Download presentation
Presentation is loading. Please wait.

1
New directions in programming: Choosing frequency allocation tables for postlingually deaf CI users
Mario A. Svirsky Dept. of Otolaryngology New York University School of Medicine

2
Do postlingually deaf patients adapt completely to the standard frequency allocation tables?

3
Hypotheses 1) Human listeners can adapt to frequency-shifted auditory input, even when there’s spectral degradation 2) Some listeners may not adapt completely 3) Individual differences in the ability to adapt completely may have clinical implications and may be addressed by appropriate signal processing.
 Some listeners may not adapt completely. 3) Individual differences in the ability to adapt completely may have clinical implications and may be addressed by appropriate signal processing.")
4
Four methods to measure adaptation to frequency tables
1) Pitch matching 2) Mathematical modeling of vowel identification 3) Perceptual vowel space 4) Self selection of “most intelligible” frequency table
 Pitch matching. 2) Mathematical modeling of vowel identification. 3) Perceptual vowel space. 4) Self selection of most intelligible frequency table.")
5
Four methods to measure adaptation to frequency tables
1) Pitch matching 2) Mathematical modeling of vowel identification 3) Perceptual vowel space 4) Self selection of “most intelligible” frequency table 5
 Pitch matching. 2) Mathematical modeling of vowel identification. 3) Perceptual vowel space. 4) Self selection of most intelligible frequency table. 5.")
6
Method 1: Electroacoustic pitch matching
Most apical electrode (#22), Nucleus device. Range= Hz Center=250 Hz Postlingually deaf adults with different amounts of post-implant experience. Data from three different laboratories.
, Nucleus device. Range= Hz Center=250 Hz. Postlingually deaf adults with different amounts of post-implant experience. Data from three different laboratories.")
8
Electroacoustic pitch matching- all electrodes
Six repetitions per electrode Alternating stimulation to each ear Acoustic frequency adjusted by the listener Randomized starting frequency Acoustic stimuli presented at comfortably loud level (when possible)
")
9
Chin-Tuan Tan Ben Guo (did not submit picture)
")
10
Bilateral pitch ranking with very different insertion depths- Case 1
Two Advanced Bionics devices: normal insertion in left ear, only five active electrodes active in right ear (significant bone drillout). Right ear had Ineraid device that was explanted; significant bone growth at the time of reimplantation. Each electrode in the partial insertion ear was pitch ranked 2 to 5 times to each electrode in the full insertion ear. Non-simultaneous presentation Electrode in the full insertion ear was randomized. Similar (standard) frequency tables in both ears. 3 years right; 9 years left.
. Right ear had Ineraid device that was explanted; significant bone growth at the time of reimplantation. Each electrode in the partial insertion ear was pitch ranked 2 to 5 times to each electrode in the full insertion ear. Non-simultaneous presentation. Electrode in the full insertion ear was randomized. Similar (standard) frequency tables in both ears. 3 years right; 9 years left.")
11
11

12
Matthew Fitzgerald 4 mm Left CI: Full Length 2.2 mm 479 Hz 1440 Hz
Right CI: Shallow 479 Hz 1440 Hz 12

13
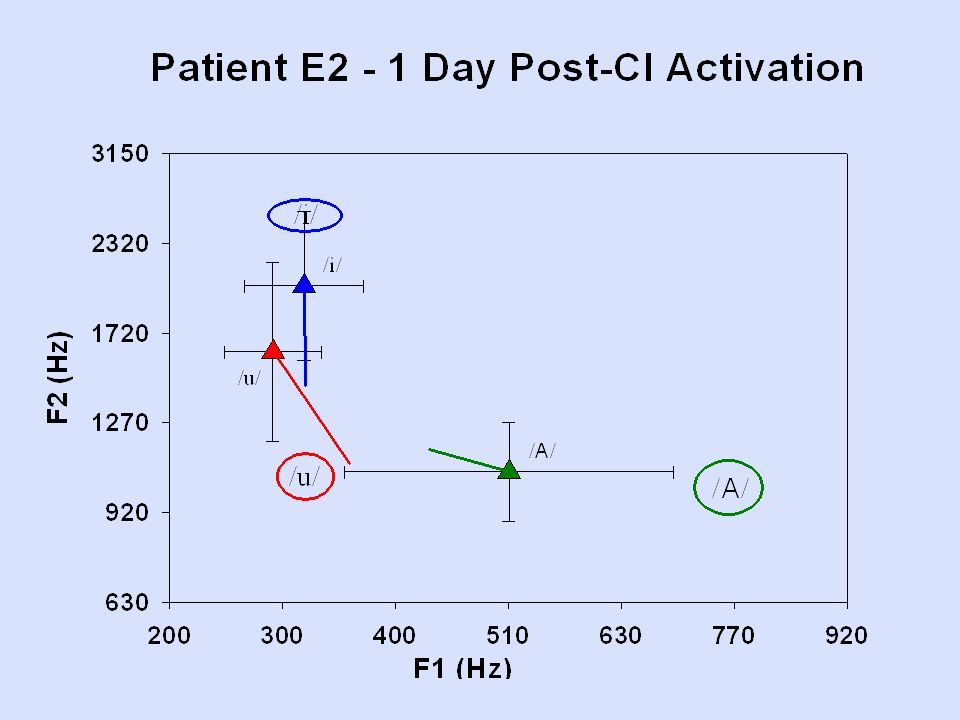
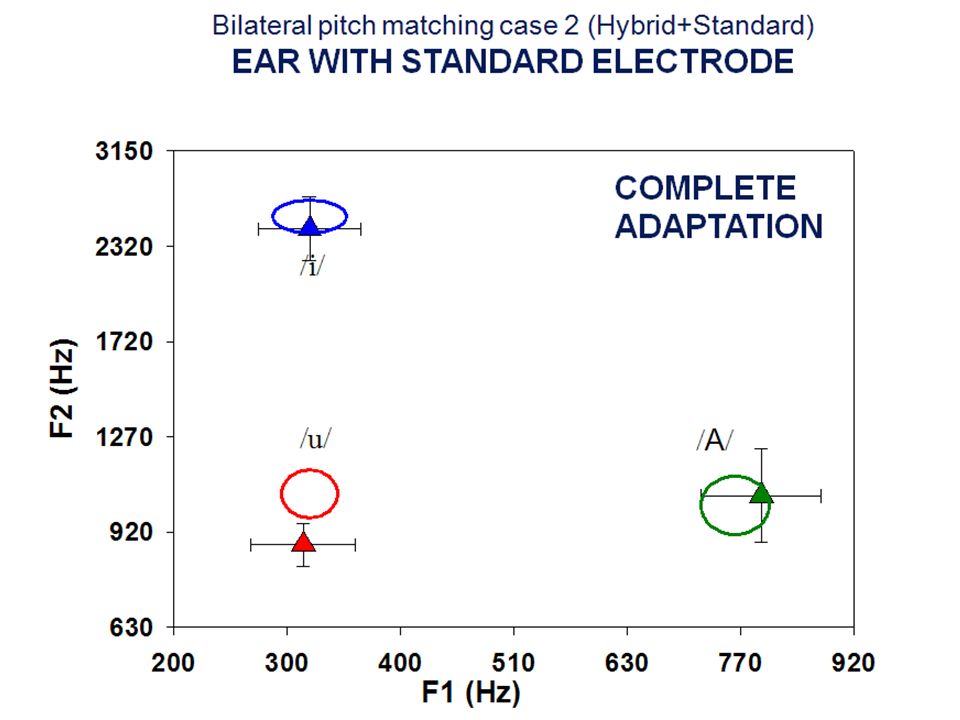
Bilateral pitch ranking with very different insertion depths- Case 2
Patient with residual hearing received Hybrid-S 10 mm electrode in the left ear. Two years after the Hybrid implantation she lost residual hearing in both ears and was then implanted with a standard electrode (24 mm) in the right ear. After loss of residual hearing and standard electrode implantation, both processors were programmed with the standard frequency table: Hz. At the time of the Reiss et al. study (Ear and Hearing, 2011) she had 2-3 years of experience with these frequency tables. She was also tested in our laboratory when she had six years of experience with the standard frequency tables in both ears.
 in the right ear. After loss of residual hearing and standard electrode implantation, both processors were programmed with the standard frequency table: Hz. At the time of the Reiss et al. study (Ear and Hearing, 2011) she had 2-3 years of experience with these frequency tables. She was also tested in our laboratory when she had six years of experience with the standard frequency tables in both ears.")
14
Reiss et al. Ear & Hearing 2011 7.8 mm
3760 Hz 325 Hz 3 mm 3760 Hz 325 Hz 14

15
CONCLUSIONS-METHOD 1 Pitch matching
Pitch matching did not always line up with frequency allocation table Electroacoustic pitch matching of most apical electrode, or all electrodes. Pitch matching across CI ears with different insertion depths. There is significant adaptation, but it is not always complete, despite years of experience.

16
Four methods to measure adaptation to frequency tables
1) Pitch matching 2) Mathematical modeling of vowel identification 3) Perceptual vowel space 4) Self selection of “most intelligible” frequency table 16
 Pitch matching. 2) Mathematical modeling of vowel identification. 3) Perceptual vowel space. 4) Self selection of most intelligible frequency table. 16.")
17
Method 2: Mathematical modeling of vowel identification
Mathematical models of vowel confusion data allow us to measure the mismatch between: Places of maximal stimulation along the cochlea for a given vowel Places along the cochlea where the patient expects to be stimulated Qualitative description of Sagi et al (2010) 17
 17.")
18
Fu et al. experiment Three postlingually deaf adults users of SPEAK strategy. 4-6 years of experience. Three months of experience with new frequency table Table 1 Table 7 Table 9 CF CF CF CF CF CF CF CF CF CF CF CF CF CF CF CF CF CF CF CF CF

19
Fu et al. results

20
Sagi E, Fu QJ, Galvin JJ 3rd, Svirsky MA. JARO 2010
Elec Freq. 1 1 300 2 507 3 702 4 975 5 1326 6 1756 7 2263 8 2848 9 3512 10 4254 11 5073 12 5971 13 6947 14 8000 Elec. Freq. 2 1 150 2 260 3 396 4 587 5 833 6 1133 7 1488 8 1897 9 2361 10 2880 11 3453 12 4081 13 4764 14 5500 11 10 9 8 7 6 5 F1 1 2 3 4 5 20

21
CONCLUSIONS-METHOD 2 Mathematical modeling
CI users show adaptation after they receive a modified frequency allocation table. This adaptation may not be complete even after they reach asymptotic speech perception scores. Correct pitch matching is necessary but not sufficient to achieve complete adaptation.

22
Four methods to measure adaptation to frequency tables
1) Pitch matching 2) Mathematical modeling of vowel identification 3) Perceptual vowel space 4) Self selection of “most intelligible” frequency table 22
 Pitch matching. 2) Mathematical modeling of vowel identification. 3) Perceptual vowel space. 4) Self selection of most intelligible frequency table. 22.")
23
Method 3: Perceptual vowel space
A case of complete adaptation and a case of incomplete adaptation to standard frequency tables. Perceptual vowel space data from one of the asymmetric insertion patients 23

42
CONCLUSIONS-METHOD 3 Perceptual vowel space
Some listeners adapt completely to the standard frequency tables; others don’t. A similar statement can be made about different ears for the same listener.

43
Four methods to measure adaptation to frequency tables
1) Pitch matching 2) Mathematical modeling of vowel identification 3) Perceptual vowel space 4) Self selection of “most intelligible” frequency table Ist part: describe model 2-5 I will show how the MPI model explains vowel and consonant identification by CI users with different types of speech processors 5- In addition, I will show how the MPI model can be used to provide quantitative estimates of auditory plasticity in response to a modified frequency map in the audotiry periphery. This will be the “perceptual learning” part of the talk. 43
 Pitch matching. 2) Mathematical modeling of vowel identification. 3) Perceptual vowel space. 4) Self selection of most intelligible frequency table. Ist part: describe model. 2-5 I will show how the MPI model explains vowel and consonant identification by CI users with different types of speech processors. 5- In addition, I will show how the MPI model can be used to provide quantitative estimates of auditory plasticity in response to a modified frequency map in the audotiry periphery. This will be the perceptual learning part of the talk. 43.")
44
Current Clinical Practice
We give every cochlear implant patient the same frequency-to-electrode map. Is this optimal? For postlingually deaf patients, probably not. -We give every cochlear implant patient the same frequency-to-electrode map. -Is this optimal? For postlingually deaf patients, probably not. -Over time, do patients adapt to frequency shifts or distortions? -Is this adaptation complete? -current fitting involved activating/deactivating electrodes.

45
Current Surgical Practice
Variation in position of electrodes, size of cochleas, neurons being stimulated Nucleus which manual? Adv Bionics – for

46
Cochleas come in different sizes
Hardy (1938)- cochlear size can vary by as much as 40%. Stakhovskaya et al. (2007): SGN frequency map. 24 mm from the base 76 Hz in a 28 mm cochlea 1,020 Hz in a 42 mm cochlea 10 mm from the base 3,450 Hz 6,100 Hz
- cochlear size can vary by as much as 40%. Stakhovskaya et al. (2007): SGN frequency map. 24 mm from the base. 76 Hz in a 28 mm cochlea. 1,020 Hz in a 42 mm cochlea. 10 mm from the base. 3,450 Hz. 6,100 Hz.")
47
COCHLEAS COME IN DIFFERENT SIZES
Average basilar membrane length is about 35 mm, but it can range from 28 mm to 42 mm. Estimated CF of SG cells in a cochlea of length= Distance from base L=28 mm L=42 mm 24 mm 76 Hz 1020 Hz 10 mm 3450 Hz 6100 Hz

48
Evidence suggesting one size does not fit all (frequency tables)
Skinner et al. (2002)- correlation between insertion depth and speech perception. Kos et al. (2007), Gani et al. (2007), Shapiro, Roland, Waltzman (2007)- overinsertion, electrode deactivation, too much bass.
- correlation between insertion depth and speech perception. Kos et al. (2007), Gani et al. (2007), Shapiro, Roland, Waltzman (2007)- overinsertion, electrode deactivation, too much bass.")
49
Take an analogy from our opthalmology colleagues
Same prescription – improve (don’t say all do pretty well)
")
50
Basic idea: power to the patient (or to the audiologist)
Selection of frequency-to-electrode maps may be done in real time while the patient “turns a knob” to maximize the intelligibility of running speech. This real-time tool may allow: Faster comparison of different maps Better comparison

51
NEW PARADIGM We have developed PC-based fitting methods that allow very quick (or even real-time) adjustment of frequency maps. This system can be used with cochlear implant users, or with simulations for normal hearing listeners.

52
Change blindness demo

55
Method 4: Self selection of “most intelligible” frequency table
Listeners are asked to select the frequency table that makes speech sound “most intelligible”. Assumption: when a listener has adapted completely, he selects his everyday frequency table. Two methods: RTStream for Advanced Bionics patients and Gridstream for Nucleus patients. Ist part: describe model 2-5 I will show how the MPI model explains vowel and consonant identification by CI users with different types of speech processors 5- In addition, I will show how the MPI model can be used to provide quantitative estimates of auditory plasticity in response to a modified frequency map in the audotiry periphery. This will be the “perceptual learning” part of the talk. 55

56
REAL TIME SPEECH PROCESSING SYSTEM
Technical assistance and equipment from Advanced Bionics (Abhijit Kulkarni) and Cochlear Americas (Chris van den Honert). Adam Kaiser, MD Mehmet Aras Mohamed El-Sharkawy, PhD Ben Stelle Shivank Sinha Tasnim Morbiwala Ravi Rayala Megha Daga Chin-Tuan Tan, PhD Mario Svirsky, PhD
 and Cochlear Americas (Chris van den Honert). Adam Kaiser, MD. Mehmet Aras. Mohamed El-Sharkawy, PhD. Ben Stelle. Shivank Sinha. Tasnim Morbiwala. Ravi Rayala. Megha Daga. Chin-Tuan Tan, PhD. Mario Svirsky, PhD.")
57
Total frequency range audible by humans
RTStream- real time selection of frequency maps Active filter bank 57

59
Self-selection of most intelligible frequency table-2
Frequency table parameters change depending on which square is selected. Pt RK 59

60
Subject #1 74yo M with hearing loss of unknown etiology, having used a CI for 14 months prior to testing Comfortably auditioned maps Selected one equivalent to the standard map he had been using for years Channel Standard Map Self Selected 1 188 – 313 2 313 – 438 3 438 – 563 4 563 – 688 … Pt RK

61
Subject #2 74yo F with hearing loss of unknown etiology, using a CI for 23 months prior Also quickly explored the 2D space Selected a map similar, but different from her standard map Channel Standard Map Self Selected 1 2 313 – 438 3 438 – 563 4 563 – 688 … Pt RK

62
Subjects #3, 4, 5 #3 choose 4,3 (standard map) Subj#4 - 4,1
 Subj#4 - 4,1")
63
FREQUENCY TABLE SELECTION “The player lost a shoe”
“This may be the clearest, may be the first choice” Svirsky et al., 2011 188-18,000 “That’s a REAL sh!” “Sounds very high pitched” “The ‘sh’ is pretty good here but not the best” “shoe sounds like sue and the ‘p’is not there” This is a small amount of data from ***. He said that his standard frequency table ( , left column) makes things sound very high pitched, much more so than the acoustic side. The column to the right represents a frequency table that extends almost to 10 KHz rather than 8 KHZ, and it makes things sound lower pitched than the standard table (yes, sounds counterintuitive at first but that’s the way it works: if you want things to sound lower pitched you need to shift your frequency table to a higher frequency)
 makes things sound very high pitched, much more so than the acoustic side. The column to the right represents a frequency table that extends almost to 10 KHz rather than 8 KHZ, and it makes things sound lower pitched than the standard table (yes, sounds counterintuitive at first but that’s the way it works: if you want things to sound lower pitched you need to shift your frequency table to a higher frequency)")
64
NULL HYPOTHESIS: complete adaptation
64

65
Self-selected frequency tables for users of the Nucleus device
65

66
Self-selected frequency tables for users of the Advanced Bionics device
66

67
ACUTE CHANGE IN SPEECH PERCEPTION SCORES

68
CONCLUSIONS-METHOD 4 Self selection of “most intelligible” frequency table
CI users can comfortably self select their preferred frequency to electrode table. For about half of them, this table is different from the standard frequency table, again suggesting incomplete adaptation in these listeners. Even in an acute setting, self selected maps may allow better speech perception for some CI users (2 or 4 out of 13). Adaptation to the standard frequency tables may be more difficult in cases of insertions that are either too deep or too shallow.
. Adaptation to the standard frequency tables may be more difficult in cases of insertions that are either too deep or too shallow.")
69
A few case studies of adaptation (or lack thereof) to frequency allocation tables
Reimplantation of Hybrid-S users Asymmetric electrode insertion across ears Excessively deep insertion Ist part: describe model 2-5 I will show how the MPI model explains vowel and consonant identification by CI users with different types of speech processors 5- In addition, I will show how the MPI model can be used to provide quantitative estimates of auditory plasticity in response to a modified frequency map in the audotiry periphery. This will be the “perceptual learning” part of the talk. 69

70
1) SPEECH PERCEPTION IN HYBRID PATIENTS REIMPLANTED WITH A STANDARD ELECTRODE
 SPEECH PERCEPTION IN HYBRID PATIENTS REIMPLANTED WITH A STANDARD ELECTRODE")
71
2) SPEECH PERCEPTION IN PATIENTS WITH STRONGLY ASSYMETRIC ELECTRODE INSERTION
 SPEECH PERCEPTION IN PATIENTS WITH STRONGLY ASSYMETRIC ELECTRODE INSERTION")
72
ACUTE CHANGE IN SPEECH PERCEPTION SCORES

73
3) EXCESSIVELY DEEP INSERTION?
Electrode 1 initial surgery High frequencies Electrode 1 regular placement

74
Electrode 1 High frequencies William Shapiro J. Thomas Roland, Jr.
regular placement

75
3) EXCESSIVELY DEEP INSERTION?
 EXCESSIVELY DEEP INSERTION")
76
Overall Conclusions Taken together, data obtained with four different methods suggest that postlingually deaf CI users have a remarkable ability to adapt to a given frequency allocation table. However, adaptation may be not always be complete, depending on the interplay between frequency range, insertion depth and cochlear size. 76

77
Overall conclusions Self selection of frequency tables (and possibly other parameters) is clinically feasible and may be beneficial for some patients. 77
 is clinically feasible and may be beneficial for some patients. 77.")
78
SOME QUESTIONS Who adapts completely and who doesn’t?
Why do some patients fail to achieve complete adaptation? Is there something we can do about it? 78

79
Auditory Brainstem Implants
Are placed in the cochlear nucleus Are used for patients with a compromised auditory nerve (e.g., NF2)
")
80
ABI surface electrode Kanowitz et al., 2004

81
ABI do help speechreading
Schwarz et al., 2008

82
In non-NF2 patients, ABI provides open-set speech understanding
Colletti and Shannon, 2005

83
QUESTIONS ABOUT ABIs Why do ABI users with NF2 do so much worse that cochlear implant users? Why do non-tumor ABI users do so much better than NF2 ABI users? Why do children with ABIs do so poorly (not shown)?
")
84
FINAL COMMENTS Clinical interest : successful replacement of a human sense. Scientific interest: platform to answer basic questions about human communication. Translational and multidisciplinary research. Many unanswered questions.

85
Acknowledgments This work has been supported by NIDCD (PIs: Chin-Tuan Tan, Matthew Fitzgerald, Arlene Neuman, Mario Svirsky), NIDRR (PI: Elad Sagi) and the AAO-HNS (PI: D. Jethanamest). Cochlear Americas and Advanced Bionics have loaned equipment, software, and provided technical advice to this project. We also acknowledge the invaluable assistance of NYU’s Cochlear Implant Center, its Co-Directors J. Thomas Roland, MD and Susan B. Waltzman, PhD, its chief audiologist, William Shapiro, AuD, and the staff. 85
, NIDRR (PI: Elad Sagi) and the AAO-HNS (PI: D. Jethanamest). Cochlear Americas and Advanced Bionics have loaned equipment, software, and provided technical advice to this project. We also acknowledge the invaluable assistance of NYU’s Cochlear Implant Center, its Co-Directors J. Thomas Roland, MD and Susan B. Waltzman, PhD, its chief audiologist, William Shapiro, AuD, and the staff. 85.")
86
Acknowledgments This work has been supported by NIDCD (PIs: Chin-Tuan Tan, Matthew Fitzgerald, Arlene Neuman, Mario Svirsky), NIDRR (PI: Elad Sagi) and the AAO-HNS (PI: D. Jethanamest). Cochlear Americas and Advanced Bionics have loaned equipment, software, and provided technical advice to this project. We also acknowledge the invaluable assistance of NYU’s Cochlear Implant Center, its Co-Directors J. Thomas Roland, MD and Susan B. Waltzman, PhD, its chief audiologist, William Shapiro, AuD, and the staff. Arlene Susan Neuman Waltzman 86
, NIDRR (PI: Elad Sagi) and the AAO-HNS (PI: D. Jethanamest). Cochlear Americas and Advanced Bionics have loaned equipment, software, and provided technical advice to this project. We also acknowledge the invaluable assistance of NYU’s Cochlear Implant Center, its Co-Directors J. Thomas Roland, MD and Susan B. Waltzman, PhD, its chief audiologist, William Shapiro, AuD, and the staff. Arlene Susan. Neuman Waltzman. 86.")
87
Acknowledgments The tools for selection of frequency allocation tables described here are patented. The author has not received any royalties from this IP and has pledged to his university that any future royalties will be donated to charity, to avoid conflicts of interest. 87

88
The end

89
From Reiss et al. Ear & Hearing 2011
89

90
90

Similar presentations


























 HAWKES LEARNING SYSTEMS math courseware specialists Copyright © 2008 by Hawkes Learning Systems/Quant.>")











