Download presentation
Presentation is loading. Please wait.

1
Stefania Maggi CNR Center on Aging Padua, Italy
Diabetes and Vitamin D Stefania Maggi CNR Center on Aging Padua, Italy In this lecture we will review the current state of knowledge regarding the role of vit D in the pathogenesis of diabetes.

2
Diabetes and Vitamin D Vitamin D metabolism and actions
Epidemiology of hypovitaminosis D Association of low Vitamin D status and chronic diseases Association of low vitamin D and diabetes: epidemiological evidence, pathophysiological plausibility, efficacy of interventions

3
Early in the 20th century it was shown that rickets could be prevented by a fat soluble factor D in the diet or by the exposure of the body to U.V. light. In plants a commonly occurring steroid, “ergosterol” can be activated by irradiation to ergocalciferol (vitamin D2), the antirachatic compound most commonly used in supplements. Cholecalciferol”(vitamin D3), is primarily in animal foods such as eggs, liver, butter, fatty fish, fortified milk and margarine. Dietary vitamin D is absorbed from the G.I. tract efficiently with fat and bile salts. In the intestinal cells, vit D is incorporated into chylomicrons and transported in the blood with chylomicrons remnants, delivering the vitamin to the liver. 7-dehydrocholesterol is synthesized in the sebaceous glands of the skin, secreted onto the surface and reabsorbed into the epidermis. During exposure to the sunlight, some of the epidermal reservoir of 7dehydrocholesterol is converted to “previtaminD3”. The previtamin D3 is then thermally isomerized within 2-3 days into vitamin D3 (cholecalciferol), diffuses from the skin and is transported in the blood with vitamin D-binding protein (DBP) and then delivered to the liver. Cholecalciferol reaching the liver either by chylomicron remnants or by DPB, is hydroxylated into 25-OH D3. The efficiency of the liver enzyme 25-hydroxylase to convert cholecalciferol into 25-OH D3 is related to the vitamin D status. Most of the 25-OH D3 made in the liver is secreted into the blood and transported by DBP. The blood is the largest single pool of 25-OH D3.25-OH D3 bound to DBP in the blood is transported to the kidney, where it is hydroxylated to 1,25 (OH)2D3 the “active vitamin D” by an enzyme 25-OH, D3-1 alpha hydroxylase or “1-hydroxylase”.
, the antirachatic compound most commonly used in supplements. Cholecalciferol (vitamin D3), is primarily in animal foods such as eggs, liver, butter, fatty fish, fortified milk and margarine. Dietary vitamin D is absorbed from the G.I. tract efficiently with fat and bile salts. In the intestinal cells, vit D is incorporated into chylomicrons and transported in the blood with chylomicrons remnants, delivering the vitamin to the liver. 7-dehydrocholesterol is synthesized in the sebaceous glands of the skin, secreted onto the surface and reabsorbed into the epidermis. During exposure to the sunlight, some of the epidermal reservoir of 7dehydrocholesterol is converted to previtaminD3 . The previtamin D3 is then thermally isomerized within 2-3 days into vitamin D3 (cholecalciferol), diffuses from the skin and is transported in the blood with vitamin D-binding protein (DBP) and then delivered to the liver. Cholecalciferol reaching the liver either by chylomicron remnants or by DPB, is hydroxylated into 25-OH D3. The efficiency of the liver enzyme 25-hydroxylase to convert cholecalciferol into 25-OH D3 is related to the vitamin D status. Most of the 25-OH D3 made in the liver is secreted into the blood and transported by DBP. The blood is the largest single pool of 25-OH D3.25-OH D3 bound to DBP in the blood is transported to the kidney, where it is hydroxylated to 1,25 (OH)2D3 the active vitamin D by an enzyme 25-OH, D3-1 alpha hydroxylase or 1-hydroxylase .")
4
The primary function of calcitriol or 1,25 (OH)2D3 in the intestine is increased absorption of calcium and phosphorous. Vitamin D is carried into the nucleus of the enterocyte, where it binds to receptor proteins and acts as a steroid hormone, resulting in the stimulation and synthesis of new messenger RNA molecules. These messenger RNA molecules are then translated to produce a protein, Calbindin, a calcium binding protein in the intestinal mucosa that is synthesized in response to the action of calcitriol (active vit. D). This calcium binding protein is needed for Ca transport across the cell membranes
. This calcium binding protein is needed for Ca transport across the cell membranes.")
5
Calcitriol and the Bone:
PTH, alone or with calcitriol, directs the mobilization of Ca and P from the bones to help achieve a normal blood Ca concentration. The body’s needs for calcium is regulated by the production of calcitriol by the kidneys. “Hypocalcemia” increases the secretion of parathyroid hormone, which in turn: a) Stimulates the conversion of some of the circulating 25(OH)2D3 to 1,25(OH)2D3 (calcitriol) in the kidneys. b) This active 1,25(OH)2D3 (calcitriol) then causes elevation of serum Ca and P by acting on kidney, bone, and G.I. Tract
 Stimulates the conversion of some of the circulating 25(OH)2D3 to 1,25(OH)2D3 (calcitriol) in the kidneys. b) This active 1,25(OH)2D3 (calcitriol) then causes. elevation of serum Ca and P by acting on kidney, bone, and G.I. Tract.")
6
Vitamin D metabolism and actions
Maalouf NM, Current opinion in Nephrology and hypertension, 2008

7
Diabetes and Vitamin D Vitamin D metabolism and actions
Epidemiology of hypovitaminosis D Association of low Vitamin D status and chronic diseases Association of low vitamin D and diabetes: epidemiological evidence, pathophysiological plausibility, efficacy of interventions

8
25(OH)D concentrations (ng/mL)
Suggested terminology to describe vitamin D status according to circulating 25(OH)D concentrations Stages of vitamin D status 25(OH)D concentrations (ng/mL) Deficiency 0–12 Insufficiency >12–30 Adequacy >30 to 100 Toxicity >100 Souberbielle JC et al, Autoimmune reviews, 2010
D concentrations. Stages of vitamin D status. 25(OH)D concentrations (ng/mL) Deficiency. 0–12. Insufficiency. >12–30. Adequacy. >30 to 100. Toxicity. >100. Souberbielle JC et al, Autoimmune reviews,")
9
Causes of hypovitaminosis D
Reduced skin synthesis Sunscreen use, skin pigment, aging, season, latitude Decreased bioavailability Malabsorption, obesity Increased catabolism Antconvulsants, glucocorticoids (binding to the steroid receptor) Breast feeding Poor vit D content in human milk Decreased synthesis of 25(OH)D Liver failure Increased urinary loss of 25(OH)D Nephrotic syndrome Decreased synthesis of 1,25(OH)D Chronic kidney failure
 Breast feeding. Poor vit D content in human milk. Decreased synthesis of 25(OH)D. Liver failure. Increased urinary loss of 25(OH)D. Nephrotic syndrome. Decreased synthesis of 1,25(OH)D. Chronic kidney failure.")
10
Hypovitaminosis D: a global perspective
80% in aged, 42% in adolescents 35-73% 89% in adolescents Midle East and Africa register the highest rates of hypovitaminosis D worldwide. Turkish, Moroccan, Indian and Sub-Sahara African immigrants in Europe have higher level of hypovitaminosis D compared to indigenous European populations 30-80% 50-97% Bandeira et al, Arq Bras Endocrinol Metab 50, Mithal et al, Osteop Int, 2009 Van der Meer M et al, Ospeop Int, 2011

11
The lowest values were found in Greece, Spain, and Italy
Serum 25(OH)D measured in elderly people in 16 European centers participating in the Euronut SENECA Study. The lowest values were found in Greece, Spain, and Italy Lips, P. Endocr Rev 2001;22: Copyright ©2001 The Endocrine Society
D measured in elderly people in 16 European centers participating in the Euronut SENECA Study. The lowest values were found in Greece, Spain, and Italy. Lips, P. Endocr Rev 2001;22: Copyright ©2001 The Endocrine Society.")
12
Diabetes and Vitamin D Vitamin D metabolism and actions
Epidemiology of hypovitaminosis D Association of low Vitamin D status and chronic diseases Association of low vitamin D and diabetes: epidemiological evidence, pathophysiological plausibility, efficacy of interventions

13
Vitamin D deficiency Rickets--------------Children
Osteomalacia Adults Osteoporosis Adults ……….. And much more!!

14
Vitamin D deficiency

15
Dobnig H et al, Arch Intern Med. 2008;168(12):1340-1349.
Independent Association of Low Serum 25-Hydroxyvitamin D Levels With All-Cause and Cardiovascular Mortality Dobnig H et al, Arch Intern Med. 2008;168(12): Prospective cohort study of 3258 patients undergoing coronary angiography Dobnig, H. et al. Arch Intern Med 2008;168: Copyright restrictions may apply.
: Prospective cohort study. of 3258 patients undergoing. coronary angiography. Dobnig, H. et al. Arch Intern Med 2008;168: Copyright restrictions may apply.")
16
associated with all-cause and CVD mortality
Cox proportional hazards regression model ratios (including 95% confidence intervals [CI]) for cardiovascular mortality are shown for 25-hydroxyvitamin D (A) and 1,25-dihydroxyvitamin D (B) quartiles (Q) for the following 3 different statistical models (M): (1) M1 (unadjusted), (2) M2 (adjusted for age, sex, body mass index, and physical activity level), and (3) M3 (variables of M2 plus active smokers, diabetes mellitus, albumin level, cystatin C level, triglyceride level, N-terminal pro-BNP level, systolic and diastolic blood pressure, low-density lipoprotein and high-density lipoprotein cholesterol levels, and the use of statins, aspirin, -blockers, bronchodilators, and angiotensin-converting enzyme inhibitors) Low 25-hydroxyvitamin D and 1,25-dihydroxyvitamin D levels are independently associated with all-cause and CVD mortality Dobnig, H. et al. Arch Intern Med 2008;168: Copyright restrictions may apply.
 for cardiovascular mortality are shown for 25-hydroxyvitamin D (A) and 1,25-dihydroxyvitamin D (B) quartiles (Q) for the following 3 different statistical models (M): (1) M1 (unadjusted), (2) M2 (adjusted for age, sex, body mass index, and physical activity level), and (3) M3 (variables of M2 plus active smokers, diabetes mellitus, albumin level, cystatin C level, triglyceride level, N-terminal pro-BNP level, systolic and diastolic blood pressure, low-density lipoprotein and high-density lipoprotein cholesterol levels, and the use of statins, aspirin, -blockers, bronchodilators, and angiotensin-converting enzyme inhibitors) Low 25-hydroxyvitamin D and 1,25-dihydroxyvitamin D levels are independently. associated with all-cause and CVD mortality. Dobnig, H. et al. Arch Intern Med 2008;168: Copyright restrictions may apply.")
17
Data From the Third National Health and Nutrition Examination Survey
Age-, Sex-, and Race-Adjusted Prevalence and ORs of Select Cardiovascular Disease Risk Factors Between the First and Fourth Quartiles of Serum 25(OH)D Levels Data From the Third National Health and Nutrition Examination Survey (15088 participants >20 yrs) Martins, D. et al. Arch Intern Med 2007;167: Copyright restrictions may apply.
D Levels. Data From the Third National Health and Nutrition Examination Survey. (15088 participants >20 yrs) Martins, D. et al. Arch Intern Med 2007;167: Copyright restrictions may apply.")
18
Vit D and Metabolic Syndrome
Relation of 25-hydroxyvitamin D and PTH levels with metabolic syndrome among US adults JP Reis, D. von Muhlen, ER Miller European Journal of Endocrinology, 159, 2008 We have strong evidences of hypovitaminosis D in MetS patients, independent of Ca intake, PTH, BMI, or renal function The potential mechanisms to explain the protective effect of vitamin D against MetS is based on the effect on glucose homeostasis (insulin resistance, β cell function): Vit D increases insulin receptor capacity and responsiveness for glucose transport
: Vit D increases insulin receptor capacity and responsiveness for glucose transport.")
19
Diabetes and Vitamin D Vitamin D metabolism and actions
Epidemiology of hypovitaminosis D Association of low Vitamin D status and chronic diseases Association of low vitamin D and diabetes: epidemiological evidence, pathophysiological plausibility, efficacy of interventions

20
Association between type 1 diabetes mellitus and risk of hip fracture in case-control and cohort studies. Association between type 1 diabetes mellitus and risk of hip fracture in case-control and cohort studies. Each square shows the study-specific relative risk (RR) estimate (the size of the square reflects the study-specific statistical weight, that is, the inverse of the variance), and the horizontal line shows the related 95 confidence interval (CI). The diamond shows the summary RR estimate, and its width represents the corresponding 95% CI. All statistical tests were two-sided. Statistical heterogeneity between studies was assessed with Cochran's Q test. Janghorbani M et al. Am. J. Epidemiol. 2007;166: American Journal of Epidemiology © The Author Published by the Johns Hopkins Bloomberg School of Public Health. All rights reserved. For permissions, please
 estimate (the size of the square reflects the study-specific statistical weight, that is, the inverse of the variance), and the horizontal line shows the related 95 confidence interval (CI). The diamond shows the summary RR estimate, and its width represents the corresponding 95% CI. All statistical tests were two-sided. Statistical heterogeneity between studies was assessed with Cochran s Q test. Janghorbani M et al. Am. J. Epidemiol. 2007;166: American Journal of Epidemiology © The Author Published by the Johns Hopkins Bloomberg School of Public Health. All rights reserved. For permissions, please")
21
Association between type 2 diabetes mellitus and risk of hip fracture in case-control and cohort studies. Association between type 2 diabetes mellitus and risk of hip fracture in case-control and cohort studies. Each square shows the study-specific relative risk (RR) estimate (the size of the square reflects the study-specific statistical weight, that is, the inverse of the variance), and the horizontal line shows the related 95 confidence interval (CI). The diamond shows the summary RR estimate, and its width represents the corresponding 95% CI. All statistical tests were two-sided. Statistical heterogeneity between studies was assessed with Cochran's Q test. Janghorbani M et al. Am. J. Epidemiol. 2007;166: American Journal of Epidemiology © The Author Published by the Johns Hopkins Bloomberg School of Public Health. All rights reserved. For permissions, please
 estimate (the size of the square reflects the study-specific statistical weight, that is, the inverse of the variance), and the horizontal line shows the related 95 confidence interval (CI). The diamond shows the summary RR estimate, and its width represents the corresponding 95% CI. All statistical tests were two-sided. Statistical heterogeneity between studies was assessed with Cochran s Q test. Janghorbani M et al. Am. J. Epidemiol. 2007;166: American Journal of Epidemiology © The Author Published by the Johns Hopkins Bloomberg School of Public Health. All rights reserved. For permissions, please")
22
Bone Mineral Density (BMD) at the hip in subjects with diabetes type 1, diabetes type 2 and without diabetes P<0.05 P<0.005 L’osteopenia è stata inizialmente descritta nel ‘76 (NEJM) in adolescenti con diabete tipo 1, 50% dei quali aveva una ridotta BMD sia trabecolare che corticale dell’avambraccio e molti studi successivi hanno confermato questo risultato, come evidenziato in questo studio su circa 120 soggetti diabetici e circa 500 controlli. Al contrario che per il diabete tipo 1, però, in pazienti con D tipo 2 la BMD è risultata uguale o addiritura superiore a quella di controlli, anche in soggetti insulino-trattati. Questo studio arruolava solo soggetti che avevano sviluppato D tipo 1 o 2 dopo i 30 anni, tutti insulino-trattati. Gli autori concludono, quindi, che la bassa BMD nel D. tipo 1 è legata, oltre che probabilmente al mancato raggiungimento del picco di massa ossea, anche alla perdita di massa ossea dopo che il picco è stato raggiunto. Tuominen et al, Diabetes Care, 1999
 in adolescenti con diabete tipo 1, 50% dei quali aveva una ridotta BMD sia trabecolare che corticale dell’avambraccio e molti studi successivi hanno confermato questo risultato, come evidenziato in questo studio su circa 120 soggetti diabetici e circa 500 controlli. Al contrario che per il diabete tipo 1, però, in pazienti con D tipo 2 la BMD è risultata uguale o addiritura superiore a quella di controlli, anche in soggetti insulino-trattati. Questo studio arruolava solo soggetti che avevano sviluppato D tipo 1 o 2 dopo i 30 anni, tutti insulino-trattati. Gli autori concludono, quindi, che la bassa BMD nel D. tipo 1 è legata, oltre che probabilmente al mancato raggiungimento del picco di massa ossea, anche alla perdita di massa ossea dopo che il picco è stato raggiunto. Tuominen et al, Diabetes Care,")
23
Bone quality vs bone density
Diabetes is associated with a decrease in bone strength that is not reflected in the measurement of BMD Despite having a higher bone density, on average, patients with T2D have a higher risk of fractures. Other factors, associated with frailty and falls, including age, physical activity and BMI do not account for the association between T2D and fracture.

24
Has Fat a Protective Role for the Skeleton? “Pros & Cons”
Decreased Vit D bioavailability Rosen CJ et al. Nature, 2006

25
Role of vitamin D in the pathogenesis of type 2 Diabetes Mellitus
Evidence exists that Vit D influences B cell insulin secretion through a rise in intracellular calcium concentration (indirect effect) and by a direct effect demonstrated by the presence of VDreceptors on the β cells and their ability to express 1-α hydroxylase and therefore activate 25 OH(D) to 1,25 OH(D). Moreover, vit D has an immune-modulation action and protects the β cells by inflammatory cytochines Palomer et al, Diabetes, Obesity and Metabolism, 2008
 and by a direct effect demonstrated by the presence of VDreceptors on the β cells and their ability to express 1-α hydroxylase and therefore activate 25 OH(D) to 1,25 OH(D). Moreover, vit D has an immune-modulation action and protects the β cells by inflammatory cytochines. Palomer et al, Diabetes, Obesity and Metabolism,")
26
Serum Vitamin D and Subsequent Occurrence of Type 2 Diabetes
Two nested case-control studies, collected by the Finnish Mobile Clinic in 1973–1980. During a follow-up period of 22 years, 412 incident type 2 diabetes cases occurred, and 986 controls were selected by individual matching. Study- and sex-specific and pooled age-adjusted relative odds of type 2 diabetes comparing highest and lowest quartiles of serum vitamin D. The black squares and horizontal lines represent study- and sex-specific ORs and 95% CIs, respectively. The area of the black squares reflects the study- and sex-specific weight (inverse of the standard error). The diamond represents the pooled ORs and 95% CI. The vertical dashed line represents the pooled relative risk. Knekt: Epidemiology, Volume 19(5).September
. The diamond represents the pooled ORs and 95% CI. The vertical dashed line represents the pooled relative risk. Knekt: Epidemiology, Volume 19(5).September")
27
Pittas AG et al, Diabetes Care, 33(9) 2010
 2010")
28
Levels of vitamin D and cardiometabolic disorders:
Systematic review and meta-analysis Parker J et al, Maturitas, 2009

29
Factors Contributing to Low Vitamin D Levels in Diabetes
Penckofer et al, 2008

31
Diabetes Care, 33(10), 2010
, 2010")
32
Vitamin D and diabetes Vitamin D and diabetes
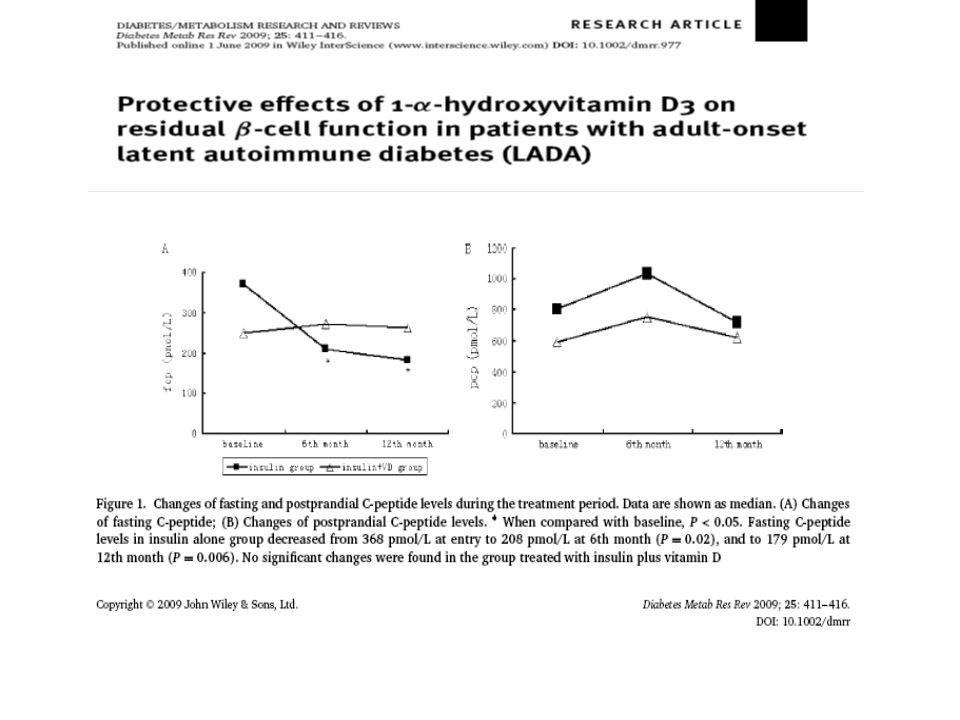
The metabolically active form of vitamin D, 1,25(OH)2D3, and its analogues have been shown to have effects on the major players involved in the pathogenesis of type 1 and type 2 diabetes. Beta cell function has been shown to be improved by 1,25(OH)2D3 in vitro and in vivo, and the avoidance of vitamin D deficiency is essential for normal beta cell function. In NOD mice, 1,25(OH)2D3 protects against insulitis, diabetes and disease recurrence after islet transplantation, primarily through immunomodulatory effects. Review Vitamin D and diabetes C. Mathieu et al, Diabetologia, 2005
2D3, and its analogues have been shown to have effects on the major players involved in the pathogenesis of type 1 and type 2 diabetes. Beta cell function has been shown to be improved by 1,25(OH)2D3 in vitro and in vivo, and the avoidance of vitamin D deficiency is essential for normal beta cell function. In NOD mice, 1,25(OH)2D3 protects against insulitis, diabetes and disease recurrence after islet transplantation, primarily through immunomodulatory effects. Review. Vitamin D and diabetes. C. Mathieu et al, Diabetologia,")
34
Evidence of the efficacy of Vit D supplementation
Vitamin D improves endothelial function in patients with Type 2 diabetes mellitus and low vitamin D levels J. A. Sugden, J. I. Davies, M. D. Witham,et al DIABETIC Medicine, 2007 Daily consumption of vitamin D-or vitamin D + calcium fortified yogurt drink improved glycemic control in patients with type 2 diabetes: a randomized clinical trial Nikooyeh B, Neyestani TR, Farvid M et al AJCN, 2011 Vitamin D as an analgesic for patients with T2D and neuropathic pain Lee P, Chen R. Arch Intern Med 2008

35
Schematic representation of the multitude of other potential physiologic action of vitamin D for cardiovascular health, cancer prevention, regulation of immune function and decreased risk of autoimmune diseases Throughout evolution, sunlight-produced vitamin D in the skin has been critically important for health. Vitamin D, known as the sunshine vitamin, is actually a hormone. Once it is produced in the skin or ingested from the diet, it is converted sequentially in the liver and kidneys to its biologically active form 1,25-dihydroxyvitamin D. This hormone interacts with its receptor in the small intestine to increase the efficiency of intestinal calcium and phosphate absorption for the maintenance of the skeleton throughout life. Vitamin D deficiency during the first few years of life results in a flattened pelvis, making it difficult for childbirth. Vitamin D deficiency causes osteopenia and osteoporosis, increasing risk of fracture. Essentially, every tissue and cell in the body has a vitamin D receptor. Therefore, vitamin D deficiency has been linked to increased risk for preeclampsia, requiring a cesarean section for birthing, multiple sclerosis, rheumatoid arthritis, types I and II diabetes, heart disease, dementia, deadly cancers, and infectious diseases. Therefore, sensible sun exposure along with vitamin D supplementation of at least 2000 IU/d for adults and 1000 IU/d for children is essential to maximize their health. It is estimated that 1 billion people worldwide are vitamin D deficient or insufficient. Correcting and preventing this deficiency could have an enormous impact on reducing health costs worldwide. Holick, Am J Clin Nutr, 2004

36
November, 2010

38
Major challenges Measuring 25(OH)D
Techniques available Clinical reporting of circulating 25(OH)D concentrations Defining doses of Vitamin D supplements
D concentrations. Defining doses of Vitamin D supplements.")
39
Recommendations for clinical practice
Souberbielle JC et al, Autoimmunity reviews, 2010

40
Vitamin D3 is more potent than Vitamin D2 in humans
Heaney, R. P. et al. J Clin Endocrinol Metab 2011;96:E447-E452 Copyright ©2011 The Endocrine Society

41
Conclusions The role of Vitamin D in diabetes is not limited to the autoimmune form of diabetes The relationship between vitamin D and diabetes is complicated, involving various mechanisms not yet fully elucidated Clinical trials are required to identify individuals with or at risk of T2D that will most benefit from Vitamin D supplementation and the dose and formulation which would be most effective

Similar presentations