Download presentation
Presentation is loading. Please wait.

1
Common Pediatric Orthopedic Clinical Problems
Saunders Jones Jr. MD

2
Common Pediatric Orthopedic Problems
Metabolic Developmental Congenital Traumatic Infectious Neoplastic Neuromuscular

3
Radiological “hole in the bone”
Fibrous cortical defect Aneurysmal Bone cyst “bone island” Giant cell tumor Infection Ewing’s Sarcoma Enchondroma

4
Fibrous cortical defect (Fibroxanthoma)
")
5
Unicameral bone cyst Next to growth plate Active vs Inactive
Falling leaf sign

6
ABC Aneurysmal bone cysts may occur in patients aged years, with a peak incidence in those aged 16 years. About 75% of patients are younger than 20 years. Four phases of pathogenesis are recognized, as follows: Osteolytic initial phase Active growth phase, which is characterized by rapid destruction of bone and a subperiosteal blow-out pattern Mature stage, also known as stage of stabilization, which is manifested by formation of a distinct peripheral bony shell and internal bony septae and trabeculae that produce the classic soap-bubble appearance. Healing phase with progressive calcification and ossification of the cyst and its eventual transformation into a dense bony mass with an irregular structure.

7
ABC

9
Ewing's Sarcoma

10
Incidence of Ewings

11
Ewings

12
Giant Cell tumor Not ped age group

13
Osteochondromas or Multiple Exostoses
Cartilaginous cap covered by a bursa Impinge on local structures CT shows cap < 1cm in thickness Can be excised due to structural problems SMALL incidence (<1% per lesion) of transformation to Chondro sarcoma (or Osteogenic less common)
 of transformation to Chondro sarcoma (or Osteogenic less common)")
14
Multiple Exostoses Found in areas around growth plates
Can occur in multiple locations or singularly Usually not Neoplastic Bone with cartilaginous cap Grows normally with growth of the rest of the skeleton

15
Osteochondromas B9 Cartilaginous cap Impinges on local structures

16
Osteochondromas Another view

17
Osteochondroma

18
Osteochondroma

19
Osteochondroma microscopic

20
Osteosarcoma

21
Osteosarcoma Some bone elements

22
Enchondroma

23
Non ossifying Fibroma

24
Metabolic Pediatric Category
Rickets Osteogenesis Imperfecta

25
Rickets Radiologic changes in the growth plate Vitamin problem

26
Osteogenesis Imperfecta

28
Twisty Bendy Feet Most common is metatarsus adductus
FPS fetal packaging syndrome Normal rotation of feet in utero Should respond to gentle massage and SWN Shoes could be worn in reverse (r-l l-r) if there is any “last” in the shoe
 if there is any last in the shoe.")
29
Metatarsus adductus/clubfoot (tell tale medial crease)
")
30
Twisty Bendy Feet Clubfeet “talipes equino-varus”
Metatarsus adductus, heel equinus and varus and talus adductus Tell tale crease on lat underneath malleolus Thinning and atrophy of lower leg Needs attention based on severity of deformity, START TREATMENT AT BIRTH !!! Refer early

31
Club feet Metatarsal Talus Hindfoot Leg atrophy

32
Endstage Club feet

33
Clubfoot casting In the nursery or soon as possible

34
Club foot Casting Must go above the knee to control rotation
Plaster is the best Soak off night before Manipulation and then maintenance of that correction

35
Limited clinic Tenotomy
New

36
Twisty Bendy legs

37
Twisty Bendy Legs Internal Tibial Torsion
Normal adult rotation is degrees external Normal unwinding of child's lower legs Not significantly affected by orthotics or treatment !!! Sight along tibial crest and look at malleoli Reassure (look for other conditions)
")
38
Twisty Bendy Legs Bendy knees/legs 2-4-6 years
Genu varus / genu valgus Normal variants Radiographs for Blount’s Disease Vitamins Orthotics (?)
")
39
Blount’s vs. Normal

40
Twisty Bendy Legs Femoral anteversion
Femur is turned in at the hip causing “pigeon towed gait” Sit on their feet SWN Education Twister cables!!?!?!?!?

41
Femoral anteversion

43
Pes Planus “flat feet” Common in infants and up to about 8 years of age Painful flat feet is different…tarsal coalition or other condition Some pes planus is genetic or racial Look at mom’s feet!!!

44
Heel Pain in Adolescent
Sever’s Disease Calcaneal apophysitis X rays show “fractionation” Symptomatic tx with NSAIDs Stretching Limitation of activity ?

45
Sever’s Disease

46
Xray of the Calcaneal Apophysis

47
Stretch for Sever’s Disease

48
Knee Pain in Adolescent
Anterior tibial tubercle pain Osgood-Schlatter’s disease Tibial apophysitis Rest stretching Ice Nsaids Prominent tubercle Hereditary tendencies HIP PAIN MASQUERADES AS KNEE PAIN !!!!! Always xray same side hip!!!

49
Anterior Knee pain Adolescent Female
Increased valgus with tracking problems Squatting and Indian style sitting Quad sets and Nsaids VMO? Usually self limited Make sure nothing else going on…..

50
OSDx and Ant knee pain

51
Osgood Schlatter's

52
Osgood Schlatter’s Disease

53
Hip Pain SCFE Transient synovitis Hip pyarthrosis LCP

54
Slipped Capital Femoral Epiphysis
SCFE Endomorphic Androgenital Onset anterior thigh pain Externally Rotated Gait Can be bilat Rx pin in situ

55
SCFE

56
SCFE

57
SCFE

58
LCP Perthe’s Disease Avascular necrosis of the proximal femoral growth plate Collapse Maintain concentricity and “containment” Multiple bouts of Transient synovitis

59
LCP initial and resorptive phases

60
LCP resorptive and remodeling

61
Congenital Dislocated Hip
Barlow's Ortilani Duration and treatment Age of child at discovery Pavlick harness Closed reduction and casting Open Reduction Subtrochanteric osteotomy Acetabular osteotomy

62
Congenital Dislocation

63
Congenital Hip Dislocation

64
Causes of Hip Pain in Children
CDH 0-2 years 1:4 m:f 20%bilat LCP 4-8 years 5:1 m:f 10% bilat SCFE 10-15 years 1.5:1 m:f 25-40%bilat

65
Idiopathic Adolescent Scoliosis
Not a painful condition If there is pain…look for another cause! OBJECTIVE OF TREATMENT: To prevent deformity as adult Skeletal maturity Onset of menses, Risser sign Criteria for referral relates to progression BracesSurgery runs the gamut

67
Risser sign

68
Risser Sign

69
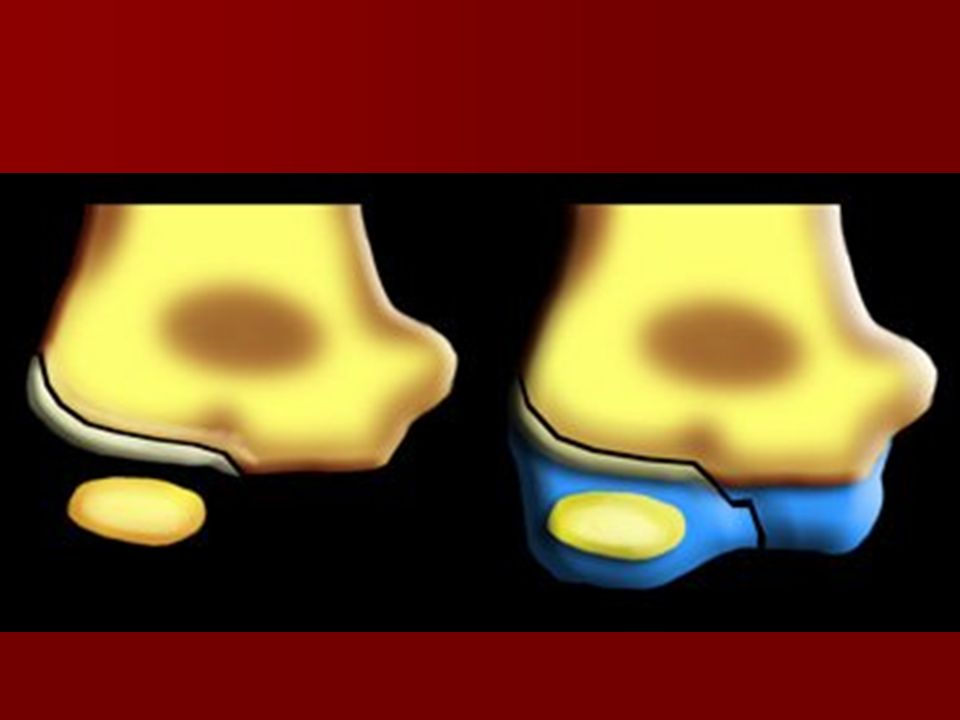
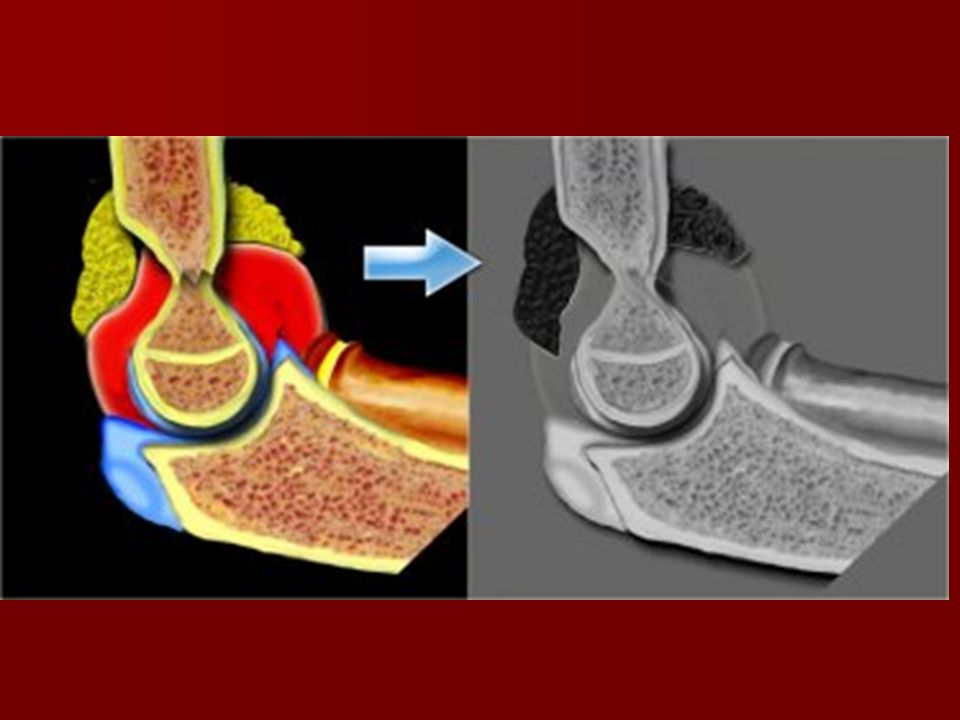
Nursemaids Elbow

70
Nursemaids Elbow

71
Falls from a Height common in Children

73
Epiphyseal Injuries: only in kids!!!
Salter classification Joint involvement Growth disturbance Thick periosteum

74
Salter One

76
Salter 2

77
Salter 3

78
Salter 4

79
Salter 5

82
Supracondylar elbow fractures
Compartment syndrome because of vascular compromise Characteristic fx due to the shape of the supracondlyar region of the humerus “balancing two canoes”

87
Lines around the elbow

89
Supracondylar fx minimal displacement

90
Displaced Supracondylar fx

91
Medial Epicondyle fx

93
Lateral condyle Salter #?

94
Supracondylar fx

95
Radial Head fxs

96
Displaced Lateral condyle Salter #?

97
Radial Head Fx displaced epiphyseal….Salter# ?

98
Late Sequelae Cubitus varus

99
Fracture Tx in Kids Alignment has different criteria Overgrowth
Maintenance of overall alignment most important Rotation, etc

100
Fracture Tx in Younger Kids (growth potential)
")
101
Overall Alignment and Residual Growth

102
Fracture Tx in Older Kids

103
Fracture Tx in Even Older Kids

104
Neuromuscular Category
Cerebral Palsy Spastic or Flaccid Birth injury Perinatal cerebral anoxia Hyperactive stretch receptors Contractures Releases, Transfers, Braces etc.

105
Infections Joints Pyarthrosis Infants and young children
Endemic Otitis Media No good lab test X-rays normal Patho-anatomy growth plate vasculature Drain and decompress because of potential damage to cartilage May lead to Osteomyelitis

106
ANY QUESTIONS??? Comments Discussion

107
Thank you

Similar presentations












 – A NEW APPROCH AND OUR EXPERIENCE Kamenetsky Natalya (1), Rachmilewitz Eliezer.>")

>")





 normal cell of origin Most are classified.>")









 female with significant right shoulder pain and rihgt upper extremity.>")
