Download presentation
Presentation is loading. Please wait.

1
Nutrition Module Notes Pediatric I – Second Year Rebecca Abiog-Castro, M.D. Rhodora Garcia de Leon, M.D Faculty of Medicine & Surgery, UST

2
Objectives of the Course
At the end of the course a Second Year Medical Student should be able: To discuss briefly the anatomy of the breast and physiology of lactation; To discuss the benefits of breastmilk and the benefits of breastfeeding to both infant and mother; To discuss the barriers on breastfeeding; To discuss the composition of mature breast-milk; To discuss the difference between breast-milk and cow’s milk;

3
Objectives of the Course
To discuss the steps to encourage Breast-feeding in the hospital: UNICEF / WHO Baby-Friendly; To discuss the features of complementary foods; To discuss the proper method to introduce complementary foods; To utilize the PSPGN Food Guide Pyramid for the prescription of the proper diet for infant & children; To classify the different breast-milk substitutes (infant formulas) and determine the indication/s for its use; To discuss the supplements for breastfed infants.
 and determine the indication/s for its use; To discuss the supplements for breastfed infants.")
4
Mother's milk is the best food a baby can have exclusively in the first 6 months of life; should be continued until two years and beyond.

6
Anatomy of Breast External structures: Internal structures
Cross section of alveolus

7
Breast Structure

8
Anatomy of the Breast

9
Palate Teat Tongue

10
Physiology of lactation Endocrine control
Three main phases of lactation 1) Mammogenesis or mammary growth 2) Lactogenesis or initiation of milk secretion: Stage I: wks before parturition Stage II: 2-3 days postpartum 3) Stage III of Lactogenesis or Galactopoiesis maintenance of milk secretion: das.
 Mammogenesis or mammary growth. 2) Lactogenesis or initiation of milk secretion: Stage I: 12 wks before parturition. Stage II: 2-3 days postpartum. 3) Stage III of Lactogenesis or Galactopoiesis maintenance of milk secretion: das.")
11
Three Main Phases of Lactation (hormonal)
Phase I - Mammogenesis Profound during pregnancy in preparation for lactation Placental lactogen, estrogen, progesterone Ductal Sprouting (estrogen), lobular formation (progesterone), Prolactin essential for complete gland growth 11 11
, lobular formation (progesterone), Prolactin essential for complete gland growth")
12
Hormones Involved in Mammary Growth
Phase I - Mammogenesis Hormones Involved in Mammary Growth Estrogens Progesterone GH Placental lactogens (PL) Prolactin Glucocorticoids GH and PL induce alveolar growth Steroids without GH and PL do not exert any effect
 Prolactin. Glucocorticoids. GH and PL induce alveolar growth. Steroids without GH and PL do not exert any effect.")
13
Phase I - Mammogenesis INDUCTION OF GROWTH (Normal animals)
• Estrogens alone induce alveolar growth Larger than normal alveoli • Estrogen and progesterone induce normal growth

14
Phase II - LACTOGENESIS
INITIATION OF LACTATION At parturition the mammary gland switches from a growing non secretory tissue to a secreting, non-growing tissue Change is endocrine mediated

15
Three Main Phases of Lactation (hormonal)
Phase II - Lactogenesis (initiation of milk): Stage I: starts 12 wks before delivery Gathering of all substrates for milk production Stage II: starts 2-3 days postpartum Milk secretion is copious 15 15
: Stage I: starts 12 wks before delivery. Gathering of all substrates for milk production. Stage II: starts 2-3 days postpartum. Milk secretion is copious")
16
ENDOCRINE REGULATION OF LACTOGENESIS
Endocrine Patterns Related to Parturition

17
Endocrine Control of Lactation
Milk Production Reflex: Prolactin is a key lactogenic hormone, stimulating initial alveolar milk production Milk Ejection Reflex: Oxytocin contracts the myoepithelial; cells, forcing milk from the alveoli into the ducts and sinuses where it is removed by the infant

18
ENDOCRINE REGULATION OF LACTOGENESIS
Effect of different hormones in the initiation of milk production Glucocorticoids Development of RER (rough endoplasmic reticulum) Prolactin Maturation of Golgi Secretory vesicles Responsible for milk secretion Progesterone Promotes mammary growth specially alveolar tissue Blocks epithelial secretion As it decreases, the block for lactogenesis is removed
 Prolactin. Maturation of Golgi. Secretory vesicles. Responsible for milk secretion. Progesterone. Promotes mammary growth specially alveolar tissue. Blocks epithelial secretion. As it decreases, the block for lactogenesis is removed.")
19
Effect of different hormones in the initiation of milk production
MAMMARY GROWTH SLOWS DOWN Most hormones involved in growth have been removed Progesterone CL has regressed and placenta is removed Estrogens Feto-placental unit no longer available Placental lactogens Placenta was expelled After parturition mammary growth slows down because most growth promoting hormones are no longer available

20
Phase III – Galactopoiesis maintenance of Breastmilk Secretion
Stage III of Lactogenesis or Galactopoiesis Maintenance of milk secretion From days Mature milk is established Prolactin and Oxytocin essential for effective maintenance of milk supply 20 20

21
MAINTENANCE OF LACTOGENESIS (Galactopoiesis)
Hormones in charge of supporting continuous milk production Responsibility of prolactin and growth hormone Supported by thyroid, parathyroid and adrenal glands through adequate metabolic function

22
Autocrine Control of Lactation
Influence of of Local Factors Acting on the Breasts It is not just the level of maternal hormones, but the efficiency of milk removal that governs the volume product in each breast A protein factor called feedback inhibitor of lactation (FIL) is secreted with other milk components into the alveolar lumen FIL, insensitive to prolactin milk production
 is secreted with other milk components into the alveolar lumen. FIL, insensitive to prolactin milk production.")
23
Autocrine Control of Lactation
FIL FIL FIL

24
Anatomy & Physiology: Milk production
Risk factors for delayed onset of lactation were: Stage II labor > 1 hr, Pre-pregnant maternal BMI > 27 kg/m2, Breastfeeding problems at day 3,and Being primiparous. Dewey et al, 2001

25
Anatomy & Physiology: Milk production
Factors associated with breastfeeding problems at day included: flat or inverted nipples at day 7, stage II labor > 1 hour, birthweight < 3601 gms, Pre-pregnant maternal BMI > 27 kg/m2 non breast milk fluids given in the first 48 hours of life Dewey, 2003

26
Breastmilk composition

27
Breast-milk Variations of Breastmilk Colostrum (1st 3-5 days of life)
Term breastmilk ( mother’s own: – 28 days) Pre-term Milk ( day days) Mature breastmilk ( >30 days) Drip breastmilk ( days postpartum)
 Pre-term Milk ( day days) Mature breastmilk ( >30 days) Drip breastmilk ( days postpartum)")
28
Colostrum First postpartum week’s mammary secretion consisting of yellowish (beta carotene) thick fluid; Has higher protein, lower fat and lactose; rich in Vitamin A (3x > BM), carotenoid (10x), vitamin E(3x); Protein content is rich in sIgA and immunologically competent mononuclear cells; Contains antioxidants which trap neutrophil-generated oxygen radicals.
, carotenoid (10x), vitamin E(3x); Protein content is rich in sIgA and immunologically competent mononuclear cells; Contains antioxidants which trap neutrophil-generated oxygen radicals.")
29
Concentration in MG /Day at Postpartum
Distribution of Immunoglobulins and other Soluble Substances in the Colostrum and Milk Delivered to the Breast-Fed Infant During a 24-Hour Period Soluble Product Concentration in MG /Day at Postpartum <1 week 1-2 weeks 3-4 weeks >4 weeks IgG 50 25 10 IgA* 5000 1000 IgM 70 30 15 Lysozyme 60 100 Lactoferrin 1500 2000 1200

30
Type of Volume Energy Protein CHO FAT NA Milk ml/d Kcal/100 ml G/100mL G/100 ml G/100 ml mmol/100ML Colostrum (1-5 d) Term D D Breastmilk (Mature>30 d)
 Term D D Breastmilk (Mature>30 d)")
31
Type of Volume ENERGY PROTEIN CHO FAT NA Milk (ml/d ) KCAL/ml G/100 ml G/100 ml G/100 ml mmol/100 ml Preterm D D D Drip BM Cow
 KCAL/ml G/100 ml G/100 ml G/100 ml mmol/100 ml Preterm D D D Drip BM Cow")
32
Calculated Nutrient Intakes Compared to Estimated Needs for LBW
Units/KG/D PreTerm Milk Week of Lactation Mature Milk Estimated Needs 1 2 4 Energy (KCAL) 120 Fluid Vol. (ML) 180 190 150 Protein (G) 3.9 3.4 2.8 2.4 3.5 Sodium (MMOL) 4.0 2.7 1.8 2.0 3.0 Calcium (MG) 53 46 42 47 Phosphorus (MG) 25 27 23 26 80-100
 120. Fluid Vol. (ML) Protein (G) Sodium (MMOL) Calcium (MG) Phosphorus (MG)")
33
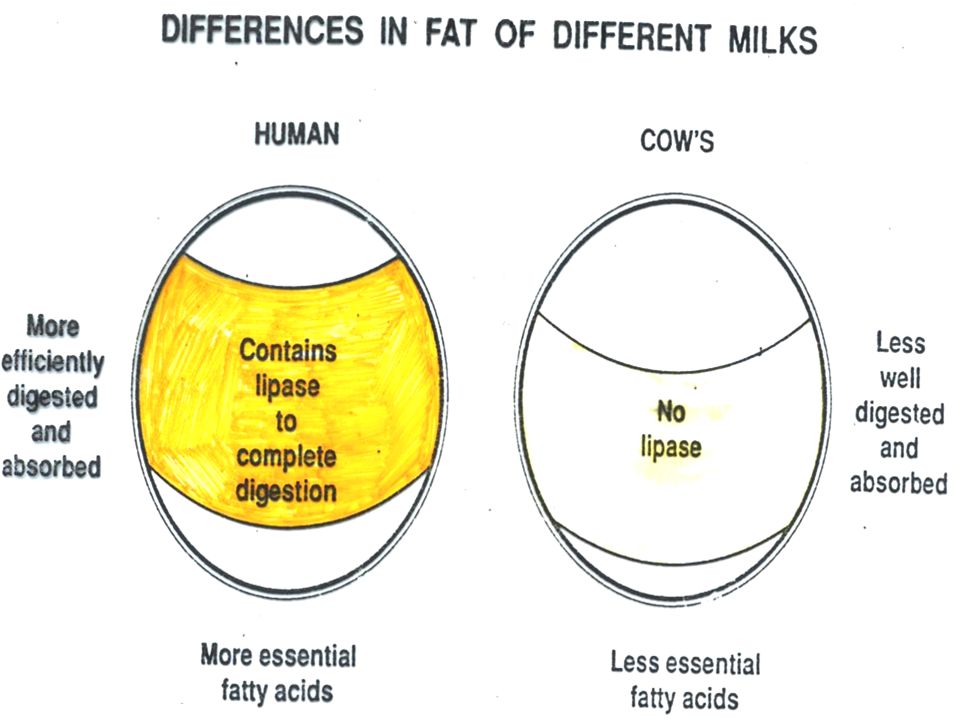
HUMAN COW’S Amino-acids Cystine Taurine Enough for growing brain
Not enough Fat Total Saturation of fatty acids Linoleic acid (essential) Cholesterol 4% (average) Enough unsaturated Enough 4% Too much saturated Lipase to digest fat Present None Lactose (sugar) 7% -- enough 3-4% - not enough Salts (mEq/l) Sodium Chloride Potassium 6.5 correct amount 12 correct amount 14 correct amount 25 too much 29 too much 35 too much
 Cholesterol. 4% (average) Enough unsaturated. Enough. 4% Too much saturated. Lipase to digest fat. Present. None. Lactose (sugar) 7% -- enough. 3-4% - not enough. Salts (mEq/l) Sodium. Chloride. Potassium. 6.5 correct amount. 12 correct amount. 14 correct amount. 25 too much. 29 too much. 35 too much.")
34
HUMAN COW’S Minerals (mg/l) Calcium Phosphate 350 correct amount
1,400 too much 900 too much Iron Small amount Well absorbed Enough Poorly absorbed Not enough Vitamins Water No extra needed Extra needed

35
Nutrients in human and animal milk
Cow Goat Fat Protein Lactose HUMAN COW GOAT BUFFALO

38
Composition Iron Not affected by maternal iron status and dietary iron supplements Higher absorption: 50% : HM 10% : unfortified cow’s milk 4% : fortified cow’s milk

40
Minerals in human milk are largely protein bound and balanced which enhanvces bioavailability.
Independent of the mother’s iron status, a term NB with adequate iron stores and utilizes little dietary iron before 4-6 months. Iron in breastmilk is readily absorbed, no need to give supplement. Preterm may need supplement because they kack iron stores. Flouride in human milk is not abundant. Addition is nescessary when the fluid level is <0.3ppm – give baby suplement of 0.25mg of flouride is required. The level in water is 0.7 to 1.2 ppm. Excess flouride may damage teeth in the earlt stages of development.

41
VITAMIN CONTENT Vitamin Human Cow’s A Enough even in 2nd year
2 X in colostrum In case of deficiency give supplement to mother Less (x 1/2) B Group Plenty Even more C Enough Less (x 1/5) May need supplement if fed artificially D Less K Usually enough More in Colostrum More Vitamin K is given one time to newborn as there is only a small amount in breastmilk and it takes time for the intestinal flora to produce adequate amount of Vit K.
 B Group. Plenty. Even more. C. Enough. Less (x 1/5) May need supplement if fed artificially. D. Less. K. Usually enough. More in Colostrum. More. Vitamin K is given one time to newborn as there is only a small amount in breastmilk and it takes time for the intestinal flora to produce adequate amount of Vit K.")
42
Comparison of Human Milk and Cow’s Milk
Bacteria contamination None Likely Anti-infective Substances Antibodies Leucocytes Lactoferrin Bifidus factor Not active Protein - Total - Casein - Lactalbumen 1% 0.5% 4% too much 3% too much

43
Supplements for Breastfed Infants
The following supplementation is generally recommended: Vitamin K supplement in the immediate postpartum period. 400 IU of Vitamin D Breastfeeding women should continue taking prenatal vitamins especially vitamin D, calcium and iron Complementary foods should be given once infants reach six months of age

44
Review Questions The part of breast responsible for milk secretion _________ under the influence of what hormone? ______ Two important reflexes that are needed for BM secretion? ________ Which part of the breast is milk stored? ________ Hormone secreted during BF which can reduce BF________ Major source of protein in BM ______

45
Benefits of Breastmilk / Breastfeeding to Infants and Mothers

46
Benefits of Breastmilk
Enhances Cognitive Development Protective: Both for baby and mother Cheap & Free: Benefits the Economy Safe

47
Benefits of Breastmilk: Infant
Enhances Cognitive Development Docosohexanoic Acid (DHA) Lactose ‘Skin to skin’ Contact and ‘face to face’ position
 Lactose. ‘Skin to skin’ Contact and ‘face to face’ position.")
48
Benefits of Breastmilk: Infant
DHA (Docosohexanoic Acid): Fatty acid derived from Linolenic Acid Only found in breastmilk in consistent level Important substance for the myelin sheath of nerve fibers Vital nutrient for the growth and development of brain tissue and good vision Researches showed that it is this substance that enhances cognitive development
: Fatty acid derived from Linolenic Acid. Only found in breastmilk in consistent level. Important substance for the myelin sheath of nerve fibers. Vital nutrient for the growth and development of brain tissue and good vision. Researches showed that it is this substance that enhances cognitive development.")
49
Benefits of Breastmilk: Infant
Lactose Predominant carbohydrate of breastmilk Disaccharide consisting of glucose and galactose Galactose combines with lipid to form a valuable nutrient, galactose-lipid, for brain tissue development

50
Benefits of Breastmilk: Infant
‘Skin to skin’ contact & ‘Face to Face’ position Enhances the cognitive and educational development of children as each feeding time is a learning opportunity for mother and child

51
Benefits of Breastmilk: Infant
Breastmilk is Protective Protective properties of BM is divided into two: Humoral factors: Consists of the 5 immunoglobulins (antibodies): IgA, s IgA, IgG, Ig E, Ig D, Ig M Cellular factors: White Blood cells: Neutrophils Lymphocytes Epithelial cells Macrophages
: IgA, s IgA, IgG, Ig E, Ig D, Ig M. Cellular factors: White Blood cells: Neutrophils. Lymphocytes. Epithelial cells. Macrophages.")
52
52

53
Benefits of Breastmilk: Infant
Breastmilk is Protective White Blood Cells Bacterial killer Highest concentration of WBC occurs in the 1st few days of lactation > a million/ml Colostrum (1-5 days post-natal): Contains 105 – 5 x 106 WBC / ml
: Contains 105 – 5 x 106 WBC / ml.")
54
Benefits of Breastmilk: Infant
Breastmilk is Protective Bifidus Factor: Enhances the growth of Lactobacillus bifidus preventing growth of pathogenic bacteria Lactoferrin: Binds iron thus preventing the growth of iron-dependent bacteria

55
Host Resistance Factors in BM
Non-immunoglobulin components: Oligosaccharides Mucin Fatty acids

56
Anti-infective Properties
Benefits of Breastmilk: Infant Anti-infective Properties IgA, IgM, IgG: immunoglobulins that guard the gut against infective bacteria Bifidus factor: stimulates bifido-bacteria, which fight against pathogenic bacteria Lactoferrin: binds iron away from bacteria Macrophages: phagocytosis of infective bacteria B12 binding protein: removes B12 from bacteria

59
Antiviral Factors in Human Milk
Shown, in vitro, to be active against: Effect of Heat Secretory IgA Poliovirus types 1, 2, 3. Coxsackie types A9, B3, B5, Echovirus types 6, 9. Semliki Forest Virus Ross River Virus Rotavirus Cytomegalovirus Reovirus type 3 Rubella virus Herpes simplex virus, Mumps virus Influenza virus Respiratory syncytial virus Stable at 56°C for 30 mins.; Some loss (0 – 30%) at 62.5 °C for 30 mins; destroyed by boiling 59
 at 62.5 °C for 30 mins; destroyed by boiling. 59.")
60
Benefits of Breastmilk: Infant
Enhanced immune response to immunizations Polio Tetanus Diptheria Haemophilus influenza

61
Protection Against Infection
Reduces risk and severity of infectious illness among infants diarrhea otitis media lower respiratory infections bacteremia bacterial meningitis necrotizing enterocolitis infant botulism urinary tract disease sudden infant death syndrome (SIDS) Colic wheezing
 Colic. wheezing.")
62
Antibacterial Properties found in human milk
62

63
Shown, in vitro, to be active against:
Factor Shown, in vitro, to be active against: Effect of Heat Secretory IgA E. Coli (also pili and capsular antigens) C. Tetani C. Diphtheriae K. pneumoniae Salmonella (6 groups) Shigella (2 groups) Streptococcus, S. mutans, S. sanguis, S. mitis, S. salivarius, S. pneumoniae, C. burnetti, H. influenzae E. coli enterotoxin, V. Cholerae enterotoxin C. difficile toxins H. Influenzae capsule Stable at 56°C for 30 min; some loss (0-30%) at 62.5°C for 30 min; destroyed by boiling IgM, IgG V. Cholerae lipopolysaccharide; E. coli IgM destroyed and IgG decreased by a third at 62.5°C for 30 min 63
 C. Tetani. C. Diphtheriae. K. pneumoniae. Salmonella (6 groups) Shigella (2 groups) Streptococcus, S. mutans, S. sanguis, S. mitis, S. salivarius, S. pneumoniae, C. burnetti, H. influenzae. E. coli enterotoxin, V. Cholerae enterotoxin. C. difficile toxins. H. Influenzae capsule. Stable at 56°C for 30 min; some loss (0-30%) at 62.5°C for 30 min; destroyed by boiling. IgM, IgG. V. Cholerae lipopolysaccharide; E. coli. IgM destroyed and IgG decreased by a third at 62.5°C for 30 min. 63.")
64
Shown, in vitro, to be active against:
Factor Shown, in vitro, to be active against: Effect of Heat IgD Bifidobacterium bifidum growth z factor E. Coli Enterobacteriacea, enteric pathogens Stable to boiling Factor binding proteins (zinc, vitamin B12, folate) Dependent E. coli Destroyed by boiling Complement C1-C9 (mainly C3 and C4) Effect not known Destroyed by heating at 56°C for 30 min Lactoferrin Two-thirds destroyed at 62.5°C for 30 min; essentially destroyed by boiling for 15 min 64
 Dependent E. coli. Destroyed by boiling. Complement C1-C9 (mainly C3 and C4) Effect not known. Destroyed by heating at 56°C for 30 min. Lactoferrin. Two-thirds destroyed at 62.5°C for 30 min; essentially destroyed by boiling for 15 min. 64.")
65
Shown, in vitro, to be active against:
Factor Shown, in vitro, to be active against: Effect of Heat Lactoperoxidase Streptococcus, Pseudomonas, E. coli, S. typhimurium Destroyed by boiling Lysozyme E. coli, Salmonella, Micrococcus lysodeikticus Some loss (0-23%) at 62.5°C for 30 min; essentially destroyed by boiling for 15 min Unidentified factors S. aureus, C. difficile toxin B Stable at autoclaving; stable at 56°C for 30 min Carbohydrate E. coli enterotoxin Stable at 85°C for 30 min Lipid S. Aureus Stable at boiling Ganglioside (GMI like) E. Coli enterotoxin, V. cholerae enterotoxin Stable to boiling 65
 at 62.5°C for 30 min; essentially destroyed by boiling for 15 min. Unidentified factors. S. aureus, C. difficile toxin B. Stable at autoclaving; stable at 56°C for 30 min. Carbohydrate. E. coli enterotoxin. Stable at 85°C for 30 min. Lipid. S. Aureus. Stable at boiling. Ganglioside (GMI like) E. Coli enterotoxin, V. cholerae enterotoxin. Stable to boiling. 65.")
66
Types of Breast milk Foremilk Hindmilk

67
Protective Factors in BM
Non-immunoglobulin components: Non-specific factors: Bifidus factor Resistance factor (Anti-staphylococcal factor) Anti-viral factor Anti-protozoal factors (bile-salt stimulated lipase) Enzymes: Lysozyme, lipoprotein lipase
 Anti-viral factor. Anti-protozoal factors (bile-salt stimulated lipase) Enzymes: Lysozyme, lipoprotein lipase.")
68
Protective Factors in BM
Anti-inflammatory properties: BM is poor initiators and mediators of inflammation (complement system, fibrinolytic, coagulation system) but rich in anti-inflammatory agents (sIGA, lysozyme); Provides good mucosal barrier (growth factors) prevents attachment of bacteria & antigen;
 but rich in anti-inflammatory agents (sIGA, lysozyme); Provides good mucosal barrier (growth factors) prevents attachment of bacteria & antigen;")
69
Benefits of Breastmilk: Infants
Maternal HIV Maternal-to-Child Viral Transmission (MTCT): Breastfeeding vs Formula feeding: Prevalence of MTCT at 24 months: Breastfeeding (BF): % Formula-feeding (FF): 20.5% Mortality rate: BF: 24.4% FF: 20.0% Nduati R. et al. JAMA 2000
: Breastfeeding vs Formula feeding: Prevalence of MTCT at 24 months: Breastfeeding (BF): 36.7% Formula-feeding (FF): 20.5% Mortality rate: BF: 24.4% FF: 20.0% Nduati R. et al. JAMA")
70
Benefits of Breastmilk: Infant
Breastfeeding and premature infants: Premature infants fed their mother's milk were found to have decreased incidences of sepsis, meningitis, and necrotizing enterocolitis

73
Benefits of Breastmilk: Safe
Breastmilk is sterile free of contamination whereas powdered infant formula maybe contaminated Weir reported an outbreak of Enterobacter Sakazakii in US based NICU due to contaminated infant formula CMAJ Van Acker et al reported 12 infants developed NEC; 2 died attributed to E. Sakazakii derived from contaminated infant formula JClin Microbiol

74
Benefits of Breastmilk: Safe
Breastmilk is sterile free of contamination whereas powdered infant formula maybe contaminated Weir reported an outbreak of Enterobacter Sakazakii in US based NICU due to contaminated infant formula CMAJ Van Acker et al reported 12 infants developed NEC; 2 died attributed to E. Sakazakii derived from contaminated infant formula JClin Microbiol

75
Benefits of Breastmilk: Safe
Joint FAO/WHO Workshop on Enterobacter Sakazakii and other Microorganisms in Powdered Infant formula February 2004 Recommendations: Guidelines should be developed for the preparation, use and handling of infant formula to decrease the risk of infection Make use of Enterobacteriaceae rather than coliform testing as an indicator of hygienic control

76
Benefits of Breastfeeding: Mothers
Prevents Obesity Early return to pre-pregnancy weight

77
Benefits of Breastfeeding: Mothers
Breast Cancer “Meta-Analysis on the Protective Effect of BF on Breast Cancer”. Labbock et al. Ped Clin North Am., 2001 Feb Eleven studies were evaluated Results: RR: to 0.85 for 1st 3-6 months of BF RR: to 0.72 for > 2 years RR: for > 6 years Conclusion: Clear and consistent protective effect of BF on breast cancer have been found in all studies

78
Benefits of Breastfeeding: Mothers
Ovarian Cancer “Breastfeeding and Risk to Ovarian Cancer” Rosenblatt 1993: 20-25% decrease in risk for cancer for women who breastfed for at least 2 months Risch et al 1993 & Gwinn 1990: Showed the protective effect of lactation (RR 0.79 per year of lactation; 0.6 respectively) Shoham 1994: 50% decrease in risk for ovarian cancer
 Shoham 1994: 50% decrease in risk for ovarian cancer.")
79
Benefits of Breastfeeding: Economy
Family: Purchase of formula costs the average poor family (7,280.00/ month income) about P2,000.00 National Economy (NEDA): Milk companies import S57.5 M (P3.1 B) worth of infant formula Sell to people 7x cost (WHO) – P21.5 B or S405 B)
 about P2, National Economy (NEDA): Milk companies import S57.5 M (P3.1 B) worth of infant formula. Sell to people 7x cost (WHO) – P21.5 B or S405 B)")
80
Longer-term Health Outcomes: Maternal benefits
Reduces risk of chronic illness in childhood Some food allergies Type-1 insulin dependent diabetes Lymphoma Asthma Obesity

81
Steps to Encourage Breast-Feeding in the Hospital: UNICEF/WHO Baby-Friendly
HOSPITAL INITIATIVES Provide all pregnant women with information and counselling. Document the desire to breast-feed in the medical record. Document the method of feeding in the infant’s record. Place the newborn and mother skin- to-skin, and initiate breast-feeding within 1 hr of birth. Continue skin-to-skin contact at other times and encourage rooming-in. Assess breast-feeding and continue encouragement and teaching on each shift.

82
Steps to Encourage Breast-Feeding in the Hospital: UNICEF/WHO Baby-Friendly
MOTHERS TO LEARN Proper position and latch on Nutritive sucking and swallowing Milk production and release Frequency and feeding cues Expression of milk needed Assessment of the infant’s nutritional status When to contact the clinician

83
Steps to Encourage Breast-Feeding in the Hospital: UNICEF/WHO Baby-Friendly
ADDITIONAL INSTRUCTIONS Refer to lactation consultation if any concerns arise. Infants should go to the breast at least 8-12 times/24 hr, day and night. Avoid time limits on the breasts; offer both breasts at each feeding. Do not give sterile water, glucose, or formula unless indicated. If supplements are given, use cup feeding, a Haberman feeder, fingers, or syringe feedings. Avoid pacifiers in the newborn nursery except during painful procedures. Avoid anti-lactation drugs.

84
Review Questions What breast structure secretes breastmilk? What hormone is responsible for it? What are the 2 processes are responsible for breastmilk secretion & maintenance? Breastmilk is stored in what part of the breast? 3 phases of lactation? Hormone secreted during BF which could cause BM reduction if breast is not emptied completely.

85
6) What is the protein distribution of BM
6) What is the protein distribution of BM? What is the predominant protein component? 7) How much calories is lost per day when bf? 8) What are the 3 areas that must be addressed in BF based on the recommendation of WHO?
 What is the protein distribution of BM What is the predominant protein component 7) How much calories is lost per day when bf 8) What are the 3 areas that must be addressed in BF based on the recommendation of WHO")
86
Thank You and God bless

88
Breastmilk Substitutes Infant Milk Formulas

89
TYPES OF INFANT FORMULA
Pre-term Formula Catch-up Growth Formula Standard Infant Formula Whey Dominant ( 60%) Casein Dominant ( 60%) Follow-on (up) Formula Growing-up Formula Whole cow’s Milk Evaporated Milk
 Casein Dominant ( 60%) Follow-on (up) Formula. Growing-up Formula. Whole cow’s Milk. Evaporated Milk.")
90
Types of Infant Formulas
Special Formulas: Hydrolysates: Partial Hydrolysates Complete Hydrolysates Goats milk

91
Nutrient Sources: FOR INFANTS LESS THAN 2 YEARS
Three Indications for Use of Infant Formulas: As substitute ( or supplement) for human milk in infants whose mother choose not to breastfeed; As a substitute for human milk in infants for whom breastfeeding is medically contraindicated; As supplement for infants who do not gain weight appropriately.
 for human milk in infants whose mother choose not to breastfeed; As a substitute for human milk in infants for whom breastfeeding is medically contraindicated; As supplement for infants who do not gain weight appropriately.")
92
Nutrient Sources: < 2 Years of Age
PRETERM FORMULA: Prescribed for premature until they have reached weeks of gestation or gained 2 kilograms. When given beyond recommended age may cause hypercalcemia Special Features: Protein: Whey predominant formula at a level higher than breast milk & standard infant formula ( g/100ml.)
")
93
PRETERM FORMULA Pre-Aptamil (Milupa): 1:1 dilution
Enfalac Premature: 1:1 dilution Pre-Nan: :1 dilution S-26 LBW: :2 dilution

94
STANDARD INFANT FORMULA
Recommended during the first 6 –12 months of life; Extensively modified from what was originally produced by the cow; Very little difference between various brands Example: S-26, Enfalac, Nan, Similac, Mylac, Aptamil, Bonna, Nestogen

95
FOLLOW-UP FORMULA Liquid part of the weaning diet for infants & children 12 mos years of age; Distribution of calories and nutrients is in between standard infant formula and whole cow’s milk Protein is higher with the ratio of 20% whey and 80% casein Example: Promil, Nan 2, Gain, Milumil

96
COMPOSITION OF VARIOUS NUTRIENT SOURCES
BM COW A PREM FF-UP Energy kcal/100ml Protein G/100 ml Whey 60% 60% 20% Casein 40% 40% 80% Fat G/100 ml CHO G/100 ml CA mg/100 ml (75) P mg/100 ml (40) NA mmol/100 ml
 P mg/100 ml (40) NA mmol/100 ml")
97
GROWING –UP FORMULA: Product used for children above 2 years to 10 years Provides nutrient necessary as they undergo transition from infant to adult formulation. Protein is high ( 3 g/100 ml) from Sodium Casseinate and soya protein CHO contains a blend of cornstarch and sucrose with very minimal lactose
 from Sodium. Casseinate and soya protein. CHO contains a blend of cornstarch and sucrose with very minimal lactose.")
98
Growing-up Formulas Enfagrow (MJ): 1:1 dilution
Grow (Abbott): 1:2 dilution Lactum (MJ): 1:1 dilution Neslac (Nestle): 1:1 dilution Progress (Wyeth): 1:2 dilution
: 1:2 dilution. Lactum (MJ): 1:1 dilution. Neslac (Nestle): 1:1 dilution. Progress (Wyeth): 1:2 dilution.")
99
Whole Cow’s Milk Maybe given as supplement to a balanced diet from 12 months above; No modification done to suit the needs of infants &children Example: Alaska, Bear Brand,

100
Protein Hydrolysates Definition:
It refers to the product of an enzymatic degradation of protein to proteose, peptone, peptide-AA mix and finally free AA mix. Types: Partial Hydrolysate: Degradation of protein to big, medium size peptides less antigenicity; Complete Hydrolysate: Degradation of protein into small peptides and free AA.

101
For prophylaxis on high risk infants:
Protein Hydrolysates Partially Hydrolyzed Formula: For prophylaxis on high risk infants: FH of atopy, asthma, food allergy Preparation: Nan-HA Extensively Hydrolyzed Formula: For treatment of food allergy during infancy Preparations: Pregomin (Milupa) Pregistimil (MJ) Alfare (Nestle)
 Pregistimil (MJ) Alfare (Nestle)")
102
“Introduction of Complementary Food”

103
Features of Complementary Foods
Timely: Should be introduced by 6 months Adequate: Should provide sufficient energy, protein and micronutrients Safe: Hygienically stored and prepared and fed using clean utensils NOT bottles nor teat Properly fed: Meal frequency, feeding methods should be suitable for age (with fingers, spoon and fork, cups and bowls, guided or self-feeding)
")
106
Complementary Food (CF)
Definition: It refers to supplemental foods (milk & solid foods) given to infants when breastmilk is no longer adequate to sustain normal growth.
 given to infants when breastmilk is no longer adequate to sustain normal growth.")
107
Nursing Period (1st 6 months of life)
WHY should CF be given? Three Infant Feeding Periods: Nursing Period (1st 6 months of life) Transitional Period (6-10 months) Modified Adult Period ( >10 months)
 Transitional Period (6-10 months) Modified Adult Period ( >10 months)")
108
WHY should CF be given? Three Infant Feeding Periods:
Nursing Period (1st 6 months of life): Breastmilk or standard infant formula is sufficient to provide nutritional requirements for normal growth; MILK should be the ONLY source of nutrient.
: Breastmilk or standard infant formula is sufficient to provide nutritional requirements for normal growth; MILK should be the ONLY source of nutrient.")
109
Nursing Period (1st 6 months of life):
Digestive, mucosal barrier and renal functions are not well developed; (Zieger EE, J Pediatr, 1990) Neuro-developmental status: not fully developed !
 Neuro-developmental status: not fully developed !")
110
Nursing Period : (1st 6 months of life)
Addition of solid foods at this time breastmilk /milk consumption proportionally growth failure Stuff et al, J pediatr,1990

111
Transitional Period (6-10 months)
It is the transition from the nursing period to the adult modified period Milk (breastmilk / standard infant formula) is NO longer adequate to sustain the nutritional needs of growing infants
 is NO longer adequate to sustain the nutritional needs of growing infants.")
112
Transitional Period (6-10 mos)
Digestive, renal systems and taste are well developed; Skills needed for feeding are likewise fully developed.

113
Transitional Period ( 6-10 months)
FAILURE to offer supplemental foods at this time difficulty in accepting them later; Underwood BA,Acta Pediatr Scand Suppl, 1982

114
“Critical Learning Period” 6-15 months
6-15 months, “critical learning period” for feeding: chewing & swallowing coordination is being developed; FAILURE of infants to go through this process feeding problems: dependence to MILK as source of nutrient picky eaters / neophobic malnutrition (obesity/wasting ,anemia)
")
115
Modified Adult Period (>10 months)
Physiologic mechanisms have matured to near adult proficiency; Most of the nutrients MUST come from table foods with minimal alteration (cut into small pieces, bland); Taste ability & preferences have become established.
; Taste ability & preferences have become established.")
116
What kind of food would you give?
Scientific Rationale: “Critical Window” for introducing “lumpy” solid foods: if these are delayed beyond 10 mos increased risk of feeding difficulties later on Northstone et al, 2001 Ingestion of the types of foods depend on the neuromuscular development of infants

117
WHEN should CF be given? 6 months
Signals that indicate readiness of the infant for CF: Birth weight has doubled; Extrusion reflex has completely disappeared; Has good head and neck control; Sits up with support;

118
WHEN should CF be started?
Signals that indicate readiness of infant for CF: Opens mouth if wants food; turns head away when not interested anymore; Has good chewing & swallowing coordination; Consumes about 32 oz of milk and wants more; Breastfeeds > 10x and wants more

119
Art of Introducing Complementary Food
Introduce one new food at time to allow infant to get use to it; continue same food for 3-4 days before giving another food; Give very small amount of any new food at the beginning, 1-4 tsp;

120
Art of Introducing Complementary Food
Use thin puree consistency initially --> shift gradually to a more viscous calorie-dense food Mix foods with ones baby likes, to enhance acceptability and nutrient content Cereals +BM: Enhanced acceptance of cereal during weaning! Mennella et al, Pediatr Res, 1997

121
Art of Introducing Complementary Food
Once infant can sit with support at about 6 mos , give fluid (milk or water) using trainer’s cup; By 12 months of age milk should be given by the cup or glass; BOTTLES should be OUT by this time!
 using trainer’s cup; By 12 months of age milk should be given by the cup or glass; BOTTLES should be OUT by this time!")
122
Art of Introducing Complementary Food
Avoid adding salt and sugar When baby is able to chew at about months, gradually switch to finely chopped foods DO NOT continue soft smooth foods for too long Feeding Frequency: 6-8 months: meals a day 9-11 months: meals; snacks > 12 months: meals: snacks

123
Art of Introducing Complementary foods
By 12 months, most of the nutrient should come from table food (modified); infants have attained physiologic maturity of adult proficiency; Encourage infant to try new flavors as a variety of foods is important ! * FNRI-DOST, Nutrition Guidelines for Filipinos, 2000 * Pediatric Nutrition Handbook, 4th Edition AAP
; infants have attained physiologic maturity of adult proficiency; Encourage infant to try new flavors as a variety of foods is important ! * FNRI-DOST, Nutrition Guidelines for Filipinos, * Pediatric Nutrition Handbook, 4th Edition AAP.")
124
Harvard School of Public Health

125
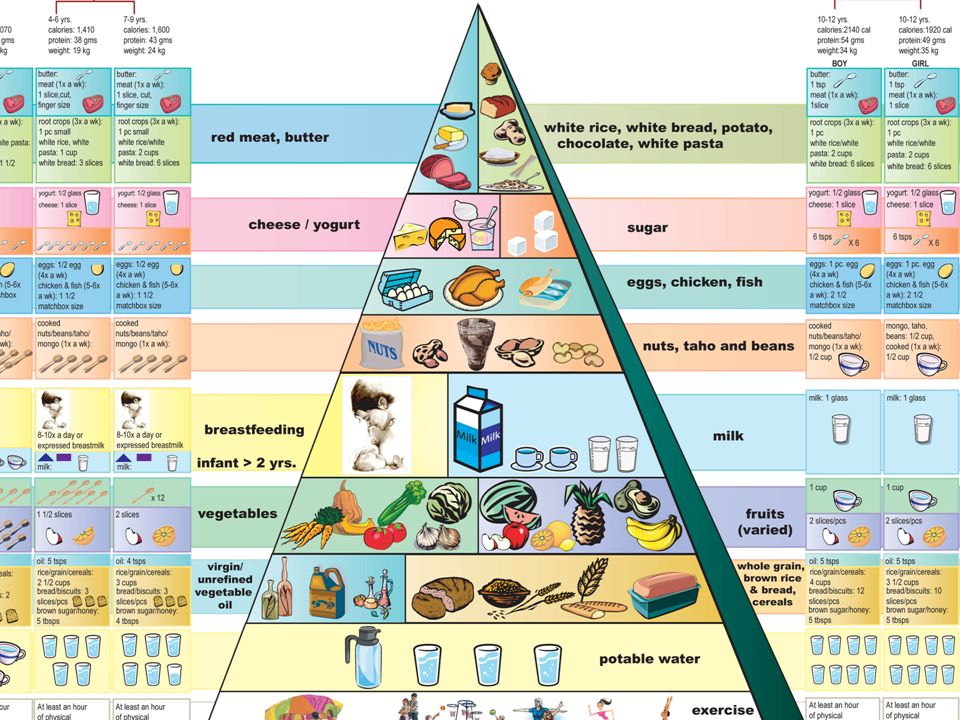
New Food Guide Pyramid US Department of Agriculture

127
Thank You and God bless

131
US Dept of Agriculture

132
Endocrine Control of Lactation

133
Endocrine Control of Lactation

Similar presentations

























 Office of Overseas Programming & Training Support (OPATS) Maternal and Newborn Health Training Package Session 8:>")






 impt. Human.>")