Download presentation
Presentation is loading. Please wait.

1
Transfusion Thresholds in the Elderly Surgical Patient
Transfusion Medicine Journal Club Shuen Tan ~ anesthesiologist, skeptic, and budding blood conservationist ~ January 8, 2009

2
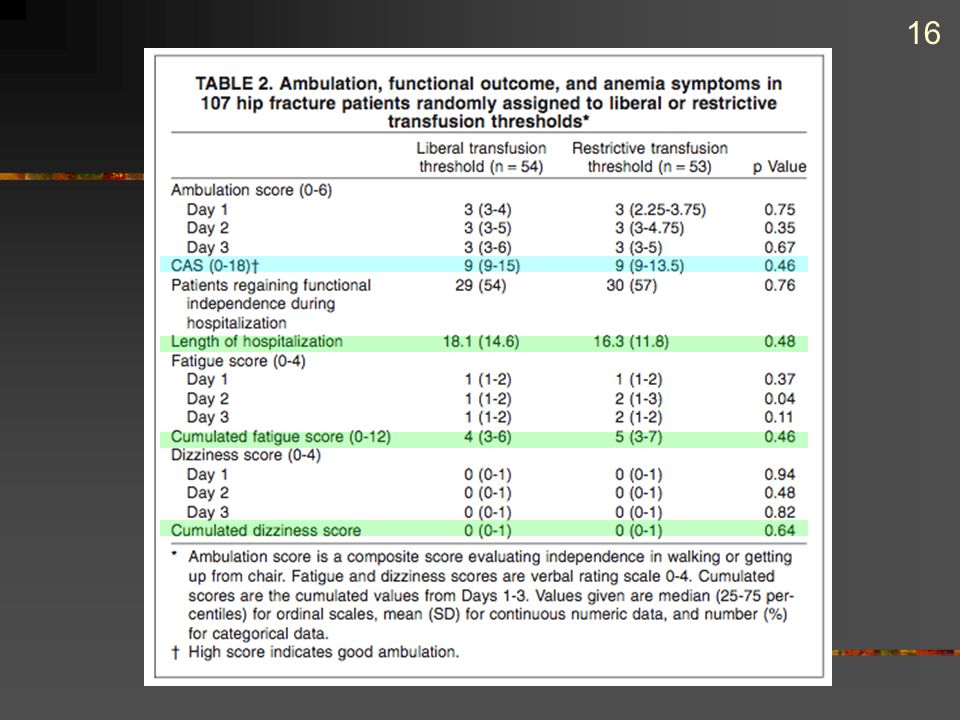
The effects of liberal versus restrictive transfusion thresholds on ambulation after hip fracture surgery Foss, NB, Kristensen MT, Jensen PS, Palm H, Krasheninnikoff M, Kehlet H Transfusion epub (accepted for publication August 25, 2008)
")
3
The Issues Is age a disease?
If so, what is old? How do surgical patients differ from medical patients? How does that affect decisions to transfuse?

4
“There’s chronological age and there’s physiological age.”
- Amit Chopra

5
Physiologic effects of age
Decrease in physiological reserve “This decline is evident by the third decade and is gradual and progressive, although the rate and extent of decline vary.” Cardiovascular Hypotensive response to HR, hypovolemia, or arrhythmia CO/HR response to stress Harrison’s 16th ed., pp , 2005

6
Physiologic effects of age
Respiratory V/Q mismatch lung elasticity, chest wall compliance resting pO2 MSK/Neuro Osteopenia Stiffer gait, body sway Harrison’s 16th ed., pp , 2005

7
Transfusion thresholds
TRICC Sick but not bleeding No difference in mortality with Hb vs Surgical patients Bleeding but not sick Dilutional anemia / Fluid shifts Guidelines vague, depending on clinical situation Hebert et al., NEJM 1999; 340: 409 Nuttall et al., Anesthesiology 2006; 105: 198

8
Methods Prospective, single-centre (Denmark), randomized, double-blind study Hip fracture patients February 2004 to July 2006 Inclusion criteria: Primary hip #, age >65, independent walking pre-fracture, community dwelling, intact cognition

9
Exclusion criteria Multiple #s, terminal condition, alcoholism, chronic transfusion, acute cardiac or severe medical condition, contraindication to neuraxial block Post-op immobilization, transfer for medical complications, return to OR within 4 days

10
Methods Powered to show 25% reduction in CAS with =0.05 and power of 0.80 Assumed 69% transfusion rate with liberal threshold 120 patients, 60 in each arm Liberal group transfused at Hb<10 g/dL Restrictive group transfused at Hb<8 g/dL

11
Methods Standardized perioperative care
Standardized fluid therapy by weight Hb on admission, in PACU, and OD x 5 Intraop PRN only Allocation revealed only if Hb<10, to attending physician only

12
Outcomes Primary Secondary CAS analyzed per-protocol
Length of stay, cardiac complications, infectious complications, 30-day mortality Measured by intention-to-treat Anemia score by PT

13
The Cumulated Ambulation Score (CAS)
Locally developed and validated Length of stay, time to discharge, 30-day mortality, and major medical complications decreased with CAS >9 Numerical representation of patient’s functional mobility Three parameters assessed on 3-pt. scale Max score = 6 Cumulated over POD 1-3 Predictive of postop rehabilitation outcome Foss, Clin Rehabil 2006; 20:701.

14
Results Demographics More patients with ASA 3 in restrictive group (p=0.02) More pins/screws in restrictive group (0.05) More SHS and IMHS in liberal group (0.02) Predictive of increased blood loss (?) IMHS and pins/screws are outliers DHS and arthroplasty similar for blood loss Foss and Kehlet, J Bone Joint Surg Br 2006; 88: 1053
 Predictive of increased blood loss ( ) IMHS and pins/screws are outliers. DHS and arthroplasty similar for blood loss. Foss and Kehlet, J Bone Joint Surg Br 2006; 88:")
15
Results Transfusion More patients exposed in liberal group (74% vs. 37%) More transfusions in liberal group (p<0.0001)
 More transfusions in liberal group (p<0.0001) .")
18
Mortality 5 patients, all in restrictive group No pre-op CV disease
3 CV deaths 1 sudden death 1 “general exhaustion”

19
Validity

20
Well-defined patient population Restrictive group “sicker” at baseline
1. Were there clearly defined groups of patients, similar in all important ways other than exposure to the treatment? Well-defined patient population Restrictive group “sicker” at baseline Larger proportion of ASA 3 patients Surgeries similar in intention-to-treat analysis More SHS and IMHS in liberal group Blood loss similar

21
“You’re forgetting the two most important determinants of intraoperative blood loss -- the surgeon and the anesthesiologist.” - Brian Muirhead

22
Technically double-blind Clinical and subjective assessment of anemia
2. Was the assessment of outcomes either objective or blinded to exposure? Technically double-blind Patient and PT unaware of allocation Clinical and subjective assessment of anemia Attending physician aware of transfusion group Interaction with PT Lab reports on chart or computer?

23
Primary outcome measured over 3 days
3. Was the follow-up of the study patients sufficiently long and complete? Primary outcome measured over 3 days Validated to predict longer-term outcome Secondary outcomes measured (presumably) over hospital stay 30 days for mortality Follow-up complete for all patients ~10% of patients excluded from per-protocol analysis
 over hospital stay. 30 days for mortality. Follow-up complete for all patients. ~10% of patients excluded from per-protocol analysis.")
24
4. Do the results fulfill some of the diagnostic tests for causation?
Did the exposure preceed the outcome? Probably, but timing of transfusion not reported Is there a dose-response gradient? Not reported Is there any positive evidence from a dechallenge-rechallenge study? Is the association consistent from study to study? One previous study also showed no difference in ambulation with restrictive threshold 60-day mortality in restrictive group: RR = 2.5 Carson et al. Transfusion 1998; 38:522

25
Does the association make biological sense?
Plausible that increased Hb might lead to less fatigue, less CV complications, and less delirium, thus better ambulation Hb values were similar throughout study despite different thresholds Ambulation may be related more to multimodal rehab

27
Multimodal Post-Fracture Rehab
Dedicated hip fracture unit Surgery within 24 hours Epidural at admission until 96 hours post-op Supplemental O2 while supine Perioperative LMWH Enforced perioperative nutrition and hydration Intensive PT starting POD 0 Foss et al. Clin Rehabil 2006; 20:701 Foss and Kehlet. J Bone Joint Surg Br 2006; 88:1053

28
Are the results of this study important?

29
What is the magnitude and precision of the association between the exposure and outcome?
Primary outcome identical (CAS 9) Range similar between groups Harm in restrictive group CV events: 10% vs. 2%, p=0.05 30-day mortality: RR = 2.1, p=0.02 Infectious complications: p = 0.19 Length of stay: p = 0.61
 Range similar between groups. Harm in restrictive group. CV events: 10% vs. 2%, p=0.05. 30-day mortality: RR = 2.1, p=0.02. Infectious complications: p = Length of stay: p =")
30
Mortality 5 patients, all in restrictive group
No pre-existing CV disease 3 CV conditions 1 sudden death, unexplained 1 “general exhaustion”

31
Can this study be applied to our patients?

32
1. Are our patients so different from those in the study that the results don’t apply?
The uppermost echelon of hip fracture patients Dr. Shuen’s broken hips Nursing home Moderate dementia Walkers and wheelchairs Anemic, cachectic, CV disease, anticoagulated, etc…. 500 patients screened for inclusion

34
Benefits of avoiding transfusion
2. What is our patient’s risk of an adverse event, and potential benefit from the therapy? Average hip fracture patients at higher risk of CV complications than those in the study Risk difficult to quantify Unknown if raising transfusion threshold would mitigate risk Benefits of avoiding transfusion TRALI and TACO in susceptible population Coagulopathy Wound healing and infection?

35
3. What alternative treatments are available?
Emergent surgery, limited time to optimize pre-op Hb Other blood conservation Early surgery, Cell-saver, anti-fibrinolytics, limited blood draws, nutritional supplements Aggressive multi-modal rehab Increased monitoring and index of suspicion for CV events

36
Summary Liberalizing transfusion thresholds for elderly hip fracture patients does not improve post-op ambulation Restrictive thresholds may put patients at higher risk of CV morbidity/mortality Any benefit associated with transfusion may be outweighed by the benefits of multimodal rehabilitation

Similar presentations












 patients Policy.>")









