Download presentation
Presentation is loading. Please wait.

1
Preoperative Evaluation of Cardiac Patient for Noncardiac surgery
Dr Balaji Asegaonkar MD,DNB (Anaesthesia) Consultant cardiac anaesthesiologist Ozone Anaesthesia Group, Aurangabad.
 Consultant cardiac anaesthesiologist. Ozone Anaesthesia Group, Aurangabad.")
2
CASE 1 65 YR MALE ,HT SINCE 5 YRS,DM SINCE 5 YRS ON INSULIN AND IHD
ANGIOPLASTY DONE 10 MONTHS BACK WITH DRUG ELUTING STENTS ON DUAL ANTIPLATELATE AGENTS TO BE POSTED FOR TURP

3
CASE 2 70 YR MALE ,HYPERTENSIVE, DIABETIC & SEVERE OSTEOARTHRITIS.
SMOKER FOR LAST 30 YRS. TO BE POSTED FOR TKR

4
CASE 3 80 YRS MALE, HT, IHD- POST PLASTY, POOR EFFORT TOLERANCE
TO BE POSTED FOR CATARACT

5
Let’s face it… The surgical population is older, sicker, on more medications, and having more & more cardiac interventions. There is a subset of your patients for whom the patient, the surgeon, or you may have questions about cardiovascular risk.

6
So what do you do? Guess?…Argue?…Worry?…Refer everyone cardiological investigations OR do a thorough, focused exam. Followed by the individualized application of some authoritative guidelines… …for evaluation, risk stratification, and management… …and refer, delay, or cancel only when appropriate.

7
Authoritative guidelines…..?
Evidence based medicine. Based on research findings, expert opinion, and consensus . Cardiovascular authority, like American College of Cardiology/American Heart Association. Anaesthesiology authority, like ASA. I am not a cardiologist, nor do I play one on TV. The point is to learn as much as possible, act responsibly based on your own knowledge and the knowledge of experts, and get assistance when you need it.

8
Objectives: How to approach cardiac Patients. Risk stratification.
Modification of level of care. Discuss standard recommendation.

9
focused approach……… We are not cardiologists, We simply need to recognize when a cardiac condition might affect the patient’s response to anaesthesia, and what to do about it. We need to be: Thorough enough to find all significant problems (sensitivity). Focused enough to consider only significant problems (specificity).
. Focused enough to consider only significant problems (specificity).")
10
…and Stepwise Approach?
Thorough, focused cardiac evaluation ACC/AHA Guidelines for Perioperative Cardiovascular Evaluation for Noncardiac Surgery (2007). Indicated cardiac testing and consultation. Optimization of cardiovascular function in relation to the demands of the surgery and the anaesthesia.
. Indicated cardiac testing and consultation. Optimization of cardiovascular function in relation to the demands of the surgery and the anaesthesia.")
11
The courage is knowledge of how to fear what ought to be feared & how not to fear what ought not to be feared.

12
Applying Classification of Recommendations and Level of Evidence
Class I Benefit >>> Risk Procedure/ Treatment SHOULD be performed/ administered Class IIa Benefit >> Risk Additional studies with focused objectives needed IT IS REASONABLE to perform procedure/administer treatment Class IIb Benefit ≥ Risk Additional studies with broad objectives needed; Additional registry data would be helpful Procedure/Treatment MAY BE CONSIDERED Class III Risk ≥ Benefit No additional studies needed Procedure/Treatment should NOT be performed/administered SINCE IT IS NOT HELPFUL AND MAY BE HARMFUL Level of Evidence: Level A: Data derived from multiple randomized clinical trials or meta-analyses Multiple populations evaluated Level B: Data derived from a single randomized trial or nonrandomized studies Limited populations evaluated Level C: Only consensus of experts opinion, case studies, or standard of care Very limited populations evaluated

13
So, let’s start with … The Preop portion of the ACC/AHA Guidelines, which is based on your history and physical, plus indicated tests.

14
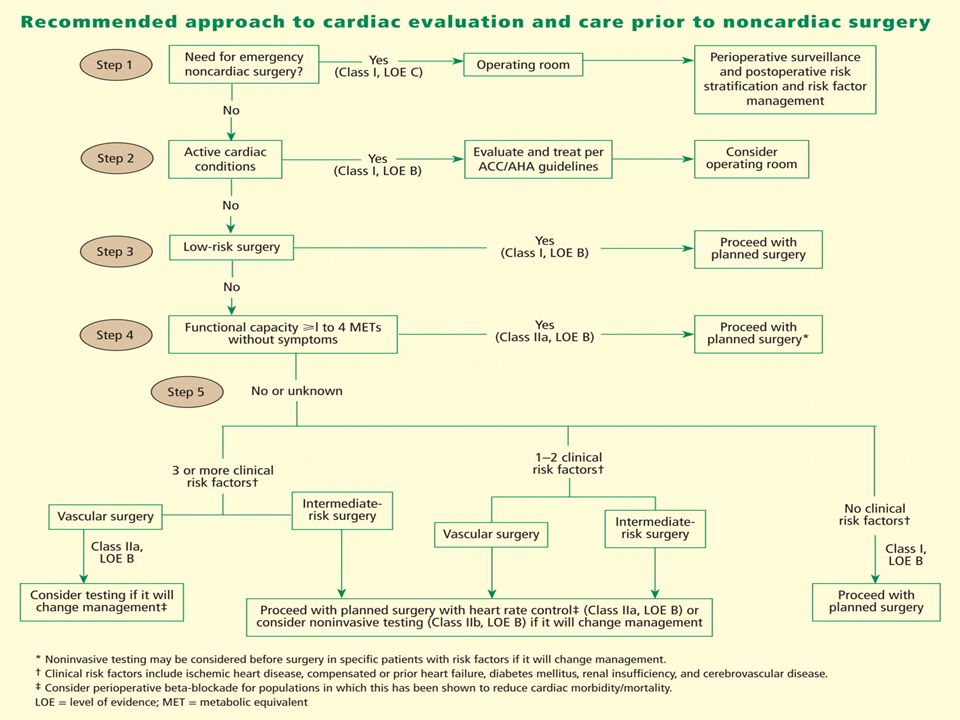
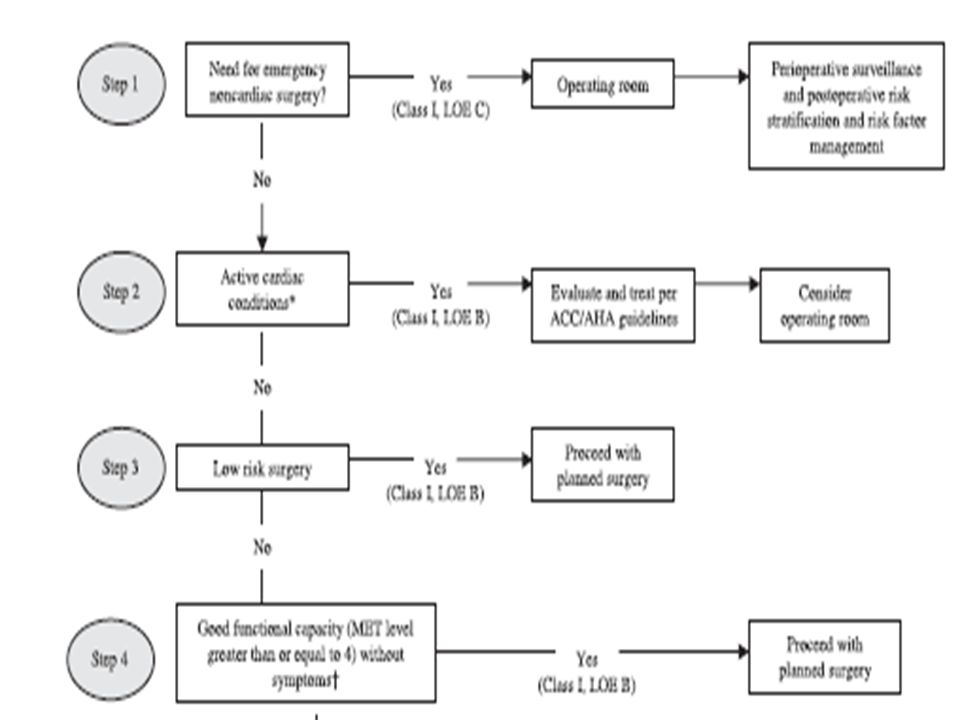
Guidelines : Stepwise approach
Need for surgery:Emergent vs Urgent/Elective. Clinical Risk Predictors: (Major, Intermediate, Minor). Functional capacity (Exercise tolerance).
. Functional capacity (Exercise tolerance).")
15
ACC/AHA Guidelines: Preop
Surgical Risk Predictors: (High, Intermediate, Low) Recent coronary revascularization or Evaluation.
 Recent coronary revascularization or Evaluation.")
16
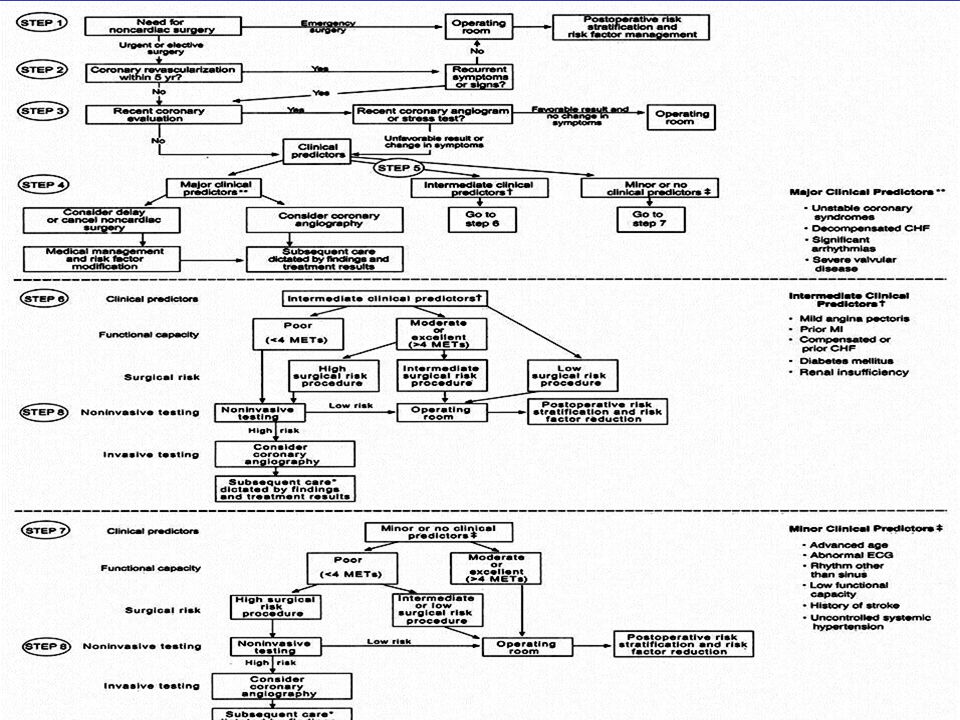
Major Clinical Risk Predictors
Unstable Coronary Syndromes: Recent MI (> 7 and < 30 days). Unstable angina (Canadian Class III-IV). Decompensated CHF. Significant Dysrhythmias. High-grade AV block. Symptomatic ventricular dysrhythmias. Supraventricular dysrhythmias with uncontrolled ventricular rate. Severe Valve Disease.
. Unstable angina (Canadian Class III-IV). Decompensated CHF. Significant Dysrhythmias. High-grade AV block. Symptomatic ventricular dysrhythmias. Supraventricular dysrhythmias with uncontrolled ventricular rate. Severe Valve Disease.")
17
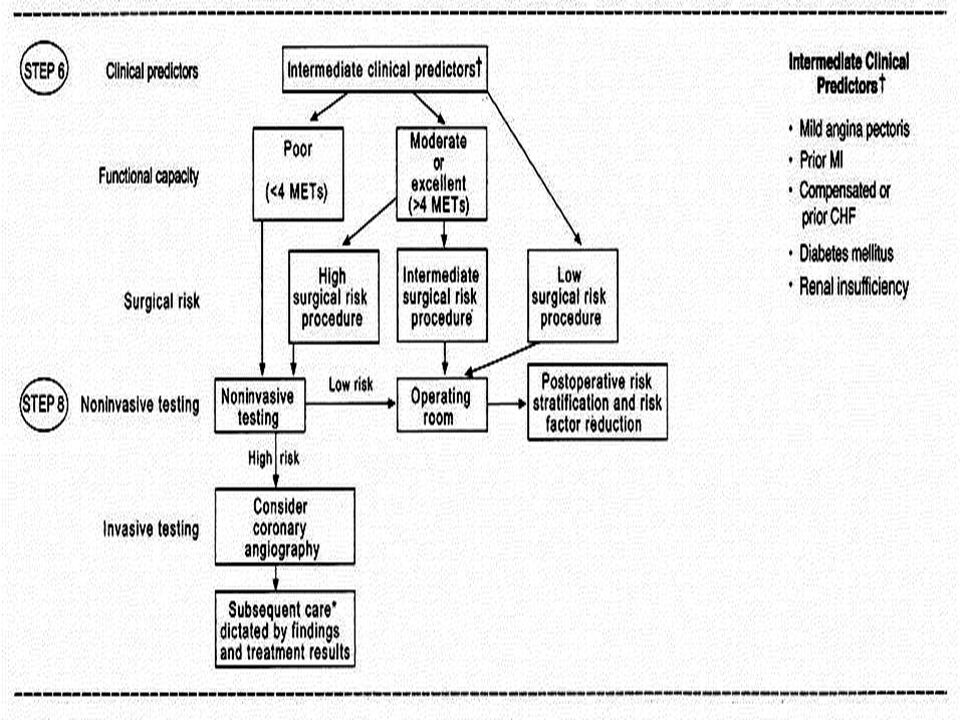
Intermediate Clinical Risk Predictors
Mild angina (Canadian Class I - II). Prior MI by history or pathological Q waves. Compensated or prior CHF. Diabetes, especially IDDM. Renal Insufficiency (creatinine > 2mg%).
. Prior MI by history or pathological Q waves. Compensated or prior CHF. Diabetes, especially IDDM. Renal Insufficiency (creatinine > 2mg%).")
18
Minor Clinical Risk Predictors
Advanced age. Abnormal ECG (LVH, LBBB, ST-T abnl). Rhythm other than sinus (e.g. a-fib). Low functional capacity (< 4 METs). Hx CVA. Uncontrolled HTN (>180 / >110). So, at some point someone is going to ask, “What’s Canadian Class Angina?”
. Rhythm other than sinus (e.g. a-fib). Low functional capacity (< 4 METs). Hx CVA. Uncontrolled HTN (>180 / >110). So, at some point someone is going to ask, What’s Canadian Class Angina")
19
Cardiac Functional Classification: Canadian Cardiovascular Society
No angina with ordinary physical activity . Angina with strenuous exertion. II. Slight limitation of ordinary activity. III. Marked limitation of ordinary activity. IV. Inability to carry on any physical activity without discomfort. Angina may be present at rest.

20
Functional Capacity = Exercise Tolerance
Major clinical risk predictors are sufficient alone to trigger further testing or intervention before pt posted for Sx. Intermediate and minor clinical risk predictors are subject to a second step: Evaluation of cardiovascular functional capacity, i.e., exercise tolerance.

21
Exercise Tolerance Angina or anginal equivalents (DOE, palpitations, fatigue)= Ischemic threshold. Point where metabolic demand > supply Metabolic equivalent (MET): MET = resting O2 consumption(VO2) = 3.5mL/kg/min Functional capacity in METs: Poor: < 4 Mod: 4-7: > 4 is the “tipping point”. Good: Excellent: > 10.
: 1 MET = resting O2 consumption(VO2) = 3.5mL/kg/min. Functional capacity in METs: Poor: < 4. Mod: 4-7: > 4 is the tipping point . Good: Excellent: > 10.")
22
Exercise Tolerance in METs
1 MET: Eat, dress, use the toilet. 2 METs: Household ambulation. 3 METs: Light housework Walk level ground 2-3 MPH. 4 METs: Walk up one flight stairs. Walk level ground 4 MPH. 4-10 METs: Run short distance. Scrub floors, move furniture. Moderate sports. >10 METs: Strenuous sports.

23
Surgical Risk Predictors
High (> 5% Cardiac Death/MI). Emergent major operation, espec. in elderly, Aortic and other major vascular Sx Peripheral vascular,Prolonged procedure. Intermediate (< 5%) Carotid endarterectomy, Head & neck Intraperitoneal, Intrathoracic, Prostate, Ortho Low (< 1%) Endoscopic, Superficial, Cataract, Breast
. Emergent major operation, espec. in elderly, Aortic and other major vascular Sx Peripheral vascular,Prolonged procedure. Intermediate (< 5%). Carotid endarterectomy, Head & neck Intraperitoneal, Intrathoracic, Prostate, Ortho. Low (< 1%). Endoscopic, Superficial, Cataract, Breast.")
25
Procedure Details : Angioplasty
Time since procedure. Which artery. Present medication. Symptoms benefits. Baseline ECG. Which stents.

26
DRUG ELUTING STENT ANTICACER DRUGS COATED.
SLOW RELEASE TILL 6 TO 8 MONTH. NO ENDOTHELIAZATION. LEAST CHANCE OF INSTENT THROMBOSIS ANTIPLATELETS

27
Post plasty :Noncardiac surgery

28
Treatment for patients requiring PCI who need subsequent surgery

29
Procedure Details : CABG
Time since procedure. Which arteries grafted & Type of conduit. Present medication. Symptoms benefits. Baseline ECG

30
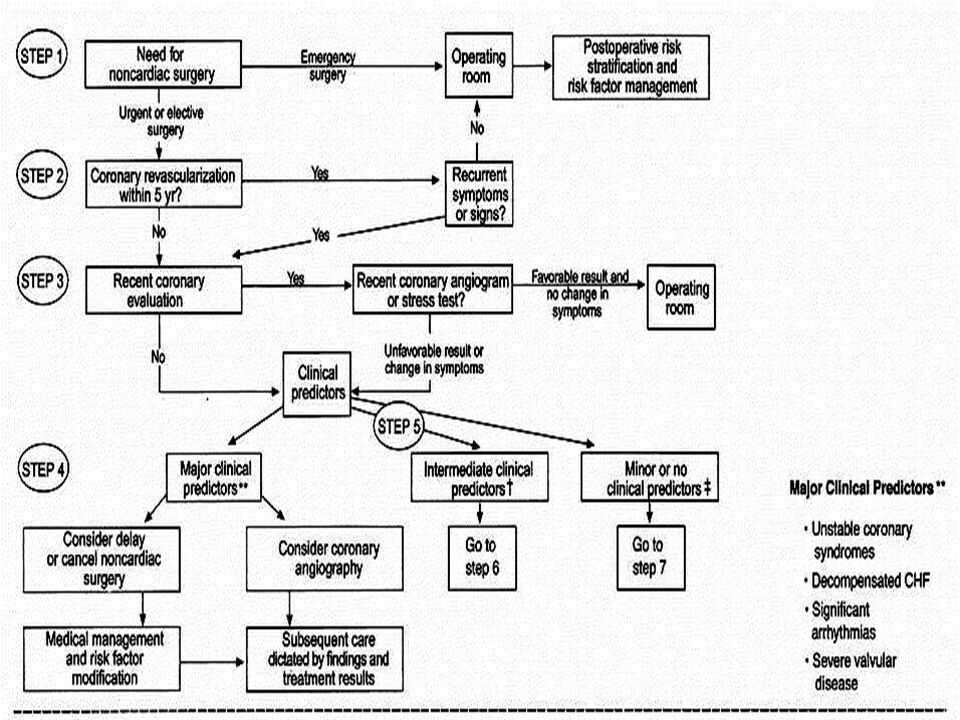
Recommended stepwise approach
How urgent noncardiac surgery is ? p/o risk stratification & assessment done. All these are Gr V cases.

31
Step 2 Has Pt undergone coronary revascularisation in past 5 yrs ?
If yes & Pt has no s/s of cardiac problem – further detail cardiac testing not required.

32
Step 3 If Pt has any coronary evaluation in past yrs – revealing no significant CAD ,if there is no aggravations of s/s –no further testing is needed.

33
Step 4 Does Pt have any major clinical predictors ?
Delay noncardiac surgery until problem has identified & treated.

34
Step 5 If Pt have intermediate clinical predictors.
Consider functional capacity & surgery specific risks. Decide accordingly weather further testing needed or not.

35
Step 6 Pt with intermediate predictor & mod to excellent functional capacity can undergo intermediate Sx. Pt with 2 or more intermediate predictor & poor functional capacity OR mod functional capacity but high risk Sx – further testing & evaluation needed.

36
Step 7 Noncardiac Sx safe in Pt with minor clinical predictor & mod to excellent functional capacity. Additional testing must for Pt with no clinical predictors but poor functional capacity & who are facing high risk Sx.

37
CASE 1 65 YR MALE ,HT SINCE 5 YRS,DM SINCE 5 YRS ON INSULIN AND IHD
ANGIOPLASTY DONE 10 MONTHS BACK WITH DRUG ELUTING STENTS TO BE POSTED FOR TURP

38
CASE 2 70 YR FEMALE ,HYPERTENSIVE & SEVERE OSTEOARTHRITIS.
CABG DONE 2 YRS BACK ON ANTIPLATE, ANTI HT & STATINS TO BE POSTED FOR TKR

39
CASE 3 80 YRS MALE, HT, IHD- POST PLASTY, POOR EFFORT TOLERANCE
TO BE POSTED FOR CATARACT

40
Thanks....!

43
Step 8 In documented CAD , if risk of coronary interventions or CABG exceeds proposed noncardiac Sx & if such Sx improves long term prognosis of Pt – noncardiac Sx should be done.

48
Summary from ACC / AHA Perioperative evaluation and mgmt of high-risk cardiac patients for noncardiac surgery requires careful teamwork and communication between patient, surgeon, anesthesiologist, physian or cardiologist. Indications for cardiac testing and treatments are the same as in the non-operative setting, and should clearly affect patient management. Factors include the urgency of surgery, patient-specific risk factors, and surgery-specific considerations.

49
Summary For many patients, noncardiac surgery represents their first opportunity for assessment of short- and long-term cardiac risk. The consultant best serves the patient by making recommendations aimed at lowering the immediate perioperative cardiac risk, as well as assessing the need for postoperative risk stratification and interventions directed to modify cardic risk factors. Future research should be directed at determining the value of routine prophylactic medical therapy vs. more extensive diagnostic testing and interventions.

50
Proposed Approach to the Management of Patients with Previous PCI Who Require Noncardiac Surgery
Balloon Bare-metal Drug-eluting angioplasty stent stent <365 days > days < days >365 days Time since PCI <14 days >14 days Delay for elective or Proceed to the Delay for elective or Proceed to the nonurgent surgery operation room nonurgent surgery operating room with aspirin with aspirin PCI, percutaneous coronary intervention

51
Proposed Treatment for Patients Requiring PCI Who Need Subsequent Surgery
Acute MI, H risk ACS, or H risk cardiac anatomy Stent & continue dual antiplatelet therapy Bleeding risk of surgery low Not low Timing of surgery 14-29 days days >365 days Bare-metal stent Balloon angioplasty Drug-eluting stent

52
Recommendations for Perioperative Beta-Blocker Therapy
Surgery No Clinical Risk Factors CAD or High Risk (1 or more clinical risk factors) Patients Currently Taking Beta Blockers Vascular Class llb, Level of Evidence: B Class lla, Level of Evidence: B Class 1, Level of Evidence: C Intermediate risk … Low risk
 Patients Currently Taking Beta Blockers. Vascular. Class llb, Level of Evidence: B. Class lla, Level of Evidence: B. Class 1, Level of Evidence: C. Intermediate risk. … Low risk.")
53
Recommendations for Statin Therapy
For patients currently taking statins and scheduled for noncardiac surgery, statins should be continued. For patients undergoing vascular surgery with or without clinical risk factors, statin use is reasonable. For patients with at least 1 clinical risk factor who are undergoing intermediate-risk procedures, statins may be considered. I IIa IIb III B

54
Happy Anaesthesia Day

58
Aims on evaluation Delay case for treatment of unstable symptoms.
Modification of intraoperative or postoperative (e.g. ICU) monitoring.
 monitoring.")
59
Aims on evaluation Modification of perioperative medical therapy.
Coronary or valve procedure before noncardiac surgery. Modification of location of care

60
Rest ECG: Indications Class I:Recent angina with intermed-high risk clinical predictors for intermed-high risk procedure. Class IIa: Asymptomatic diabetics. Class IIb: Prior coronary revascularization or cardiac hospital admission. Asymptomatic males > 45 or females > 55 with 2 CAD risk factors. Class III: Asymptomatic pts. For low-risk procedures

61
Rest ECG: Significant Findings
Path.Q waves (> 0.4s wide, or > 25% of R, in 2 contiguous leads): Size and extent predict LVEF, long term mortality. Horizontal or downsloping ST depression > 0.5mm, LVH with strain pattern (ST depression + TWI in I, II, III, AVL or AVF, V5, V6), LBBB with CAD predict increased perioperative risk and long term mortality. Significant dysrhythmias: High-grade AV block, symptomatic ventricular dysrhythmias, supraventricular dysrhythmias with uncontrolled rate.
: Size and extent predict LVEF, long term mortality. Horizontal or downsloping ST depression > 0.5mm, LVH with strain pattern (ST depression + TWI in I, II, III, AVL or AVF, V5, V6), LBBB with CAD predict increased perioperative risk and long term mortality. Significant dysrhythmias: High-grade AV block, symptomatic ventricular dysrhythmias, supraventricular dysrhythmias with uncontrolled rate.")
62
Echocardiogram: Indications
Asymptomatic murmurs : Class I: Diastolic, continuous, holosystolic, mid & late systolic, III/VI murmurs. Class IIa: Murmur assoc with abnl cardiac palpation or auscultation, abnl ECG or CXR. Class III: II/VI midsystolic innocent murmur. Dx of “silent” AR or MR without murmur, to recommend endocarditis prophylaxis.

63
Echocardiogram: Indications
Symptomatic murmur: Class I: S/S of CHF, MI, syncope, infective endocarditis, thromboembolism Class IIA: S/S possibly non-cardiac. Class III: S/S non-cardiac dz with midsystolic “innocent” murmur

64
Stress Testing: ECG or Echo
Normal rest ECG → ECG stress, Abnl ECG → Echo Class I: Dx of intermediate probability CAD, Prognosis of CAD or s/p ACS, Eval of med tx. Proof of ischemia before revascularization. Class IIa: Evaluate exercise tolerance in unreliable historian. Class IIb: Dx of high or low probability CAD, Resting ST depression < 1mm, On digoxin, LVH by ECG, Dx of restenosis in high-risk asymptomatic . Class III: Resting pre-excitation or ST depression > 1mm, Routine screening. 28

65
Recommendations for CAG in Preop Evaluation
Class I: Patients With Suspected or Known CAD Evidence for high risk of adverse outcome based on noninvasive test results. Angina unresponsive to adequate medical therapy. Unstable angina, particularly when facing intermediate-risk* or high-risk* noncardiac surgery. Equivocal noninvasive test results in patients at high clinical risk undergoing high-risk* surgery. Class IIa Multiple markers of intermediate clinical risk and planned vascular surgery (noninvasive testing should be considered first). Moderate to large ischemia on noninvasive testing but without high-risk features and lower left ventricular ejection fraction. Nondiagnostic noninvasive test results in patients at intermediate clinical risk undergoing high-risk* noncardiac surgery. Urgent noncardiac surgery while convalescing from acute MI.
. Moderate to large ischemia on noninvasive testing but without high-risk features and lower left ventricular ejection fraction. Nondiagnostic noninvasive test results in patients at intermediate clinical risk undergoing high-risk* noncardiac surgery. Urgent noncardiac surgery while convalescing from acute MI.")
66
Recommendations for CAG in Preop Evaluation
Class IIb Perioperative MI. Medically stabilized class III or IV angina and planned low-risk or minor* surgery. Class III Low-risk* noncardiac surgery with known CAD and no high-risk results on noninvasive testing. Asymptomatic after coronary revascularization with excellent exercise capacity (greater than or equal to 7 METs). Mild stable angina with good left ventricular function and no high-risk noninvasive test results. Noncandidate for coronary revascularization owing to concomitant medical illness, severe left ventricular dysfunction (e.g., left ventricular ejection fraction less than 0.20), or refusal to consider revascularization. Candidate for liver, lung, or renal transplant less than 40 years old, as part of evaluation for transplantation, unless noninvasive testing reveals high risk for adverse outcome.
. Mild stable angina with good left ventricular function and no high-risk noninvasive test results. Noncandidate for coronary revascularization owing to concomitant medical illness, severe left ventricular dysfunction (e.g., left ventricular ejection fraction less than 0.20), or refusal to consider revascularization. Candidate for liver, lung, or renal transplant less than 40 years old, as part of evaluation for transplantation, unless noninvasive testing reveals high risk for adverse outcome.")
Similar presentations