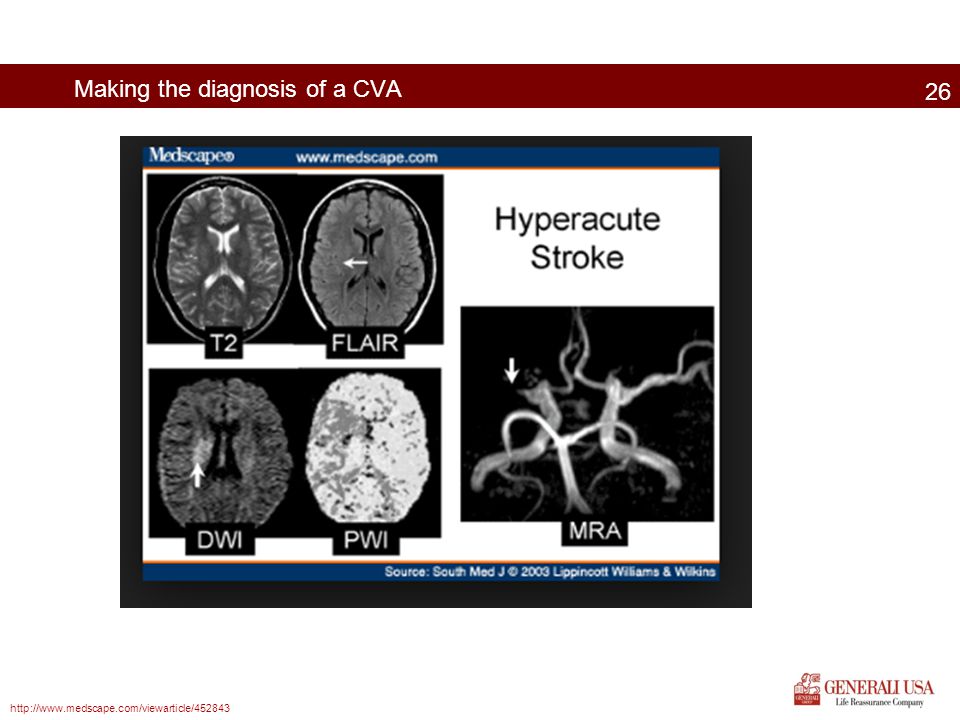
Brain imaging with CT or MRI is indicated in all patients with a suspected TIA or minor non-disabling stroke as soon as possible. The 2013 AHA/ASA guidelines suggest: Imaging techniques and quality of the exams has evolved To some extent the type of imaging performed is based upon the availability of testing devices and expertise of staff Many feel that the Diffusion Weighted Imaging (DWI) MRI is more sensitive than CT for the early detection of acute ischemia. CT’s are frequently more accessible and are frequently used—especially first tests. CT’s are also especially good at detecting the presence of hemorrhage. Imaging within 24 hours of symptom onset MRI and specifically Diffusion-weighted Imaging MRI as the preferred modality Noninvasive imaging (MRA, CTA) of the cervico-cephalic vessels to be part of the evaluation of suspected TIA’s or non-disabling strokes
 MRI is more sensitive than CT for the early detection of acute ischemia. CT’s are frequently more accessible and are frequently used—especially first tests. CT’s are also especially good at detecting the presence of hemorrhage. Imaging within 24 hours of symptom onset. MRI and specifically Diffusion-weighted Imaging MRI as the preferred modality. Noninvasive imaging (MRA, CTA) of the cervico-cephalic vessels to be part of the evaluation of suspected TIA’s or non-disabling strokes.")
24
CVA—Making the diagnosis
Cardiac evaluation is important when TIA or CVA is suspected. Testing frequently performed include: ECG Echocardiogram Cardiac monitoring Other tests are performed as needed Blood cultures Sed rate CBC PT/PTT

25
JOKE TIME!! Diagnostic dilemma What could it be?
What is wrong with me????? So far I have removed a banana from your right ear and a carrot from your nose. Now I find part of an apple in your left ear. You are not eating properly!!!!

26
Making the diagnosis of a CVA
27
Thalamocapsular region
DWI T2 weighted FLAIR Cerebellum region Thalamocapsular region

28
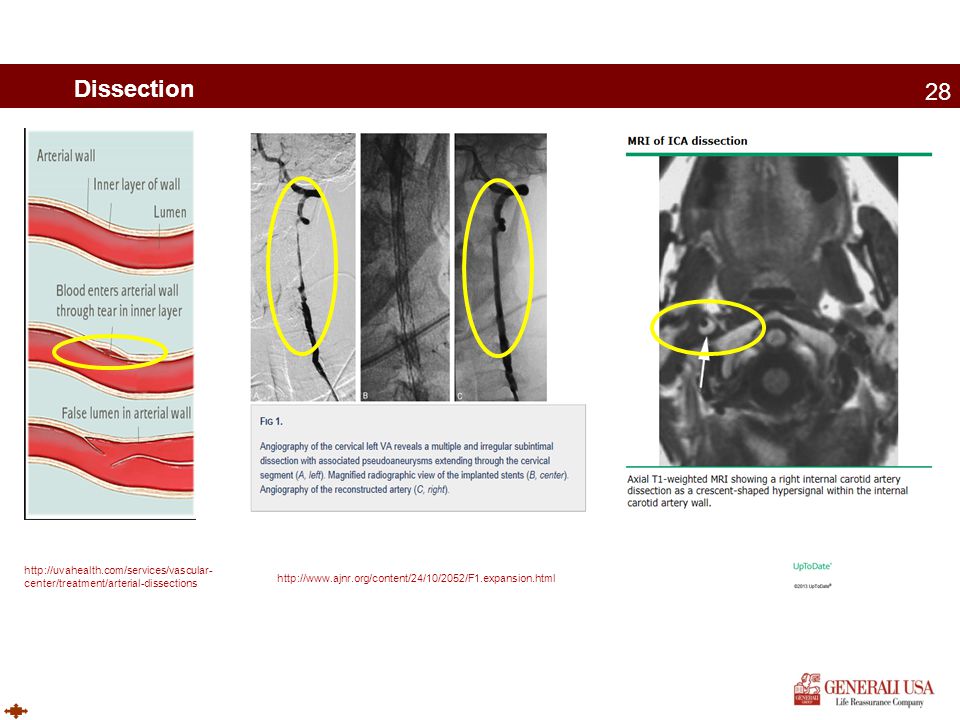
Dissection
29
Primary treatment of an acute ischemic CVA or TIA
Acute Ischemic strokes: Thrombolytic therapy with intravenous alteplase (tPA—recombinant tissue-type plasminogen activator) Early treatment important Many exclusions Unfortunately, in the US only about 8% of all ischemic stroke victims present to the ER within 3 hours and also meet the eligibility criteria for tPA. Vertebral artery or Carotid artery dissecting aneurysms Thrombolytic therapy is not contraindicated and the effectiveness and safety is comparable to ischemic strokes from other causes Extension of the aortic dissection is a potential complication of the thrombolysis however.
 Early treatment important. Many exclusions. Unfortunately, in the US only about 8% of all ischemic stroke victims present to the ER within 3 hours and also meet the eligibility criteria for tPA. Vertebral artery or Carotid artery dissecting aneurysms. Thrombolytic therapy is not contraindicated and the effectiveness and safety is comparable to ischemic strokes from other causes. Extension of the aortic dissection is a potential complication of the thrombolysis however.")
30
Primary treatment of an acute bleed
Subarachnoid hemorrhage Aneurysmal (~80%) Surgical management usually needed Surgical clipping Endovascular therapy with coil system Non-aneurysmal (~20%) AVM Endovascular therapy Intracranial artery dissection Perimesencephalic non-aneurysmal subarachnoid hemorrhage Subtype identified in 1985 Findings of localized blood on CT, normal angiography, and a relatively benign course Long term mortality is significantly better than aneurysmal SAH approaching normal controls. Intra-cerebral bleeding Reversal of anticoagulation Monitoring of intracranial pressure Seizure prophylaxis Surgery for cerebellar decompression and possibly supratentorial ICH (controversial)
 Surgical management usually needed. Surgical clipping. Endovascular therapy with coil system. Non-aneurysmal (~20%) AVM. Endovascular therapy. Intracranial artery dissection. Perimesencephalic non-aneurysmal subarachnoid hemorrhage. Subtype identified in Findings of localized blood on CT, normal angiography, and a relatively benign course. Long term mortality is significantly better than aneurysmal SAH approaching normal controls. Intra-cerebral bleeding. Reversal of anticoagulation. Monitoring of intracranial pressure. Seizure prophylaxis. Surgery for cerebellar decompression and possibly supratentorial ICH (controversial)")
31
Secondary Treatment of the acute ischemic CVA or TIA
Smoking cessation Heavy ETOH consumption should be avoided but light to moderate consumption (no more than 2 per day for men and 1 drink per day for women) is reasonable Physical exercise—30 min of moderate-intensity for 30 min or more 1-3 times per week Antithrombotic therapy initiation within 48 hours of stroke BP management—Goal of therapy is BP of <120/80 mm Hg. Lipid lowering therapy (Statins) for those with elevated LDL >100 mg/dl with goal LDL-C of <70 mg/dL. Prophylaxis for DVT and PE important for those at risk DM management (Diabetics have twice the typical risk for CVA). Unfortunately studies have not provided conclusive evidence that tight control decreases macro-vascular disease similar to the benefit in micro-vascular disease. The AHA/ASA still supports good control of blood sugars however. Guidelines for the Prevention of Stroke in Patients With Stroke or Transient Ischemic Attack. A guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke. 2011; 42:
 is reasonable. Physical exercise—30 min of moderate-intensity for 30 min or more 1-3 times per week. Antithrombotic therapy initiation within 48 hours of stroke. BP management—Goal of therapy is BP of <120/80 mm Hg. Lipid lowering therapy (Statins) for those with elevated LDL >100 mg/dl with goal LDL-C of <70 mg/dL. Prophylaxis for DVT and PE important for those at risk. DM management (Diabetics have twice the typical risk for CVA). Unfortunately studies have not provided conclusive evidence that tight control decreases macro-vascular disease similar to the benefit in micro-vascular disease. The AHA/ASA still supports good control of blood sugars however. Guidelines for the Prevention of Stroke in Patients With Stroke or Transient Ischemic Attack. A guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke. 2011; 42:")
32
Secondary Treatment of the acute ischemic CVA or TIA—Slide 2
Atrial Fibrillation (paroxysmal or permanent): Anticoagulation with a vitamin K antagonist preferred ASA alone for those who can’t tolerate a vitamin K antagonist Prosthetic heart valves Oral anticoagulation with an INR of ASA is recommended to be added to the oral anticoagulation for those with an ischemic event while on anticoagulation Cardiomyopathy with EF <35%: Warfarin, ASA, Clopidogrel, or the combo of ASA and dipyridamole may be considered Non-cardioembolic ischemic strokes or TIA’s Antiplatelet therapy Acute MI and left ventricular thrombus Oral anticoagulation recommended for at least 3 months PFO (Patent Foramen Ovale) Antiplatelet therapy is reasonable Insufficient data to make a recommendation for surgical closure in those with PFO who have had a stroke PFO closure. RESPECT and PC trial results published in the NEJM early PC Trial involved 414 patients. RESPECT involved 980 patients. Both randomized patients to either medical therapy or PFO closure after suffering an ischemic stroke or TIA. No benefit of closure in the main, intention-to-treat- analysis. However in the RESPECT trial there was benefit to closure in a “as-treated_ analysis. Arterial Dissection Antithrombotic treatment for 3-6 months Endovascular stenting should be considered for recurrent ischemic events despite medical treatment Surgical treatment should be considered for those failing stenting. Guidelines for the Prevention of Stroke in Patients With Stroke or Transient Ischemic Attack. A guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke. 2011; 42:
: Anticoagulation with a vitamin K antagonist preferred. ASA alone for those who can’t tolerate a vitamin K antagonist. Prosthetic heart valves. Oral anticoagulation with an INR of ASA is recommended to be added to the oral anticoagulation for those with an ischemic event while on anticoagulation. Cardiomyopathy with EF <35%: Warfarin, ASA, Clopidogrel, or the combo of ASA and dipyridamole may be considered. Non-cardioembolic ischemic strokes or TIA’s. Antiplatelet therapy. Acute MI and left ventricular thrombus. Oral anticoagulation recommended for at least 3 months. PFO (Patent Foramen Ovale) Antiplatelet therapy is reasonable. Insufficient data to make a recommendation for surgical closure in those with PFO who have had a stroke. PFO closure. RESPECT and PC trial results published in the NEJM early PC Trial involved 414 patients. RESPECT involved 980 patients. Both randomized patients to either medical therapy or PFO closure after suffering an ischemic stroke or TIA. No benefit of closure in the main, intention-to-treat- analysis. However in the RESPECT trial there was benefit to closure in a as-treated_ analysis. Arterial Dissection. Antithrombotic treatment for 3-6 months. Endovascular stenting should be considered for recurrent ischemic events despite medical treatment. Surgical treatment should be considered for those failing stenting. Guidelines for the Prevention of Stroke in Patients With Stroke or Transient Ischemic Attack. A guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke. 2011; 42:")
33
Secondary Treatment of the acute ischemic CVA or TIA
Symptomatic extracranial carotid disease: 70-99% stenosis of ipsilateral side: Carotid endarterectomy recommended When morbidity and mortality risk is <6% 50-69% stenosis: Carotid endarterectomy to be considered When morbidity and mortality risk is <6% and Dependent on pt specific factors (age, sex, comorbid conditions) <50% stenosis No indication for endarterectomy or stenting Carotid angioplasty and stenting is an alternative in some settings > 70% stenosis by noninvasive testing Especially those difficult to assess surgically such as radiation induced stenosis or restenosis after endarterectomy > 50% stenosis by angiography Optimal medical therapy including antiplatelet therapy, statins, etc. Extracranial vertebrobasilar disease: Optimal medical therapy Consider surgery when medical therapy has failed. Intracranial atherosclerosis 50-99% stenosis: ASA recommended (in preference to warfarin) Angioplasty and/or stent placement usefulness is unknown and considered E/I Bypass surgery is not recommended Guidelines for the Prevention of Stroke in Patients With Stroke or Transient Ischemic Attack. A guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Furie, Karen et al. Stroke. 2011; 42:
 <50% stenosis. No indication for endarterectomy or stenting. Carotid angioplasty and stenting is an alternative in some settings. > 70% stenosis by noninvasive testing. Especially those difficult to assess surgically such as radiation induced stenosis or restenosis after endarterectomy. > 50% stenosis by angiography. Optimal medical therapy including antiplatelet therapy, statins, etc. Extracranial vertebrobasilar disease: Optimal medical therapy. Consider surgery when medical therapy has failed. Intracranial atherosclerosis % stenosis: ASA recommended (in preference to warfarin) Angioplasty and/or stent placement usefulness is unknown and considered E/I. Bypass surgery is not recommended. Guidelines for the Prevention of Stroke in Patients With Stroke or Transient Ischemic Attack. A guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Furie, Karen et al. Stroke. 2011; 42:")
34
Mortality implications of TIA’s and CVA’s
TIA without images being positive 90 day stroke risk <1% Transient event that is image positive 90 day stroke risk 14% CVA CVA’s have a high peri-stroke period mortality rate Complications clearly are determined by Location of the stroke How much brain tissue is involved 95% of patients have at least one medical complication1 24% of patients have at least one serious, life threatening complication1 Direct effects of the stroke cause death in the first few days. Medical complications account for the mortality thereafter In the first year the most common cause of death is2: First week: Cerebrovascular disease 2-4 weeks: PE 2-3 months: Pneumonia >3 months Cardiac disease 1Randomized trial of Tirilizad Mesylate in Acute Stroke (RANTTAS) 2Risk of myocardial infarction and vascular disease after transient ischemic stroke and ischemic stroke: a systematic review and meta-analysis. Touze E et al Stroke :36 (12):2748
 2Risk of myocardial infarction and vascular disease after transient ischemic stroke and ischemic stroke: a systematic review and meta-analysis. Touze E et al. Stroke. 2005:36 (12):2748.")
35
Cardiac complications of a stroke
Cardiac complications are not just the association of atherosclerosis Stroke is a coronary artery disease risk equivalent Those with a stroke with no known coronary disease have a similar risk of MI as those with established coronary disease Takotsubo cardiomyopathy is one condition that can occur Extreme catecholamine release is postulated to cause this Causes an acute cardiomyopathy Interestingly it typically involves the apical and mid sections of the heart ECG abnormalities present in 92% of patients with an acute stroke Classic large and upright T waves can occur Prolonged QT intervals are common Cardiac arrhythmias

36
Included those with hx. of heart disease
Did not include those with hx. of heart disease

37
What percentage of stroke victims die within 5, 10 and 15 years?
4 QUESTIONS What percentage of stroke victims die within 1 month of their first stroke? What percentage of stroke victims die within 5, 10 and 15 years? Does age matter? Does type of stroke matter?

38
Proportion of patients dead 1 year after first stroke.
>64 y/o 45-64 y/o Proportion of patients dead 1 year after first stroke. Source: Pooled data from the Framingham Heart Study, Atherosclerosis Risk in Communities study, and Cardiovascular Health Study of the National Heart, Lung, and Blood Institute. Go A S et al. Circulation 2013;127:e6-e245 Copyright © American Heart Association

39
Proportion of patients dead within 5 years after first stroke.
>64 y/o 45-64 y/o Proportion of patients dead within 5 years after first stroke. Source: pooled data from the Framingham Heart Study, Atherosclerosis Risk in Communities study, and Cardiovascular Health Study of the National Heart, Lung, and Blood Institute. Compared to the general population nonfatal stroke is associated with a: 5 fold increase for death between 1 month and 1 year. 2 fold increase for death at 5 years Writing Group Members et al. Circulation 2012;125:e2-e220 Copyright © American Heart Association

40
Figure 1. Short-term survival probability for patients aged 65 years at first nonfatal stroke by subtype (Cox regression). Estimated cumulative risk for death: 28 days 28% 1 year 41% 5 years 60% However, risk of death did vary based upon type of stroke IDS Ill Defined Stroke CI Cerebral Infarct SAH Subarachnoid Hemorrhage PICH 1o Intracerebral Bleed Part of the World Health Organizations (WHO) MONICA (Monitoring Trends and Determinants in Cardiovascular Disease) Project. 4,162 patients with a first stroke eligible for analysis Brønnum-Hansen H et al. Stroke 2001;32: Copyright © American Heart Association
 MONICA (Monitoring Trends and Determinants in Cardiovascular Disease) Project. 4,162 patients with a first stroke eligible for analysis. Brønnum-Hansen H et al. Stroke 2001;32: Copyright © American Heart Association.")
41
Figure 2. Long-term survival probability for patients aged 65 years at first nonfatal stroke by subtype (Cox regression). Estimated cumulative risk for death: 5 years 60% 10 years 76% 15 years 86% SAH Subarachnoid Hemorrhage Figure 2. Long-term survival probability for patients aged 65 years at first nonfatal stroke by subtype (Cox regression). PICH, primary intracerebral hemorrhage; CI, cerebral infarct; and IDS, ill-defined stroke patients. SAH Subarachnoid Hemorrhage CI Cerebral Infarct PICH 1o Intracerebral Bleed IDS Ill Defined Stroke Brønnum-Hansen H et al. Stroke 2001;32: Copyright © American Heart Association
. PICH, primary intracerebral hemorrhage; CI, cerebral infarct; and IDS, ill-defined stroke patients. SAH Subarachnoid Hemorrhage. CI Cerebral Infarct. PICH 1o Intracerebral Bleed. IDS Ill Defined Stroke. Brønnum-Hansen H et al. Stroke 2001;32: Copyright © American Heart Association.")
42
A well-designed prospective cohort study of 2447 participants from the Dutch TIA trial found that the risk for major vascular events and stroke was highest shortly after TIA or minor nondisabling stroke, declined to its lowest point at about three years, and then progressively increased over the remainder of the 10-year follow-up (figure 4) [19]. In contrast, the risk for mortality gradually rose throughout the study. By 10 years, 60 percent had died and 54 percent had experienced new vascular events (stroke and myocardial infarction). Event-free survival was 48 percent. Predictive factors for risk of vascular events and death included age over 65 years, diabetes, claudication, previous vascular surgery, and pathologic Q waves on baseline electrocardiogram.
![A well-designed prospective cohort study of 2447 participants from the Dutch TIA trial found that the risk for major vascular events and stroke was highest shortly after TIA or minor nondisabling stroke, declined to its lowest point at about three years, and then progressively increased over the remainder of the 10-year follow-up (figure 4) [19].](http://slideplayer.com/slide/3421875/12/images/42/A+well-designed+prospective+cohort+study+of+2447+participants+from+the+Dutch+TIA+trial+found+that+the+risk+for+major+vascular+events+and+stroke+was+highest+shortly+after+TIA+or+minor+nondisabling+stroke%2C+declined+to+its+lowest+point+at+about+three+years%2C+and+then+progressively+increased+over+the+remainder+of+the+10-year+follow-up+%28figure+4%29+%5B19%5D..jpg "In contrast, the risk for mortality gradually rose throughout the study. By 10 years, 60 percent had died and 54 percent had experienced new vascular events (stroke and myocardial infarction). Event-free survival was 48 percent. Predictive factors for risk of vascular events and death included age over 65 years, diabetes, claudication, previous vascular surgery, and pathologic Q waves on baseline electrocardiogram..")
43
Imaging results frequently encountered by the underwriting staff
3 tests, frequently seen, that I want to discuss in more depth are: CIMT testing Carotid Duplex Ultrasound testing MRI or CT scan which shows the presence of a previous infarct—incidental finding

44
Carotid artery intima-media thickness (CIMT)
CIMT measures the thickness of 2 layers (intima and media) of the carotid artery walls Carotid artery methods are being refined so it is important to know exactly where the artery is being measured (Carotid bulb, common carotid, or internal carotid), near or far walls or both. /S (05) /abstract Thought by some to be an even earlier indicator of atherosclerosis than Coronary artery calcium measurements since thickening precedes a plaque
 of the carotid artery walls. Carotid artery methods are being refined so it is important to know exactly where the artery is being measured (Carotid bulb, common carotid, or internal carotid), near or far walls or both. /S (05) /abstract. Thought by some to be an even earlier indicator of atherosclerosis than Coronary artery calcium measurements since thickening precedes a plaque.")
45
Carotid artery intima-media thickness (CIMT)
Abnormal (“high risk”) frequently defined as media thickness above the 75th percentile. Conflicting evidence whether this test has independent predictive power as compared to usual CV risk factors American Heart Association Position Statement (dated 3/7/12) even suggested this test not be mandated by health insurers as the predictive power hasn’t been established. (Of note however is that they also did not support EBCT measurements whereas there is some evidence this test is helpful, at least in intermediate risk individuals, independently of other tests). In the Multi-Ethnic Study of Atherosclerosis (MESA) which had 6698 subjects aged years CIMT was a modestly better predictor of stroke than EBCT but was not as good as EBCT for CV disease prediction Meta-analysis has shown that serial measurements are not useful for predicting progression.
 frequently defined as media thickness above the 75th percentile. Conflicting evidence whether this test has independent predictive power as compared to usual CV risk factors. American Heart Association Position Statement (dated 3/7/12) even suggested this test not be mandated by health insurers as the predictive power hasn’t been established. (Of note however is that they also did not support EBCT measurements whereas there is some evidence this test is helpful, at least in intermediate risk individuals, independently of other tests). In the Multi-Ethnic Study of Atherosclerosis (MESA) which had 6698 subjects aged years CIMT was a modestly better predictor of stroke than EBCT but was not as good as EBCT for CV disease prediction. Meta-analysis has shown that serial measurements are not useful for predicting progression.")
46
US and MRA

47
Evaluation of the Carotid arteries
Carotid duplex ultrasound frequently performed: 81-98% sensitive 82-89% specific Less precise for stenosis of <50% Less precise for stenosis of 100% Frequently used with MRA or CTA for confirmation of stenosis of >50% or for 100% stenosis. Complete Obstruction: No surgical treatment has been proven to be of benefit. Combo of US and MRA very good at detecting this CTA is also extremely good at detecting this Gold standard is angiography

48
Asymptomatic extracranial carotid artery disease
The 2011 AHA/ASA Guidelines Medical therapy and lifestyle changes should be instituted Population screening for asymptomatic carotid artery stenosis is not recommended Benefit in women is very controversial Prophylactic CEA performed with <3% morbidity and mortality should be considered when: Minimum of 60% occlusion by angiography or >/= 70% occlusion on doppler >80% occlusion on CTA or MRA for those with US showing 50% to 69% stenosis The number to treat (NTT) to prevent 1 stroke over 3 years is 33 Carotid artery stenting can be considered but the advantage over medical therapy is not well established Guidelines for the Prevention of Stroke in Patients With Stroke or Transient Ischemic Attack. A guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Furie, Karen et al. Stroke. 2011; 42:
 to prevent 1 stroke over 3 years is 33. Carotid artery stenting can be considered but the advantage over medical therapy is not well established. Guidelines for the Prevention of Stroke in Patients With Stroke or Transient Ischemic Attack. A guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Furie, Karen et al. Stroke. 2011; 42:")
49
Silent Strokes A not so uncommon incidental finding
Not such good outcomes when found Evaluated in the Cardiovascular Health Study1 Published in 2002 5888 people >/= 65 y/o with normal MRI followed by repeat MRI in 5 years. 17.7% had 1 or more infarct Only 11% had experienced a documented TIA or CVA . Those with + MRI scans showed > decline in Mini-Mental exam test results Evaluated in the Rotterdam Scan study2 Published in 2003 1077 elderly people followed for over 4 years. Silent brain infarcts increased the chance of a subsequent major CVA by 5 times. Those with >1 silent infarct were at the highest risk for a subsequent major CVA. The presence of silent infarcts significantly increased the risk of dementia Silent strokes typically involve small areas of the brain or areas that have tremendous amount of potential for redundancy....not areas like the pre-Rolandic motor cortex area containing the pars opercularis or its connections which would result in Broca’s aphasia. 1. Incidence, manifestations, and predictors of brain infarcts defined by serial cranial magnetic resonance imaging in the elderly: The Cardiovascular Health Study. Longstreth WT et al Stroke. 2002;33(10):2376. 2. Silent brain infarcts and white matter lesions increase stroke risk in the general population: the Rotterdam Scan Study. Vermeer SE, et al, Rotterdam Scan Study Stroke. 2003;34(5):1126
: Silent brain infarcts and white matter lesions increase stroke risk in the general population: the Rotterdam Scan Study. Vermeer SE, et al, Rotterdam Scan Study Stroke. 2003;34(5):")
50
More examples of silent CVA’s
Axial T2-weighted Axial T1-weighted FLAIR Axial Proton Density Main signal characteristics used for defining SBI on different MRI sequences. A–D, A silent brain infarct (SBI) corresponds to CSF signal on all MRI sequences (black arrows). A, Axial T2-weighted; (B) axial T1-weighted; (C) axial fluid-attenuated inversion-recovery (FLAIR); (D) axial proton density. E–H, A hyperintense lesion on T2-weighted images that is moderately hypointense on T1 in the left thalamus (white arrows) is not defined as SBI in studies defining only cavities containing CSF as infarcts, whereas it is diagnosed as an infarct in studies that simply defined hyperintense T2 and hypointense T1 foci as infarcts. E, Axial T2-weighted; (F) axial T1-weighted; (G) axial FLAIR; (H) axial proton density. CSF indicates cerebrospinal fluid. Zhu Y et al. Stroke 2011;42: Copyright © American Heart Association
 corresponds to CSF signal on all MRI sequences (black arrows). A, Axial T2-weighted; (B) axial T1-weighted; (C) axial fluid-attenuated inversion-recovery (FLAIR); (D) axial proton density. E–H, A hyperintense lesion on T2-weighted images that is moderately hypointense on T1 in the left thalamus (white arrows) is not defined as SBI in studies defining only cavities containing CSF as infarcts, whereas it is diagnosed as an infarct in studies that simply defined hyperintense T2 and hypointense T1 foci as infarcts. E, Axial T2-weighted; (F) axial T1-weighted; (G) axial FLAIR; (H) axial proton density. CSF indicates cerebrospinal fluid. Zhu Y et al. Stroke 2011;42: Copyright © American Heart Association.")
51
Summary CVA rates in the US are declining. However, based upon population demographics the total number/year is anticipated to continue to rise Definition changes regarding TIA and CVA will impact mortality numbers There are several types of strokes and multiple etiologies. Regardless of the type there are significant adverse long term mortality concerns Diagnosis of TIA’s and CVA’s can be accomplished with several types of imaging. A diffusion weighted MRI probably is one of the best methods. Quick evaluation is important Primary and secondary treatment depends on the etiology of the stroke but does impact mortality CIMT testing might demonstrate future potential value in underwriting but as an independent cardiac or cerebrovascular disease indicator there are currently conflicting results Carotid US results and the presence of CVA’s found incidentally do help with underwriting

52
CASE 2 cases arrive for underwriter review. Which has the worst mortality risk based upon the following limited information you are provided? Case 1: 66 y/o female with hx. of a “TIA-like” event 4 years ago with no subsequent symptoms. Hx. of hypertension and hyperlipidemia. BMI 30 MRI of the brain WNL. US of the carotids WNL. ECG WNL. CIMT abnormal at >75th percentile for age—no plaque. Case 2: 65 y/o female with no known neurological complaints—past or present Hx. of hypertension and hyperlipidemia. BMI 30 Recent MRI of the brain shows 2 small lacunar infarcts—age unknown US of the carotids WNL ECG WNL CIMT normal

53
The patient has been depressed ever since she began seeing me in 1983.
JOKE TIME AGAIN!! Medical Record Documentation---sometimes words just come out …well, wrong The patient has been depressed ever since she began seeing me in 1983. The patient was to have a bowel resection. However he took a job as a stockbroker instead. The patient has no past history of suicides. The patient left the hospital feeling much better, except for her original complaints.

54
Please use the ? function on your screen to type in a question.
Questions? Questions? Please use the ? function on your screen to type in a question. or call me if you think of questions later (913) Copies of the presentation will be available: On the Website: or By contacting A recording of the webinar should be available in few days: On the Website:
 Copies of the presentation will be available: On the Website: or. By contacting A recording of the webinar should be available in few days: On the Website:")
55
Thank You For Attending Housecalls: Webinar #8 Cerebrovascular Disease
Presented by: William R. Rooney, M.D., VP & Medical Director July 24, 2013

Similar presentations




















