Download presentation
Presentation is loading. Please wait.

1
Elda Baptistelli de Carvalho, MD, PGY-3 University of Toronto
Cervical Spine Trauma Elda Baptistelli de Carvalho, MD, PGY-3 University of Toronto

2
Objectives Clinical indication for each imaging modality
Identify anatomy of cervical spine Approach to C-spine radiography interpretation Classification of spine injuries

3
Who gets radiographs? Midline cervical tenderness
Focal neurologic deficits Altered LOC Evidence of intoxication Painful distracting injury

4
Who gets CT? Dangerous mechanisms/high energy mechanisms:
-fall from elevation = or > 3 feet/5 stairs -axial load to head (diving) -MVC high speed (>100 km/h), ejection -motorized recreational vehicles -bicycle collision
 -MVC high speed (>100 km/h), ejection. -motorized recreational vehicles. -bicycle collision.")
5
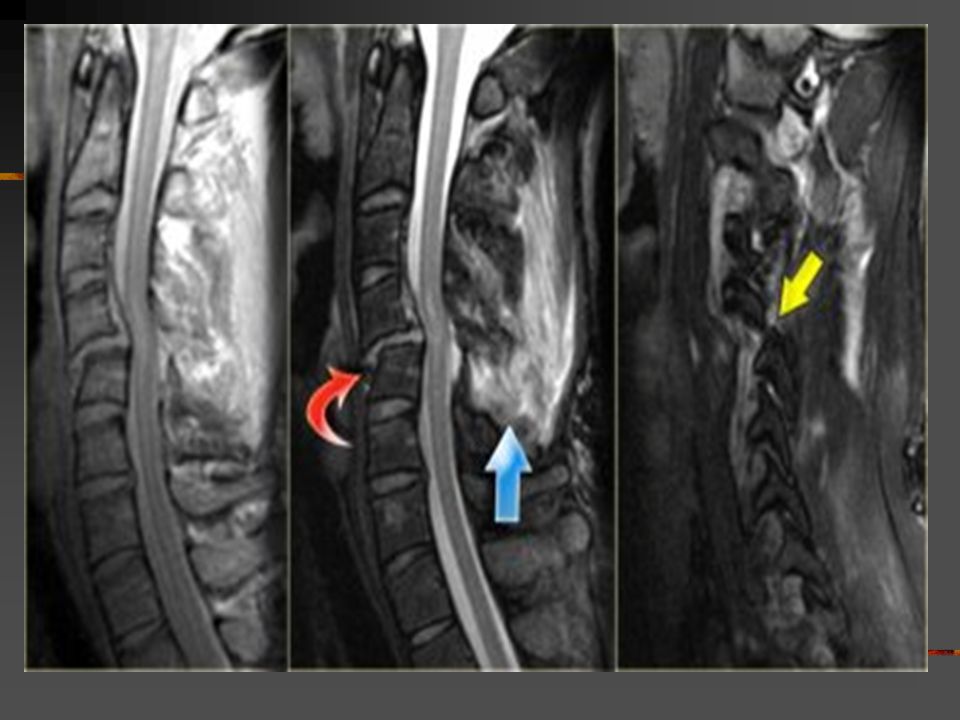
Who gets MRI? Unexplained neurologic symptoms/signs
For visualizing soft tissues, neural elements and unsuspected disk herniation To differentiate cord edema x hemorrhage x infarction To better characterize epidural hematoma

6
Anatomy

7
Approach to C spine radiograph
ABC’S -Adequacy

8
Approach to C spine radiograph
ABC’S -Adequacy

9
Approach to C spine Radiograph
ABC’S -Alignment

10
Approach to C spine Radiography
ABC’S - Bones

11
Approach to C spine radiograph
ABC’S - Cartilage

12
Approach to C spine radiograph
ABC’S -Soft Tissue Rule 2-6 (C2-6 mm) 6-2 (C6-2 cm)
 6-2 (C6-2 cm)")
13
Case 1

14
Case 1

15
Mechanism of Fractures
Hyperflexion Hyperextension Axial Compression

16
Classification

17
Classification By Mechanism of injury /Stability Type of Injury
Fractures Stability Flexion Anterior subluxation Unilateral facet dislocation Bilateral facet dislocation Wedge compression fracture Flexion teardrop fracture Clay Shoveler's fracture Odontoid stable or delayed instability stable unstable stable unstable stable unstable Extension Hangman's fracture Compression Jefferson fracture Burst fracture unstable stable

18
Hyperflexion

19
Case 2

20
Clay shoveler fracture
Stable fracture Hyperflexion ( shoveling snow) Sudden exertion of muscular attachment Avulsion # of spinous process of C7>C6>T1 Rule out extension to lamina, facet #, unilateral jump facet
 Sudden exertion of muscular attachment. Avulsion # of spinous process of C7>C6>T1. Rule out extension to lamina, facet #, unilateral jump facet.")
21
Case 3

26
Unilateral Facet Dislocation
Hyperflexion + rotation Superior facet slides over inferior facet and becomes locked Anterior subluxation of superior vertebral body –25% AP diameter Stable injury 30% with associated neurologic deficit MRI: disk extrusion leading to cord compression

27
Case 4

31
Bilateral Facet Dislocation
Extreme hyperflexion Anterior dislocation of articular masses (disruption of posterior ligament complex,PLL,disk and ALL. Complete dislocation: dislocated vertebra anteriorly displaced ½ of AP diameter of vertebral body Unstable ( high incidence of cord damage)
")
32
Case 5

36
Case 6

39
Flexion Tear Drop Flexion+compression (MVA)
Teardrop fragment comes from the anteroinferior aspect of the vertebral body Larger posterior part displaced backward into the spinal canal Facets joints and interspinous distances usually widened, disk space may be narrowed 70% of patients with neurologic injuries Unstable fracture (complete disruption of ligaments and anterior cord syndrome)
")
40
Hyperextension

41
Case 7

42
Hangman’s fracture Most common cervical spine fracture
Usually hyperextension Diving Unstable, however seldom associated with cord injury (AP diameter of spinal canal greatest at C1/C2 level and # pedicles allow decompression) Hangman’s + uni/bilateral facet dislocation: high rate of neurologic complications
 Hangman’s + uni/bilateral facet dislocation: high rate of neurologic complications.")
43
Types of Hangman #

44
Case 8

47
Hyperextension injury
Widening of disk space anteriorly and narrowing posteriorly “open book” Central cord injury= disproportionated weakness in arms and normal strength in the legs Injuries can be devastating, however are uncommon hemorrhagic

48
Case 9

51
Extension Teardrop Fracture
ALL pulls bony fragment away from inferior aspect of the vertebra because sudden extension Fragment is true avulsion x fragment from flexion teardrop (compression) Diving accidents Lower cervical spine Central cord syndrome (buckling of ligamenta flava into spinal canal) Stable in flexion; highly unstable in extension
 Diving accidents. Lower cervical spine. Central cord syndrome (buckling of ligamenta flava into spinal canal) Stable in flexion; highly unstable in extension.")
52
Case 10

54
Axial Compression

55
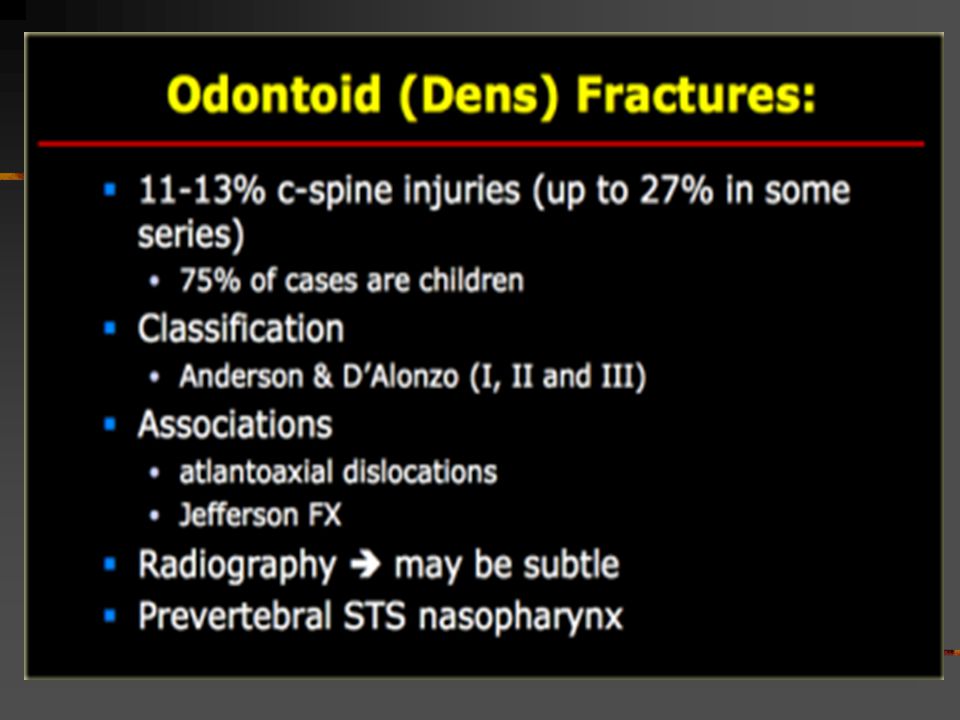
Jefferson Fracture Burst fracture of ring of C1
Axial loading in the occiput No associated neuro deficts ( C1 ring is wide!) Diving, MVA, fall onto height > 2mm dislocation of lateral masses of C1 or odontoid view is diagnostic, 1-2 mm is equivocal ( rotation of head?) Predental space > 3 mm: disruption of transverse ligament 1/3 associated with C2 fracture
 Diving, MVA, fall onto height. > 2mm dislocation of lateral masses of C1 or odontoid view is diagnostic, 1-2 mm is equivocal ( rotation of head ) Predental space > 3 mm: disruption of transverse ligament. 1/3 associated with C2 fracture.")
56
Case 11

59
Atlanto-Occipital Dislocation
Very rare in surviving patients More common in Kids Hyperextension+distraction Disruption of tectorial ligaments CR: rule of 12: tip of dens-basion Basion-post line< 12mm Atlanto-occipital condyle distance<5mm

60
Summary Be systematic (follow ABC’S!!!!)
Know anatomy and mechanism of trauma If dangerous mechanism-CT Unexplained neuro symptoms-MRI Don’t clear C spine on call if not sure!!

61
References http://www.wheelessonline.com/ortho
Emergency Radiology-Schwartz Primer to Diagnostic Imaging

Similar presentations