Download presentation
Presentation is loading. Please wait.

1
A pitvari fibrilláció (ablációs) kezelése
Pap Róbert SZTE

2
Elbocsátási aritmia-diagnózisok

3
The solid curve indicates the projected increase in AF prevalence if no further increase in AF incidence occurs. The dotted curve indicates the increase in AF prevalence if the increase in incidence rate continues to rise to a similar extent as it rose between 1980 and 2000.

4
Prevalencia

6
Nathan H, Eliakim M. The junction between the left atrium and the pulmonary
veins. An anatomic study of human hearts. Circulation 1966;34:412– 422. Mechanizmus Jalife J, Berenfeld O, Mansour M. Mother rotors and fibrillatory conduction: a mechanism of atrial fibrillation. Cardiovasc Res 2002;54:204 –216. Ectopic foci vs. circus movement activity. Moreover, these investigators estimated that maintenance of fibrillation in the canine atrium required a The exact mechanisms underlying AF are still poorly critical number of four to six wavelets. Some support of understood despite many years of research and speculation. this idea came from the pharmacological experiments of As early as 1907, Winterberg [11] surmised that AF was Wang and co-workers [17,18] in which termination of due to multiple rapidly firing foci distributed throughout atrial fibrillation by class IC antiarrhythmic drugs was the atria. In 1914, Mines [12] advanced the circus move- preceded by a decrease in the mean number of wavelets. ment theory of reentry. Thereafter, and until the late Subsequent experiments in dogs [19], as well as more 19509s, all of the hypotheses proposed to explain AF were recent intra-operative mapping studies in humans [20], variations of the circus movement and ectopic focus have provided important insight into the characteristics of theories [13,14]. However, following publication of the wave front propagation during fibrillation, and have given multiple wavelet hypothesis by Moe and Abildskov [10], it support to Moe’s idea that multiple wavelets distributed became generally accepted that AF was the result of the randomly throughout the atria gave rise to the seemingly random propagation of multiple wavelets across the atria, a chaotic activation patterns observed in the electrocarprocess that was thought to be independent of the initiating diograms of patients with AF. Finally, the hypothesis was event. emboldened by the clinical observation that chronic AF could be cured in some patients by the placement of 2.2. Multiple wavelets vs. circus movement multiple surgical lesions (MAZE) to compartmentalize the atria into regions presumably unable to sustain the multiple Moe and Abildskov [10] strongly argued that both the wavelets [21]. Indeed, this theory is virtually universally ectopic focus and circus movement reentry notions were accepted by most clinical electrophysiologists today. inadequate descriptions of AF. For them it was hard to However, none of the above-mentioned studies gave believe that either mechanism could be endowed with the answers to many critical questions about the origin of the necessary stability to persist for many years as AF turbulent activity that gave rise to the multiple wavelets in commonly does. Thus, they proposed that the mechanism the experiments. For example, while the computer simulaof AF, whether occurring spontaneously in man or pro- tions of Moe et al. [15] suggested that 15–30 wavelets duced experimentally, was fundamentally different from were needed at a given time to keep the fibrillatory process flutter and from automatic ectopic discharge. In 1964, Moe going, the experiments of Allessie et al. [16] could show et al. published their classical computer model study on only 4–6 wavelets propagating on the surface of the dog AF [15]. Based on that numerical study and on their heart. In the presence of such a small number of wavelets, previous experimental results [10], they postulated that AF one would expect that, at any given time, a large amount could exist as a stable state, self-sustained and independent of tissue in both atria would be recovered from previous of its initiating agency, and also that an independent excitation, which would lead to coalescence of wavelets survival of the arrhythmia was possible only in the and eventual termination of AF. In other words, it is presence of inhomogeneous atrial repolarization enhanced reasonable to speculate that, in the experiments of Allessie by adequate vital activity. The idea of Moe et al. was et al. [16], the arrhythmia could have been in fact the result simple. They considered fibrillation to be a fundamentally of a single (or a small number of) high frequency source turbulent and self-sustaining process, which takes place in that was (were) hidden from view. Additional questions a non-homogeneous excitable medium. Such a process include the following: is spontaneously occurring fibrillacould be initiated by an impulse propagating through the tion the result of a ‘‘mother rotor’’ that breaks and medium at a time when some of its components have fractionates into multiple independent offspring? What are recovered while others remain partially or fully refractory the fundamental structural and electrophysiological characas a result of a preceding activation. Accordingly, some teristics that sustain the wavelets and which enable their elements in the medium may Moe GK, Rheinboldt WD, Abildskov JA. A computer model of atrial fibrillation.Am Heart J 1964:200 –220. 6
 to compartmentalize the. atria into regions presumably unable to sustain the multiple. Moe and Abildskov [10] strongly argued that both the wavelets [21]. Indeed, this theory is virtually universally. ectopic focus and circus movement reentry notions were accepted by most clinical electrophysiologists today. inadequate descriptions of AF. For them it was hard to However, none of the above-mentioned studies gave. believe that either mechanism could be endowed with the answers to many critical questions about the origin of the. necessary stability to persist for many years as AF turbulent activity that gave rise to the multiple wavelets in. commonly does. Thus, they proposed that the mechanism the experiments. For example, while the computer simulaof. AF, whether occurring spontaneously in man or pro- tions of Moe et al. [15] suggested that 15–30 wavelets. duced experimentally, was fundamentally different from were needed at a given time to keep the fibrillatory process. flutter and from automatic ectopic discharge. In 1964, Moe going, the experiments of Allessie et al. [16] could show. et al. published their classical computer model study on only 4–6 wavelets propagating on the surface of the dog. AF [15]. Based on that numerical study and on their heart. In the presence of such a small number of wavelets, previous experimental results [10], they postulated that AF one would expect that, at any given time, a large amount. could exist as a stable state, self-sustained and independent of tissue in both atria would be recovered from previous. of its initiating agency, and also that an independent excitation, which would lead to coalescence of wavelets. survival of the arrhythmia was possible only in the and eventual termination of AF. In other words, it is. presence of inhomogeneous atrial repolarization enhanced reasonable to speculate that, in the experiments of Allessie. by adequate vital activity. The idea of Moe et al. was et al. [16], the arrhythmia could have been in fact the result. simple. They considered fibrillation to be a fundamentally of a single (or a small number of) high frequency source. turbulent and self-sustaining process, which takes place in that was (were) hidden from view. Additional questions. a non-homogeneous excitable medium. Such a process include the following: is spontaneously occurring fibrillacould. be initiated by an impulse propagating through the tion the result of a ‘‘mother rotor’’ that breaks and. medium at a time when some of its components have fractionates into multiple independent offspring What are. recovered while others remain partially or fully refractory the fundamental structural and electrophysiological characas. a result of a preceding activation. Accordingly, some teristics that sustain the wavelets and which enable their. elements in the medium may. Moe GK, Rheinboldt WD, Abildskov JA. A computer model of atrial fibrillation.Am Heart J 1964:200 –")
7
Pitvari fibrilláció kezelése
Frekvencia-kontroll Ritmus-kontroll - Gyógyszeres (béta-blockoló, Ca-antagonista, digoxin) - Gyógyszeres Nem-gyógyszeres: AV csomó abláció + pacemaker Nem-gyógyszeres Anticoaguláns kezelés
 - Gyógyszeres. Nem-gyógyszeres: AV csomó abláció + pacemaker. Nem-gyógyszeres. Anticoaguláns kezelés.")
9
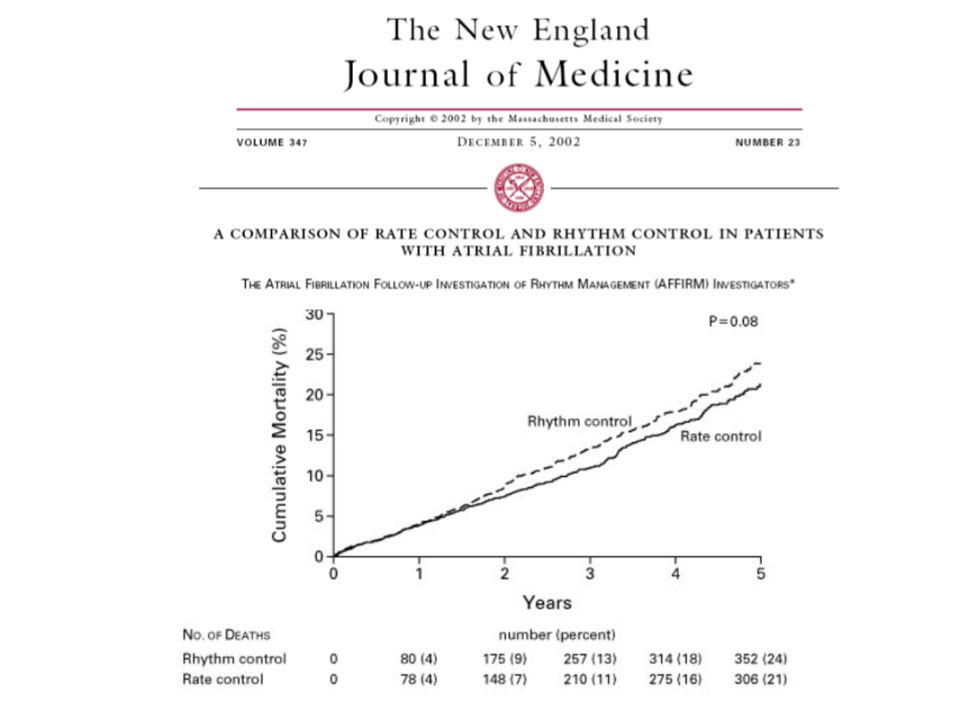
Frekvencia- vagy ritmus-kontroll?

10
Circulation 2004 Covariates Significantly Associated With Survival p
HR Age at enrollment* <0.0001 1.06 Coronary artery disease <0.0001 1.65 Congestive heart failure <0.0001 1.83 Diabetes <0.0001 1.56 Stroke or transient ischemic attack <0.0001 1.54 Smoking <0.0001 1.75 First episode of atrial fibrillation 0.0067 1.27 Sinus rhythm <0.0001 0.54 Warfarin use <0.0001 0.47 Digoxin use <0.0001 1.50 Rhythm-control drug use 0.0005 1.41 Circulation 2004

11
Patients Without Recurrence (%)
Ritmus-kontroll? CTAF Study 100 Amiodarone (n = 201) 80 60 Propafenone (n = 101) Patients Without Recurrence (%) 40 Sotalol (n = 101) 20 0.0 100 200 300 400 500 600 Days of Follow-up Roy D, et al. New Engl J Med. 2000;342:913–920.
 Propafenone (n = 101) Patients Without Recurrence (%) 40. Sotalol (n = 101) Days of Follow-up. Roy D, et al. New Engl J Med. 2000;342:913–920.")
12
Cox maze III.

13
1998 Haissaguerre NEJM

14
NEJM 1998

16
Fokális abláció

18
Pulmonális véna izoláció

19
Pulmonális véna izoláció

24
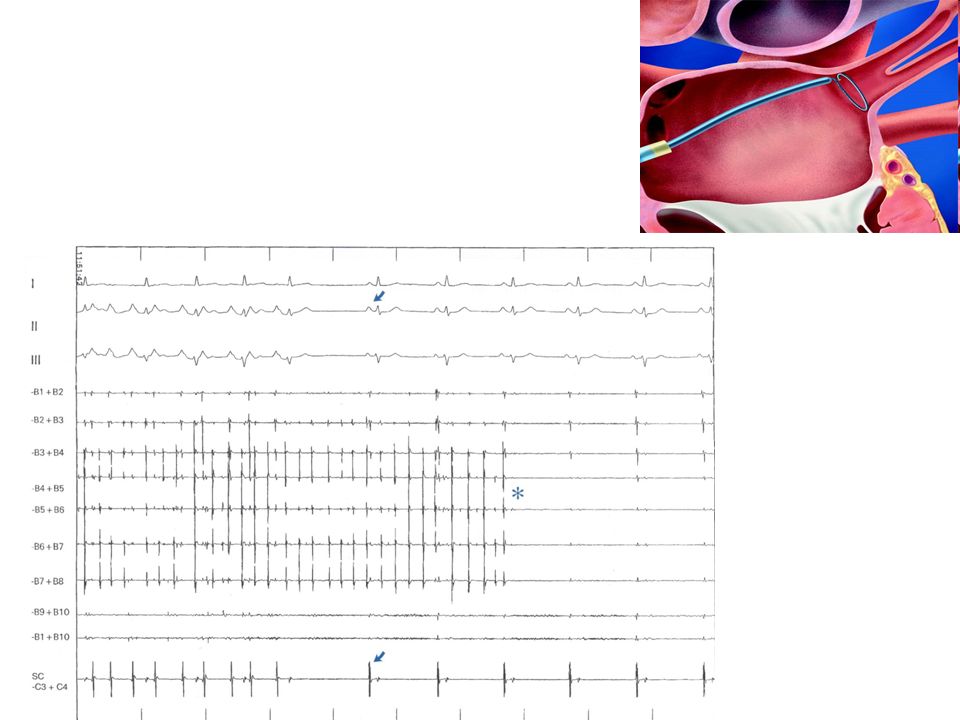
Beavatkozás Anticoaguláns terápia TEE
Intracardialis echocardiographia (ICE)
")
25
ICE

26
ICE

27
CS LS RA Map/Abl AF indukció * 27

29
II LS 1,2 LS 2,3 LS 3,4 LS 4,5 LS 5,6 LS 6,7 LS 7,8 LS 8,9 LS 9,10 Abl
CS 9,10 CS 5,6 CS 1,2

30
Katéter-abláció

31
Késői rekurrencia: 24% Nincs rekurrencia Rekurrencia (N=32) (N=10) p
Persist. AF 16% 50% 0,026 Amio 28% 30% 0,909 Hypertonia 63% 0,482 Diabetes 22% 20% 0,900 ISZB 6% 10% 0,688 Valvularis 3% 0,012 Bal pitvar 49 mm 51 mm 0,468 Bal kamra 54 mm 55 mm 0,373 EF 64% 0,813 Életkor 52 év 60 év 0,031 Előzmény 6,25 év 5,8 év 0,831

33
Randomized Trial of Radiofrequency Ablation versus Antiarrhythmic Drugs as First-Line Treatment of Symptomatic Atrial Fibrillation (RAAFT) JAMA 2005

34
Ablation for Paroxysmal Atrial Fibrillation (APAF) trial
JACC 2006

35
Catheter ablation versus antiarrhythmic drugs for atrial fibrillation: the A4 study.
cca. 40% required a second ablation Circulation 2008

36
Candidates in whom to consider first-line ablation for atrial fibrillation
From: Verma: Curr Opin Cardiol, Volume 23(1).January –8
.January –8.")
37
dronedarone

40
CHADS2 score Condition Points C Congestive heart failure 1 H
Hypertension (or treated hypertension) A Age >75 years D Diabetes S2 Prior Stroke or TIA 2
 A. Age >75 years. D. Diabetes. S2. Prior Stroke or TIA. 2.")
41
CHADS score Treatment with Coumadin reduces the risk of stroke in atrial fibrillation by about 2/3 (66%,) and treatment with aspirin reduces the risk by 1/4 (25%). The risk that anticoagulation will produce a major bleeding episode varies depending on the patient's medical problems and the care with which the protime or INR (i.e., the "thinness" of the blood) is monitored, but generally is less than 1 - 2% per year. Based on all this information, the developers of the CHADS model recommend strongly considering therapy with Coumadin for anybody whose CHADS score is 1 or higher. Certainly, most patients with CHADS scores of 2 or higher stand a strong chance of benefitting from anticoagulation. Precautions in using the CHADS model The CHADS model was developed by studying the records of 1733 Medicare beneficiaries aged 65 to 95, and in this age group the model appears very accurate at predicting stroke risk. How well the CHADS model works for younger patients is not entirely clear, however, since the data was gathered for elderly patients. The model is not valid at all for individuals with the valve disease called mitral stenosis - these patients have a very high risk of stroke, and virtually all of them should take anticoagulation therapy. 41
. The risk that anticoagulation will. produce a major bleeding episode varies depending on the patient s medical problems and the. care with which the protime or INR (i.e., the thinness of the blood) is monitored, but. generally is less than 1 - 2% per year. Based on all this information, the developers of the CHADS model recommend strongly. considering therapy with Coumadin for anybody whose CHADS score is 1 or higher. Certainly, most patients with CHADS scores of 2 or higher stand a strong chance of benefitting from. anticoagulation. Precautions in using the CHADS model. The CHADS model was developed by studying the records of 1733 Medicare beneficiaries aged. 65 to 95, and in this age group the model appears very accurate at predicting stroke risk. How well the CHADS model works for younger patients is not entirely clear, however, since the. data was gathered for elderly patients. The model is not valid at all for individuals with the. valve disease called mitral stenosis - these patients have a very high risk of stroke, and. virtually all of them should take anticoagulation therapy. 41.")
43
Dabigatran

Similar presentations






























 discharge, and … does not apply to ventricular.>")

, MS (Cardiology)>")
